Radiographic Anatomy Knowledge of the radiographic appearances of




 and multidetector CT")






















































 the superior wall")





























- Slides: 91
Radiographic Anatomy
Knowledge of the radiographic appearances of normal structures is the foundation of radiologic interpretation
General Principles of Radiologic Evaluation The radiographic appearance of structures reflects the pattern of x-ray photon attenuation. Tissues that attenuate more photons appear more radiopaque (brighter) low-attenuation tissues appear radiolucent (darker)
On two-dimensional projections, the anatomic structures along the path of the beam are superimposed onto the same region on the image
CT images: three dimensions, without superimposition. Cone beam CT (CBCT) and multidetector CT (MDCT) are typically displayed as multiplanar reconstructions of the imaged structures in three orthogonal planes
CT images
it is important to evaluate all structures imaged. Often, disease is an incidental finding—that is, located typically in part of the image unrelated to the reason for which the image was made. Accordingly it is critical to systematically evaluate the entire image or imaged volume.
Teeth Hard Tissues Teeth are composed primarily of dentin, with an enamel cap over the coronal portion and a thin layer of cementum over the root surface
Enamel The enamel cap characteristically appears more radiopaque than the other tissues because it is the most dense naturally occurring substance in the body. Because it is about 96% mineral, it causes the greatest attenuation of x-ray photons. Its radiographic appearance is uniformly opaque and without evidence of the fine structure. Only the occlusal surface reflects the complex gross anatomy.
Dentin The dentin is about 75% mineralized, and because of its lower mineral content, its radiodensity is similar to that of bone. Dentin is homogeneous on radiographs because of its uniform morphologic features. The junction between enamel and dentin appears as a distinct interface that separates these two structures.
Cementum The thin layer of cementum on the root surface has a mineral content (50% to 60%) comparable to dentin. Cementum is not usually apparent radiographically because the contrast between it and dentin is so low and the cementum layer is so thin.
Cervical burnout On periapical and bitewing radiographs, diffuse radiolucent areas with ill-defined borders may be apparent radiographically on the mesial or distal aspects of teeth in the cervical regions between the edge of the enamel cap and the crest of the alveolar ridge.
Pulp The pulp of normal teeth is composed of soft tissue and consequently appears radiolucent. The chambers and root canals containing the pulp extend from the interior of the crown to the apices of the roots.
In normal, fully formed teeth, the pulp canal may be apparent, extending from the pulp chamber to the apex of the root. An apical foramen is usually recognizable.
In other normal teeth, the canal may appear constricted in the region of the apex and not discernible in the last 1 mm or so of its length.
In periapical radiographs, there may be superimposition of two pulp canals within the same root, for example, in the mesiobuccal root of the maxillary molar. Radiographs taken at different horizontal angulations may be needed to separate the images of these canals.
periapical radiographs provide adequate information for the initial evaluation of pulpal and periapical disease.
CBCT scans portray the three-dimensional morphology of the roots, pulp chambers, and pulp canals more accurately than intraoral radiographs
Individual canals are best identified on axial sections the length of the root and its exit through the apex are typically assessed on coronal and sagittal sections
In a mature tooth, the shape of the pulp chamber and canal may change. A gradual deposition of secondary dentin occurs with aging. This process begins apically, proceeds coronally, and may lead to pulp obliteration.
Trauma to the tooth (e. g. , from caries, a blow, restorations, attrition, or erosion) also may stimulate dentin production, leading to a reduction in size of the pulp chamber and canals.
Developing Teeth At the end of a developing tooth root, the pulp canal diverges, and the walls of the root rapidly taper to a knife edge. In the recess formed by the root walls and extending a short distance beyond is a small, rounded, radiolucent area in the trabecular bone, surrounded by a thin layer of cortical bone. This is the dental papilla bounded by its bony crypt.
When the tooth reaches maturity, the pulpal walls in the apical region begin to constrict and finally come into close apposition.
Supporting Dentoalveolar Structures Lamina Dura Alveolar Crest Periodontal Ligament Space Cancellous Bone Cortical Bone
Lamina Dura tooth sockets are bounded by a thin radiopaque layer of dense bone lamina dura (“hard layer”), is derived from its radiographic appearance only slightly thicker and with the same radiodensity as the trabeculae of cancellous bone that the x-ray beam passes tangentially through many times the thickness of the thin bony wall, which results in its observed attenuation (the eggshell effect)
Lamina Dura
The appearance of the lamina dura on radiographs may vary, depending on the direction of the x-ray beam relative to the cortical bone thickness The lamina dura is thicker and more radiopaque around the roots of teeth in heavy occlusion and thinner and less dense around teeth not subjected to occlusal function
When the x-ray beam is directed through a relatively long expanse of the structure, the lamina dura appears radiopaque and well defined. When the beam is directed more obliquely, the lamina dura appears more diffuse and may not be discernible.
Alveolar Crest The gingival margin of the alveolar process that extends between the teeth is apparent on radiographs as a radiopaque line.
The level of this bony crest is considered normal when it is 0. 5 to 2 mm apical to the cementoenamel junction of the adjacent teeth The alveolar crest may recede apically with age and show marked resorption with periodontal disease
In the anterior region, the crest is reduced to only a point of bone between the closeset incisors Posteriorly it is flat, aligned parallel with and slightly below a line connecting the cementoenamel junctions of the adjacent teeth
The crest of the bone is continuous with the lamina dura and forms a sharp angle with it. Rounding of these sharp junctions is indicative of periodontal disease.
Periodontal Ligament Space radiolucent space between the tooth root and the lamina dura
The PDL width varies between individuals, from tooth to tooth in the same individual and even from location to location around one tooth
When the x-ray beam is directed so that two convexities of a root surface appear on a film, a double PDL space is seen
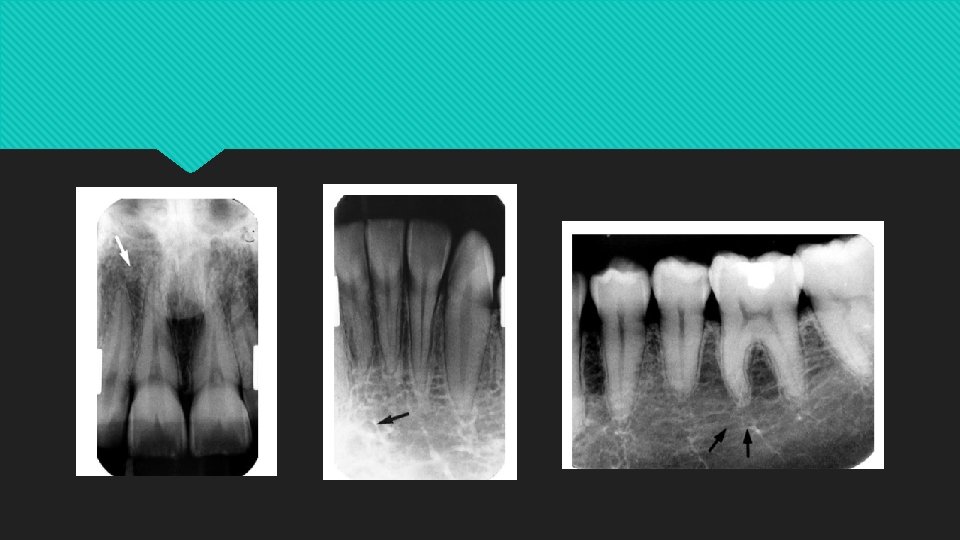
Cancellous Bone trabecular bone or spongiosa between the cortical plates in both jaws thin radiopaque plates and rods (trabeculae) surrounding many small radiolucent pockets of marrow
The trabeculae in the anterior maxilla are typically thin and numerous, forming a fine, granular, dense pattern and the marrow spaces are consequently small and relatively numerous In the posterior maxilla, the trabecular pattern is usually quite similar to the pattern in the anterior maxilla, although the marrow spaces may be slightly larger.
In the anterior mandible, the trabeculae are thicker than in the maxilla, resulting in a coarser pattern. with trabecular plates that are oriented more horizontally. The trabecular plates are also fewer than in the maxilla, and the marrow spaces are correspondingly larger In the posterior mandible, the periradicular trabeculae and marrow spaces may be similar to those in the anterior mandible but are usually larger The trabecular plates are also oriented mainly horizontally in this region
Cortical Bone Buccal and lingual cortical plates of the mandible and maxilla do not cast a discernible image on periapical, bitewing and panoramic radiographs. on CBCT images, best visualized on the axial, coronal, or cross-sectional images Cortical bone has higher mineral content than the adjacent cancellous bone, and appears more radiopaque
Maxilla and Midfacial Bones The maxilla comprises a pyramidal-shaped body and four processes—alveolar, palatine, zygomatic, and frontal.
Intermaxillary Suture The alveolar and palatine processes articulate in the midline to form the intermaxillary suture between the central incisors. On intraoral periapical radiographs this suture appears as a thin radiolucent line in the midline between the two portions of the premaxilla
The suture is limited by two parallel radiopaque borders of thin cortical bone on each side of the maxilla. The radiolucent region is usually of uniform width. The adjacent cortical margins may be either smooth or slightly irregular.
Anterior Nasal Spine on periapical radiographs of the maxillary central incisors Located in the midline, it lies approximately 1. 5 to 2 cm above the alveolar crest, usually at or just below the junction of the inferior end of the nasal septum and the inferior outline of the nasal aperture
It is radiopaque because of its bony composition and is usually V-shaped
Nasal Aperture and Nasal Cavity radiolucent image may be apparent on intraoral radiographs of the maxillary teeth especially in central incisor projections
On maxillary incisor periapical views, the inferior border of the fossa aperture appears as a radiopaque line extending bilaterally away from the base of the anterior nasal spin
The relatively radiopaque nasal septum is seen arising in the midline from the anterior nasal spine the septum frequently deviates slightly from the midline, and its plate of bone (the vomer) is curved.
Nasal Conchae and Nasal Turbinates The lateral walls contain thin bony projections called conchae. The conchae plus their mucosal covering are called turbinates There are three nasal turbinates—superior, middle, and inferior—which define spaces termed superior, middle, and inferior meati
Pneumatization of the concha is termed concha bullosa and is a common variant with a reported frequency of 14% to 53%
Nasal Floor and Hard Palate On periapical radiographs, the floor of the nasal aperture and a small segment of the nasal cavity are occasionally projected high onto a maxillary canine radiograph
In the posterior maxillary region, the floor of the nasal cavity may be seen in the region of the maxillary sinus. It may falsely convey the impression of a septum in the sinus or a limiting superior sinus wall.
Nasopalatine Canal and Incisive Foramen originates in the anterior floor of the nasal cavity and exits on the anterior maxilla as the incisive foramen, located in the midline on the anterior aspect of the palatine process immediately palatal to the maxillary central incisors
On intraoral and panoramic radiographs, the incisive foramen is usually projected between the roots and in the region of the middle and apical thirds of the central incisor
Lateral Fossa incisive fossa gentle depression in the maxilla near the apex of the lateral incisor diffusely radiolucent on periapical projections of this region, superimposed over the root of the lateral incisor
Nose The soft tissue of the tip of the nose is frequently seen in projections of the maxillary central and lateral incisors, superimposed over the roots of these teeth. The image of the nose has a uniform, slightly opaque appearance with a sharp border
Nasolacrimal Canal The nasal and maxillary bones form the nasolacrimal canal on periapical radiographs in the region above the apex of the canine, especially when a steep vertical angulation is used
usually seen on maxillary occlusal projections region of the molars
Paranasal Sinuses maxillary, frontal, and sphenoid sinuses and ethmoid air cells Only the maxillary sinuses are visualized on periapical radiographs
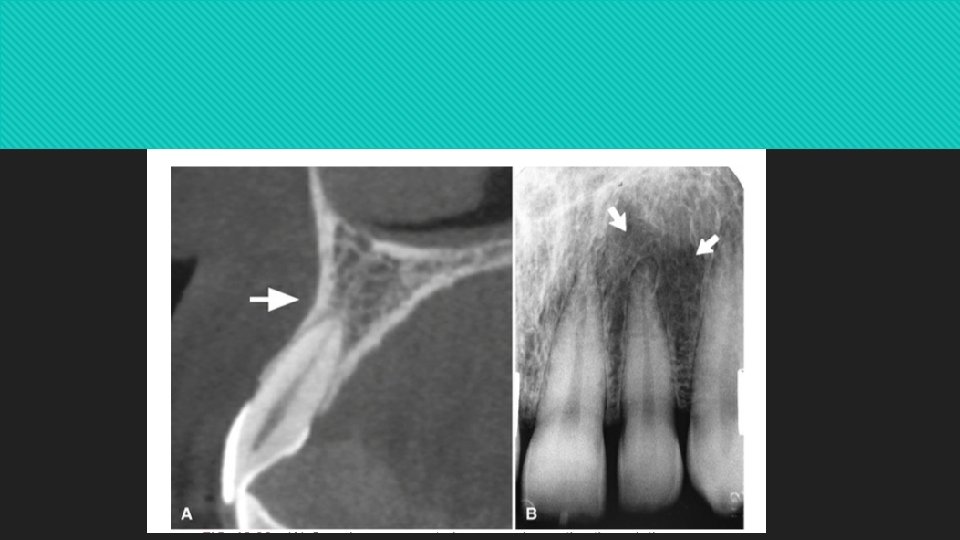
Maxillary Sinus The largest of the paranasal sinuse three sides: (1) the superior wall forming the floor of the orbit, (2) the anterior wall extending above the premolars, and (3) the posterior wall bulging above the molar teeth and maxillary tuberosity
Periapical radiographs show the inferior portion of the maxillary sinus. The maxillary sinus floor is a thin layer of cortical bone and appears as a thin radiopaque line.
on periapical radiographs of the canine, the floors of the sinus and nasal cavity are superimposed and seen crossing one another, forming an inverted “Y” in the area
. In response to a loss of function (associated with the loss of posterior teeth), the sinus may expand farther into the alveolar bone, occasionally extending to the alveolar ridge
Often one or several radiopaque lines traverse the image of the maxillary sinus. These opaque lines are called septa
Zygomatic Process and Zygoma On periapical radiographs, the zygomatic process appears as a U-shaped radiopaque line with its open end directed superiorly. The enclosed rounded end is projected in the apical region of the first and second molars
The inferior border of the zygoma extends posteriorly from the inferior border of the zygomatic process of the maxilla to the zygomatic process of the temporal bone uniform radiopacity over the apices of the molars
Nasolabial Fold slight radiopacity frequently traverses periapical radiographs of the premolar region
Pterygoid Plates The medial and lateral pterygoid plates lie immediately posterior to the maxilla. single radiopaque homogeneous shadow without any evidence of trabeculation
Extending inferiorly from the medial pterygoid plate is the hamular process which on close inspection can show trabeculae.
Mandible
Symphysis a radiolucent line through the midline of the jaw between the images of the forming deciduous central incisors
Genial Tubercles mental spine on the lingual surface of the mandible slightly above the inferior border and in the midline They attach the genioglossus muscles (at the superior tubercles) and the geniohyoid muscles (at the inferior tubercles) to the mandible
They are well visualized on mandibular occlusal radiographs as one or more small projection
Lingual Foramen 96% to 100% of individuals, located in the region of the genial tubercles a single round radiolucent canal with a well-defined opaque border lying in the midline below the level of the apices of the incisors.
Mental Ridge On periapical radiographs of the mandibular central incisors, two radiopaque lines sweeping bilaterally forward and upward toward the midline
Mental Fossa a depression on the labial aspect of the mandible extending laterally from the midline and above the mental ridge.
Mental Foramen the anterior limit of the inferior dental canal that is apparent on periapical radiographs the wall of the foramen consists of cortical bone round, oblong, slit-like, or very irregular and partially or completely corticated
Inferior Alveolar Canal dark linear shadow with thin radiopaque superior and inferior borders
Nutrient Canals on mandibular periapical radiographs running vertically from the inferior dental canal directly to the apex of a tooth or into the interdental space between the mandibular incisors
Mylohyoid Ridge internal oblique ridge On a periapical radiograph, its image runs diagonally downward and forward from the area of the third molars to the premolar region at approximately the level of the apices of the posterior teeth
Submandibular Gland Fossa On the lingual surface of the mandibular body, immediately below the mylohyoid ridge in the molar area, there is frequently a depression in the bone a radiolucent area with the sparse trabecular pattern characteristic of the region
External Oblique Ridge anterior border of the mandibular ramus a radiopaque line of varying width, density, and length
Inferior Border of the Mandible dense, broad, radiopaque band of bone
Coronoid Process on periapical radiographs of the maxillary molar region as a triangular radiopacity, with its apex directed superiorly and anteriorly, superimposed on the region of the third molar
Restorative Materials depending principally on their atomic number and also influenced by their thickness and density
Silver amalgam Gold
calcium hydroxide base Gutta-percha
Silver point porcelain restorations
Orthodontic appliances