Pediatric Endocrinology 2007 Merrily Poth M D Professor





 DECREASED BLOOD PRESSURE/BLOOD VOLUME")





 n n n WATER RESTRICTION (CAREFULLY) NPO AFTER MIDNIGHT WEIGH")













 Acne Body")
 n n PREMATURE THELARCHE-ONLY SEEN IN GIRLS PREMATURE")
 n")


















 n n n Unlike the situation in girls-LH alone")







")




















































 SURGERY I")
















 n n Effect of exercise Interaction of exercise, diet, and")













 n n If you are unable to eat, you can")









 Ovary Wolffian Ducts")
 Di-Hydro-Testosterone Androgen Receptor (X q 11 -12) Virilization of")





 n n ARE THERE PALPABLE TESTES IN THE SCROTUM? IS THE BABY")
 n n n GENDER ASSIGNMENT SHOULD BE MADE EXPEDITIOUSLY, BUT NOT FRIVOLOUSLY.")








 Congenital adrenal hyperplasia")






 n ON REVIEW OF HER HISTORYJANICE GREW AT THE 90 -95%")














 with enlarged clitoris was also noted to be")

- Slides: 198
Pediatric Endocrinology 2007 Merrily Poth, M. D. Professor Pediatrics and neuroscience USUHS Bethesda, MD
Pediatric Endocrinology Purpose of these talks is to review clinical endocrinology, in part in to prepare for pediatric board exams. I will emphasize areas targeted in past in board questions. I will also emphasize facts that will help you in your practices, outlining the fundamentals of how to diagnose, when to refer and when to reassure
Caveats n n n Not completely comprehensive. Not a substitute for in-depth consultation. Clinically up-to-date, but not emphasizing newer areas of molecular medicine and genetics.
Principles of Endocrinology n n Hormones-chemical compounds secreted into blood stream and transported to distant site-where they react with specific receptors. Feedback loops-in order to maintain homeostasis, each hormone system has method of sensing need for secretion and altering this up or down.
POSTERIOR PITUITARY CONNECTED TO THE HYPOTHALAMUS BY NERVES SECRETES ANTI-DIURETIC HORMONE AND OXYTOCIN Each hormone is made and secreted in associated with a specific physin.
n n SECRETION OF VASOPRESSIN IS STIMULATED BY HYPERNATREMIA (HYPEROSMOLARITY) DECREASED BLOOD PRESSURE/BLOOD VOLUME ALSO STIMULUS, BUT TAKES GREATER DEFICIT
Vasopressin n Binds to vasopressin receptors in renal tubule opening channel to water In absence of vasopressin cannot concentrate urine Resultant disease called “diabetes insipidus”
DIABETES INSIPIDUS n n n PRESENTATION DEPENDS ON AGE OF PATIENT IN INFANT PRESENTS WITH FTT, LOW GRADE FEVER WITHOUT SOURCE, POOR FEEDING IN OLDER CHILD PRESENTS WITH POLYURIA AND POLYDYPSIA
PATIENT n n 5 YO BOY PRESENTS WITH POLYURIA AND POLYURIA UP AT NIGHT TO DRINK AND URINATE 3 x PER NIGHT Sudden onset of symptoms APPEARS “OBSESSED” WITH WATER
CRITICAL QUESTIONS n WHAT DOES HE DRINK? • WATER VS JUICE- When offered a sweet drink does he prefer water? • Does he wake at night to drink water? SUDDEN VS GRADUAL ONSET
EVAULATION FOR DI n n n FIRST MORNING VOID SPECIFIC GRAVITY-IF GREATER THAN 1. 008 THE DIAGNOSIS IS HIGHLY UNLIKELY SERUM ELECTROLYTES AND GLUCOSE (Diabetes mellitus is much more common than DI) IF ALLOWED FREE ACCESS TO WATER WILL MAINTAIN SERUM SODIUM AT HIGH END OF NORMAL
EVALUATION FOR DI (CONT) n n n WATER RESTRICTION (CAREFULLY) NPO AFTER MIDNIGHT WEIGH EVENING BEFORE AND Q 2 HOURS during test STRICTLY MONITOR URINE OUTPUT AND TEST SPECIFIC GRAVITY OF ALL URINE IF SPECIFIC GRAVITY INCREASE ABOVE 1008 -NEGATIVE DIAGNOSIS
Diagnosis of DI IF WEIGHT LOSS GREATER THAN 5% AND URINE SPEC GRAV DOESN’T RISE, AND URINE OUTPUT CONTINUES AT SAME RATE WITHOUT INTAKE. IF APPEARS NOT TO BE ABLE TO CONCENTRATE URINE NEED TO GIVE DDAVP AND DOCUMENT THAT SPECIFIC GRAVITY OF URINE INCREASES MEASURE SERUM VASOPRESSIN WHEN SODIUM INCREASED-This is most “fool proof measure.
DIABETES INSIPIDUS n n IF DIAGNOSIS CONFIRMED AND PT RESPONDS TO EXOGENOUS VASOPRESSIN NEED TO EVALUATE FOR PITUITARY OR HYPOTHALAMIC PATHOLOGY IF EVALUATION NEGATIVE REPEAT IN 6 MONTHS ALSO NEED TO EVALUATE FOR STATUS OF ANTERIOR PITUITARY HORMONES • GH, ACTH, LH, FSH AND TSH
PATIENT n n 5 YO BOY PRESENTS WITH POLYURIA AND POLYURIA UP AT NIGHT TO DRINK AND URINATE 3 x PER NIGHT Sudden onset of symptoms APPEARS “OBSESSED” WITH WATER
To diagnose this child as having diabetes insipidus which of the following is true. n n A. He must have a elevated serum sodium at baseline. B. He must awaken at night to drink water. C. He must be growing normally. D. His first morning urine can have a specific activity of over 1. 010
Review of DI n n Cannot concentrate urine. Will usually drink water sufficient to maintain high normal serum sodium if allowed to. Treatment is DDAVP, either nasal or oral preparation. Treated or untreated, the important issue is free access to water, and if not able to drink, replacing output, cc for cc.
ANTERIOR PITUITARY n n Anterior pituitary is connected to the hypothalamus by blood vessels (the hypothalamic portal system) Releasing factors and other controlling substances travel to pituitary thru this portal system
ANTERIOR PITUITARY n n Deficiencies of anterior pituitary hormones can occur singly or in combination Puberty is a good example of a process that is under control of the hypothalamic-pituitary axis and a good example of active feedback loops.
HYPOTHALAMIC-PITUITARYGONADAL AXIS
The Hypothalamic-pituitary-gonadal axis Gn. RH Gonadal steroids LH, FSH
Normal Puberty n n Activity of the HPG axis occurs first prenatally, then during the first few months of life, then again at the time of normal puberty. First event in puberty is pulsing of LHRH by the hypothalamus, which begins to mature the pituitary gland, which then secretes LH and FSH.
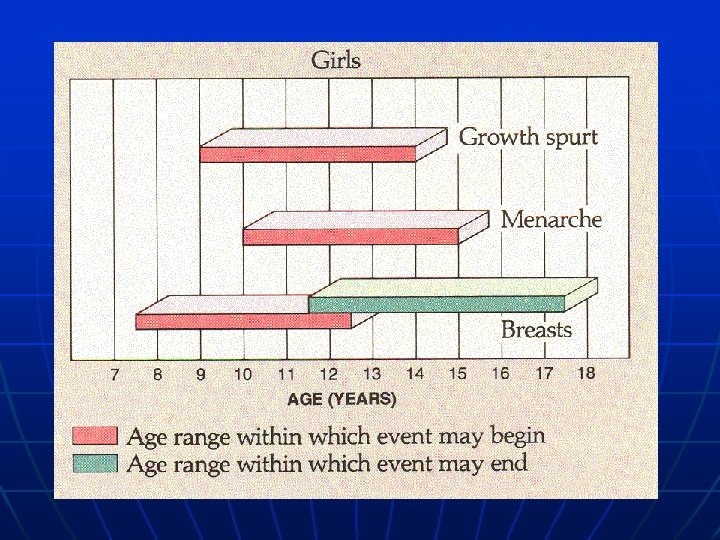
PUBERTY in GIRLS n n n NORMAL PUBERTY BEGINS AT MEAN AGE OF 11 FIRST SIGN OF PUBERTYBREASTS IN 85% AND PUBIC HAIR IN 15% MENARCHE USUALLY APPROX 2 YEARS AFTER THELARCHE
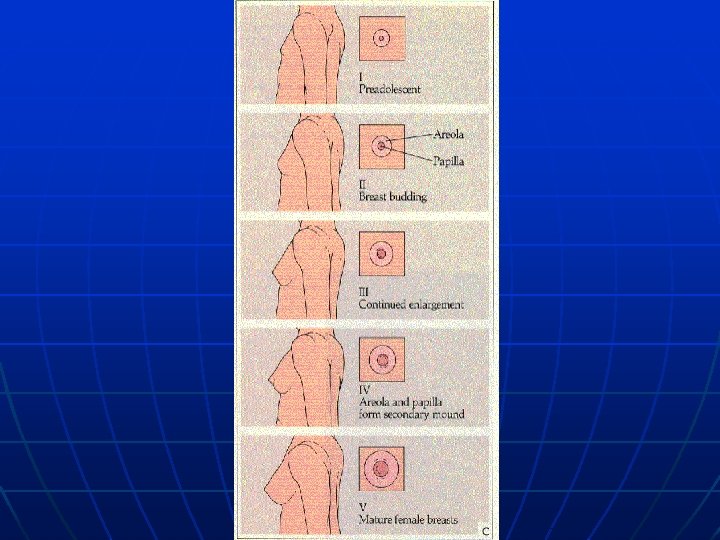
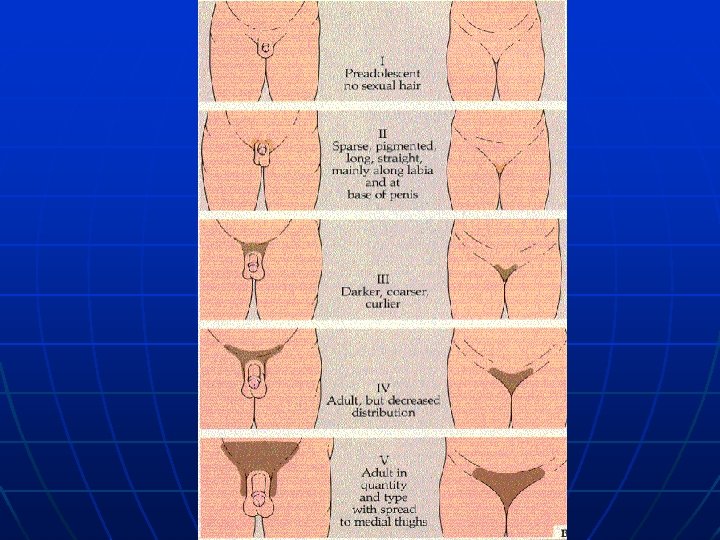
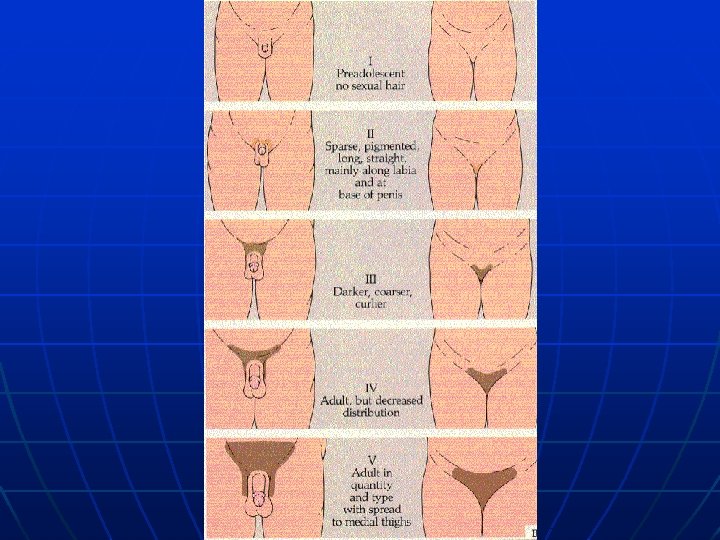
STAGING OF PUBERTY n n n NEED TO BE COMFORTABLE WITH THE STAGES OF PUBERTY NEED TO KNOW HOW TO DESCRIBE NEED TO KNOW WHAT THEY MEAN
Estrogen effects n n Breast development Change in body shape and adipose distribution Growth increase • FUSION OF GROWTH PLATES n n Menarche Psychological changes?
Androgen Effects n n Pubic and axillary hair Growth spurt (? ) Acne Body odor
NORMAL VARIANTS OF PUBERTY (early signs) n n PREMATURE THELARCHE-ONLY SEEN IN GIRLS PREMATURE ADRENARCHE-MUCH MORE COMMON IN GIRLS
PREMATURE THELARCHE n BREASTS BEGINNING BEFORE AGE OF 3 (OFTEN NOTED “SINCE BIRTH”) n NO OTHER SIGN OF PUBERTY n n NOT ASSOCIATED WITH PATHOLOGY AND DOES NOT REQUIRE FURTHER EVALUATION IN REALITY CAN’T MAKE THE DIAGNOSIS UNTIL YEARS PASS AND PUBERTY HAS NOT PROGRESSED
PREMATURE ADRENARCHE n n PUBIC HAIR AFTER THE AGE OF 3 AND BEFORE 8 No BREAST DEVELOPMENT NO OTHER SIGNS OF PUBERTY All labs pre-pubertal except adrenal androgen levels, which are appropriate for physical findings
Precocious Puberty Much more common in girls. n More likely to be idiopathic in girls. n Cannot predict the time course of pubertal development at the onset. n
PRECOCIOUS PUBERTY n n FIRST STEP IN EVALUATION IS TO DECIDE WHETHER THIS INVOLVES THE HYPO-THALAMICPITUITARY AXIS =CENTRAL PRECOCIOUS PUBERTY VERSUS-SIGNS OF PUBERTY, WITHOUT ACTIVATION OF THE HP AXIS=INCOMPLETE OR PERIPHERAL PUBERTY
Precocious puberty n n n If gonadotropins are pubertal then the problem is central. May be associated with a wide variety of CNS lesions, but most often idiopathic (in girls). Regardless of the cause, if gonadotropins are elevated it can be treated with a long acting Gn. RH analogue.
n n n EARLY SIGNS OF PUBERTY COMMON IN GIRLS. THERE ARE DATA THAT PUBERTY IN GIRLS IS OCCURRING EARLIER NOW. MAY BE ASSOCIATED WITH OBESITY. THIS IS ONLY TRUE FOR GIRLS! NO COMPARABLE DATA FOR BOYS. MENARCH HAS NOT ADVANCED.
n Puberty case 1 • A 6 YEAR OLD AFRICAN AMERICAN GIRL COMES TO YOUR CLINIC FOR A SCHOOL PHYSICAL. YOU NOTICE THAT SHE HAS TANNER II PUBIC HAIR AND A LITTLE BIT OF UNDERARM ODOR.
WHICH OF THE FOLLOWING WOULD YOU FIND REASSURING? n n A. AN ADVANCED BONE AGE. B. CLITOROMEGALLY. C. FACIAL HAIR. D. NORMAL GROWTH RATE.
n A. AN ADVANCED BONE AGE. n B. CLITOROMEGALLY. n C. FACIAL HAIR. n D. NORMAL GROWTH RATE.
PUBERTY CASE 2 n n ANGELA IS A 3 YEAR OLD WHO PRESENTS WITH A 6 MONTH HISTORY OF INCREASING BREAST DEVELOPMENT. ON EXAM SHE HAS TANNER BREASTS, AND NO PUBIC HAIR (TANNER I)
Angela is a 3 YO who presents with complaint of increasing breast development Noted over past 6 months. No other complaints. This is her growth curve.
What is Angela’s diagnosis? A. Precocious Adrenarche. n B. Premature Thelarche. n C. Exogenous androgen exposure. n D. Precocious puberty. n
PRECOCIOUS PUBERTY FIRST QUESTION-DOES SHE HAVE “CENTRAL PRECOCIOUS PUBERTY? n PELVIC ULTRASOUND WILL ALLOW YOU TO CHECK SIZE OF HER OVARIES AND SHAPE OF HER UTERUS. n THIS IS “BIOASSAY” FOR GONADOTROPINS. n
ANGELA n On pelvic ultrasound her ovaries are noted to be symetrically enlarged and her uterus is also slightly larger than pre-pubertal. n Now what?
CENTRAL PRECOCIOUS PUBERTY n DIAGNOSIS OF CENTRAL PRECOCIOUS PUBERTY REQUIRES EXAMINATION OF CNS TO BE SURE THAT THERE IS NO CENTRAL PROCESS INVOLVED (TUMOR, CYST, HYDROCEPHALUS, ETC) n USUALLY MRI IS PERFORMED.
Gn. RH analogues n n n They are long-acting agonists for the Gn. RH receptor They act by desensitizing the receptor to endogenous Gn. RH Major indications for Rx of central precocious puberty are: • Concerns about eventual short stature • Concerns re the social effects of puberty and menstruation on a young girl and her family
PUBERTY IN BOYS
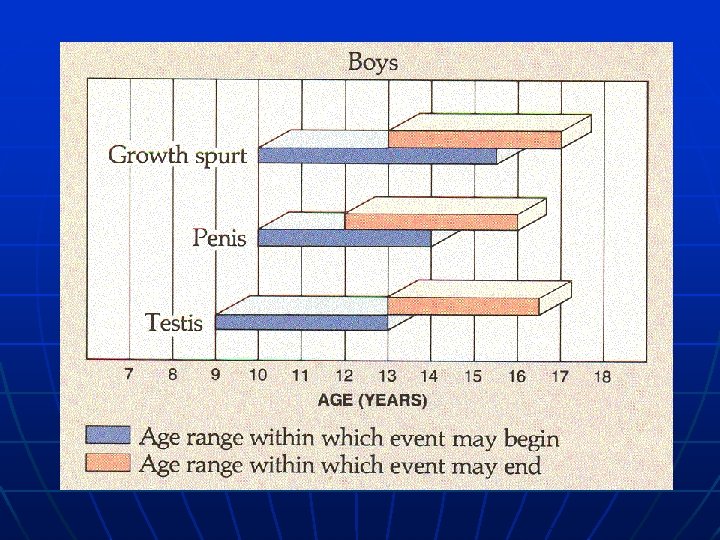
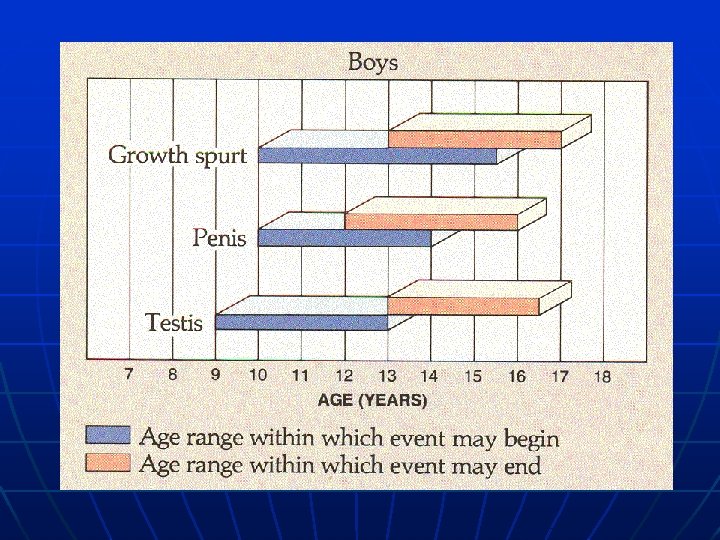
Normal puberty in boys n n n Most boys begin puberty between the ages of 9 and 15. The mean age is 12. The first sign of puberty is testicular enlargement. This is followed by pubic hair, growth of scrotum and penis, axillary hair, acne, voice changes and finally the growth spurt.
Precocious puberty in boys n n n Much less common than in girls. Much more likely to be do to a treatable disease state. Start with the same processdifferentiating puberty involving LH/FSH secretion by the pituitary vs puberty independent of gonadotropin secretion
Precocious puberty in boys (cont) n n n Unlike the situation in girls-LH alone (without FSH) can cause pubertal changes. h. CG reacts with the LH receptor and can stimulate androgen secretion and pubertal signs. Therefore in boys a h. CG secreting tumor can present as precocious puberty.
Androgen Effect n n n n Pubic and axillary hair Acne Body odor Face hair Voice changes Maturation of body shape Growth spurt
Precocious puberty in boys n n n In girls need to use U/S to see size and consistency of gonad In boys gonads are directly palpated and measure Testes measurements of greater than 2 cm in length or 4 cc in volume are pubertal.
Kevin-3 yo boy n n n Presents with increasing aggressiveness noted at preschool. His height has progressed from the 25 % at age 18 months, to 95% at 36 months. On PE has T 3 pubic hair, early changes of puberty noted in penis and scrotum.
What is the most important question about his physical exam? n n A. Is he skin coarse. B. Does he have acne. C. What size are his testicles. D. Does he need deodorant.
Precocious puberty in boys n n Since androgen effects are the physical signs of puberty in boysandrogen made by either gonad or by adrenal may be associated with early puberty If androgen is coming from adrenal this may be due to either CAH (common) or to a tumor (uncommon, but important to diagnose).
n n Even though Kevin’s genitalia look “mature” to casual glancehis testes are only 3 cc in volume. What does that mean?
Peripheral or incomplete precocious puberty n Differential diagnosis • Adrenal tumor (malignant or benign) • Exogenous androgen • Testicular tumor (rare-asymetric testes) • CAH-most common
Congenital Adrenal Hyperplasia n n If not salt-losing can present as just signs of androgen excess in either boys or girls. Need to measure precursors of cortisol either early in the morning or after a dose of ACTH to diagnose.
n DELAYED PUBERTY • No pubertal development by age 14 in girls. • No pubertal development by age 15 in boys. • Abnormal progression of puberty.
DIFFERENTIAL DIAGNOSIS OF DELAYED PUBERTY n n CONSTITUTIONAL DELAY HYPOGONADISM • HYPERGONADOTROPIC • HYPOGONADOTROPIC To understand this, go back to our cartoon of the hypothalamic-pituitarygonadal axis.
The Hypothalamic-pituitary-gonadal axis Gn. RH Gonadal steroids LH, FSH
Constitutional Delay-most common reason for delay n n Stature is less than predicted by parental heights (may be “short”) Growth rate is normal Bone age is delayed. Family history of late puberty
Mike is a 15 yo who comes in because he is “too short”. n n n On review of history he has been at 5 % for height since age 3, but has fallen slightly below this percentile in the last year. He is otherwise well. On PE he appears younger than his stated age. He is Tanner I for pubic hair and has 3 cc testes.
Does Mike have constitutional delay? n n A. Only if his bone age is delayed at least two years. B. Only if his serum gonadotropin levels are pubertal. C. No, because he has fallen further from the growth curve over the last year. D. Not enough data to be sure.
Treatment of constitutional delay n n May use testosterone injections 100 mg q month for 3 or 4 months if older than 13 or 14. GH has NOT been shown to increase final adult height in this situation.
Pathologic causes of delayed puberty n n Kallman’s syndrome-may be associated with decreased or absent sense of smell. Prolactinoma. Other CNS tumors. If not hypo-gonadotropic-defect in gonad.
Girls with delayed puberty n n n More likely to be significant. Less commonly referred. Also divide into hyper vs hypogonadotropic. Hypergonadotropic-ovarian failuremost commonly Turners syndrome-always short. Hypogonadotropic-most commonly poor nutrition/anorexia nervosa/athletic extremes.
GROWTH AND SHORT STATURE
GROWTH-NORMAL AND ABNORMAL n BABIES GROW 20 INCHES IN UTERO n 10 INCHES IN FIRST YEAR n 5 INCHES IN SECOND YEAR n 2 ½-3 INCHES / YEAR FROM AGE 3 UNTIL PUBERTY
ABNORMAL GROWTH n n DIFFERENTIAL DIAGNOSIS DEPENDS ON AGE ON ONSET GROWTH RATE MORE IMPORTANT THAN HEIGHT AT ANY GIVEN TIME ABNORMAL GROWTH RATE ALWAYS DESERVES ATTENTION SHORT STATURE (SHORTER THAN FAMILIAL PREFERENCE)-NOT ALWAYS PATHOLOGIC.
SHORT STATURE STARTING IN UTERO n n n CHROMOSOMAL ABNORMALITIES CONGENITAL INFECTION SYNDROMES ENVIRONMENTAL EXPOSURES MULTIPLE GESTATION MATERNAL FACTORS • • • HYPERTENSION IDDM WITH COMPLICATIONS NUTRITION-ESPECIALLY IF TEENAGE MOTHER
CHILDREN WITH SHORT STATURE BEGINNING IN UTERO n n MAY OR MY NOT CATCH UP ALWAYS DESERVE CAREFUL EVALUATION IF STILL SMALL AT AGE 3 MAY TRY GH TREATMENT NOTE: HORMONAL CAUSES OF SHORT STATURE DO NOT START IN UTERO
Short stature presenting in first two years of life n n Nutritional deficiencies. Normal growth pattern • Genetic short stature-finding own growth channel. • Constitutional delay-finding channel to follow until puberty-which will be later than normal. • Hormonal deficiency
GROWTH IN CHILDREN WITH GENETIC SHORT STATURE n n CHILDREN WITH GENETIC SHORT STATURE MAY BE BORN AT A NORMAL SIZE, BUT WILL DECELERATE GROWTH OVER THE FIRST 2 YEARS UNTIL ON FINAL CHANNEL OF GROWTH. THIS IS PERIOD OF TIME WHEN CHILDREN “FIND THEIR GROWTH CHANNEL”
Alex is a 14 year old boy who has been at the 5% his whole life, but now is below the 3 percentile and extremely unhappy about this.
What are the important questions regarding Alex and his future growth? n n A. Parental heights. B. His bone age. C. His pubertal stage. D. The history of pubertal development of his family members.
What are the important questions regarding Alex and his future growth? n n A. Parental heights-mean parental height at 50 th percentile. B. His bone age is markedly delayed. C. His pubertal stage – 3 cc testes and T 1 pubic hair. D. The history of pubertal development of his family membershis father did not shave until he was a senior in college.
What are the important questions regarding Alex and his future growth? n n A. Parental heights-mean parental height at the 5 th percentile. B. His bone age-is 12 at his CA of 14 8/12. C. His pubertal stage-he has 6 cc tests and Tanner II pubic hair. D. The history of pubertal development of his family members. His father had normal puberty as far as he remembers.
ALEX’S DX n CONSTITUTIONAL DELAY
Ben is another 14 year old boy who has been at the 5% his whole life, but now is extremely unhappy about this.
WHAT WILL HELP YOU DETERMINE BEN’S DX
NEED TO KNOW n n PARENTAL HEIGHTS. PUBERTAL STAGE BONE AGE. HISTORY OF PARENT’S PUBERTY
BEN’S DATA n n BEN’S FATHER IS 5’ 4” HIS MOTHER IS 4’ 10” HIS BONE AGE IS 14 6/12 HE IS TANNER IV FOR PUBIC HAIR
BEN’S DIAGNOSIS GENETIC SHORT STATURE
GROWTH HORMONE DEFICIENCY n THIS IS THE DIAGNOSIS THAT EVERY FAMILY WITH A SHORT CHILD IS CONCERNED ABOUT.
Ghrelin GHRH Somatostatin GH plus IGF 1 GROWTH
SHORT STATURE n n NOT A DISEASE MAY BE DUE TO NORMAL VARIANT PATHOLOGY IS DETERMINED BY GROWTH RATE-NOT STATURE LOW GROWTH RATE INDICATION FOR EVALUATION
GROWTH HORMONE DEFICIENCY IS RARE CAUSE OF POOR GROWTH n OTHER CAUSES INCLUDE • POOR NUTRITION • RENAL DISEASE (RTA, RENAL INSUFFICIENCY) • INFLAMMATORY BOWEL DISEASE • PSYCHO-SOCIAL ISSUES • MEDICATIONS STEROID n AMPHETAMINE n ? OTHER n
ENDOCRINE CAUSES OF SHORT STATURE n n MOST COMMON ENDOCRINE CAUSE OF POOR GROWTH IS HYPOTHYROIDISM CUSHING SYNDROME-USUALLY EXOGENOUS GROWTH HORMONE DEFICIENCY VERY POORLY CONTROLLED DIABETES
GROWTH HORMONE DEFICIENCY n CLUES TO THE DIAGNOSIS-IF CONGENITAL • MAY HAVE MICRO-PENIS OR MICROCLITORIS • MAY HAVE HAD NEONATAL HYPOGLYCEMIA • MAY HAVE OTHER MID-LINE DEFECTS • MAY HAVE HAD PROLONGED JAUNDICE
CONGENITAL GH DEFICIENCY n n BABIES BORN NORMAL SIZE MAY HAVE OTHER NEONATAL PROBLEMS GROWTH MAY BE SOMEWHAT POOR FIRST 18 MONTHS, BUT THEN FALLS FROM CURVE WITH LOW GROWTH RATE MAY CONTINUE TO HAVE UNDIAGNOSED HYPOGLYCEMIA
CONGENITAL GH DEFICIENCY n n n MUST RULE OUT OTHER PITUITARY HORMONE DEFICIENCIES. HYPOGLYCEMIA WILL RESPOND TO GH TREATMENT. UNDIAGNOSED ACTH DEFICIENCY MAY BE FATAL.
ACQUIRED GH DEFICIENCY n n n HALLMARK IS DECREASED GROWTH RATE. LOW SOMATOMEDIN C (IGF-1) MAY BE CLUE DELAYED BONE AGE USUALLY SEEN NEEDS TO BE EVALUATED BY PEDIATRIC ENDOCRINOLOGIST ALWAYS NEED TO RULE OUT CNS TUMOR.
THYROID DISEASE IN CHILDREN AND ADOLESCENTS
CONGENITAL HYPOTHYROIDISM NOT RARE-IRREVERSIBLE DAMAGE IS NOT TREATED PROMPTLY AND ADEQUATELY
NEWBORN SCREENING n n n INCUMBENT ON YOU TO SEE THAT SAMPLE SENT, RESULTS NOTED AND PATIENT CONTACTED AND TREATED. CAN NOT ASSUME ANYTHING. NEGATIVE SCREEN DOES NOT RULE OUT DIAGNOSIS.
Thyroid Physiology TRF THYROXINE TSH THYROID
THRYOID DISEASE n TIME COURSE OF TSH IN FIRST WEEK OF LIFE
Newborn TSH Surge
Congenital Hypothyroidism n n Incidence is about 1/3, 500 Etiology: • 10% biochemical defect in thyroid synthesis • 60% ectopic thyroid gland • 30% athyrotic
Congenital Hypothyroidism n Signs: • Puffiness around eyes • Large tongue • Hoarse cry • Mottled skin, Failure to maintain temperature • Umbilical hernia • Large fontanel-posterior fontanel open
n n WHILE YOU HAVE TO KNOW THE “SIGNS AND SYMPTOMS” OF CONGENITAL HYPOTHYROIDISMNOTE-LESS THAN 5% OF INFANTS WITH CONFIRMED HYPOTHYROIDISM DETERMINED BY NEWBORN SCREEN WERE DIAGNOSED CLINICALLY PRIOR TO SCREEN RESULTS!
You are called because of a positive newborn screen for hypothyroidism on a 2 week old baby girl, Janelle. n n T 4 is 5. 9 (normal 8 -14) TSH is 196 (normal 3. 8 -6. 9)
Your best next move is: n n A. Schedule her for routine visit at 2 months. B. See her immediately, and start her on T 4 pending repeat labs. C. Schedule her to come in for labs and tell the mother that you will call with the results. D. See her in clinic and if she seems normal reassure the parents that she is probably fine.
n n A. Schedule her for routine visit at 2 months. B. See her immediately, and start her on T 4 pending repeat labs. C. Schedule her to come in for labs and tell the mother that you will call with the results. D. See her in clinic and if she seems normal reassure the parents that she is probably fine.
TREATMENT OF CONGENITAL HYPOTHYROIDISM n GOALS OF THERAPY-TO NORMALIZE T 4 AND TSH AS RAPIDLY AS POSSIBLE. • PREFERABLY BY 4 WEEKS OF AGE. • STARTING DOSE OF T 4 USUALLY 12 -15 MICROGRAM PER KG • FOLLOW free T 4 and TSH LEVELS MONTHLY ONCE NORMALIZED. • SOY FORMULA MAY BE PROBLEM
ACQUIRED HYPOTHYROIDISM n n MAY PRESENT WITH GROWTH FAILURE, CONSTIPATION, ABDOMINAL PAIN OR FTT WITH/OR WITHOUT GOITER MAY PRESENT AT ANY AGE. MORE COMMON IN GIRLS USUALLY AUTOIMMUNE
A. B. C. D. This 9 -year-old boy presented to the endocrine clinic because he had not grown since age 5 years. Notice his sallow complexion and periorbital edema. Which of the following is true? Appropriate workup should include a T 4 and a TSH. Appropriate workup should include serum cortisol, LH, and FSH. He may lose intellectual functioning, even if he is treated adequately. He will always be short, even if treated adequately.
HYPERTHYROIDISM n n MOST COMMON IN GIRLS MOST COMMON IN ADOLESCENTS CAN PRESENT AS BEHAVIORAL PROBLEMS/HYPERACTIVITY (BEWARE OF LATE ONSET HYPERACTIVITY) CAN PRESENT AS CARDIOVASCULAR SIGNS AND SYMPTOMS (HBP, DIZZINESS OR PALPATATIONS)
HYPERTHYROIDISM n TREATMENT OPTIONS INCLUDE • • • MEDICATIONS (PTU OR METHIMAZOLE) SURGERY I 131 PATIENTS WITH GRAVES DISEASE NEED LONG TERM FOLLOW UP NO MATTER HOW TREATED, AS MAY RECUR OR PATIENT MAY DEVELOP HYPOTHYROIDISM.
CALCIUM HOMEOSTASIS
CALCIUM HOMEOSTASIS n CIRCULATING CALCIUM EXISTS IN 3 FORMS • IONIZED-ABOUT 45%-THIS IS THE FORM THAT IS REGULATED BY THE BODY • PROTEIN-BOUND (40%) • COMPLEXED TO OTHER IONS (NOTABLY PHOSPHATE)
CALCIUM HOMEOSTASIS n SHORT TERM CONTROLLED BY PTH • PTH SECRETED MOMENT BY MOMENT IN RESPONSE TO CIRCULATING CONCENTRATION OF IONIZED CALCIUM n LONG TERM CONTROLLED BY CONCENTRATION OF 1, 25 DIHYDROXY VITAMIN D.
VITAMIN D n n MOST COMMON DISEASE OF CALCIUM HOMEOSTASIS IS VITAMIN D DEFICIENT RICKETS TOTALLY PREVENTABLE OCCURS ONLY IN GROWING BONES ALL INFANTS TAKING LESS THAN 500 ML OF FORMULA NEED VITAMIN D SUPPLEMENTATION (200 -400 IU/DAY.
VITAMIN D DEFICIENT RICKETS PRESENTATION: GROWTH FAILURE DELAYED MOTOR MILESTONES LOW SERUM CALCIUM LEVELS, WITH OR WITHOUT SEIZURES BONY ABNORMALITIES (for example-BOWED LEGS)
VITAMIN D DEFICIENT RICKETS n LAB FINDINGS • LOW OR LOW NORMAL LEVELS OF 25 HYDROXYVITAMIN D • NORMAL OR LOW SERUM CALCIUM • USUALLY NORMAL 1, 25 DIHYDROXY VITAMIN D • ELEVATED PTH • ELEVATED ALKALINE PHOSPHATASE • LOW OR LOW NORMAL SERUM PHOSPHATE
JAMIE IS A 13 MONTH OLD BOY WHO PRESENTS WITH DELAYED IN WALKING n n n HE IS EXCLUSIVELY BREAST FED WITH SOLID FOOD INTRODUCED AT AGE 6 MONTHS. NO SUPPLEMENTS. HIS EARLY MILESTONES WERE NORMAL HE IS AFTRICAN-AMERICAN
WHAT TESTS WOULD YOU ORDER? n A. 1, 25 DIHYDROXY VITAMIN D. n B. 25 HYDROXYVITAMIN D. n C. SWEAT TEST. n ROUTINE CHEMISTRIES.
OTHER DISEASES OF CALCIUM HOMEOSTASIS n HYPOPARATHYROIDISM • RARE-USUALLY AS PART OF MULTIPLE ENDOCRINE DEFICITS • LABORATORY VALUES INCLUDE LOW CALCIUM AND ELEVATED PHOSPHATE LEVELS • TREATED WITH 1, 25 DIHYDROXY VITAMIN D AND CALCIUM
CONDITIONS WITH ELEVATED SERUM CALCIUM n n HYPERPARATHYROIDISM HYPERCALCEMIA ASSOCIATED WITH MALIGNANCY OR GRANULOMATOUS DISEASE FAMILIAL HYPERCALCEMIC HYPOCALCIURIA VITAMIN D TOXICITY
DIABETES MANAGEMENT
DIABETES IN CHILDREN AND ADOLESCENTS n n n NOT JUST TYPE I ANY MORE TREATMENT OF TYPE II OFTEN STARTS WITH INSULIN NO CLEAR CONSENSUS RE TREATMENT OF TYPE II STAY TUNED-BUT SHOULD CONSIDER THIS. WE ARE ALSO SEEING “COMBINATION” PATIENTS WITH I+II
Goals of Therapy n n n Avoid life-threatening, acute metabolic imbalance including: • Diabetic ketoacidosis • Severe hypoglycemia Prevent hospitalization Minimize symptoms related to hyperglycemia and hypoglycemia Achieve normal linear growth and sexual development n Maintain normal body weight n Allow normal school activities, job performance, or social/recreational activities
NEW GOALS OF THERAPY n AVOID LONG TERM COMPLICATIONS OF DISEASE • NEPHROPATHY • RETINOPATHY • NEUROPATHY • VASCULAR DISEASE
TO AVOID COMPLICATIONS n n NEED TO KEEP BLOOD GLUCOSE CONCENTRATION AS CLOSE TO NORMAL AS IS POSSIBLE WITHIN THE CONSTAINTS OF THE CHILD’S DEVELOPMENT, ENVIRONMENT AND PHYSIOLOGY. HOW?
Patient Educational Curriculum Intensive Diabetes Management n n Insulin action/ insulin regimens Rationale for self-monitoring of BG: testing frequency, goals, patterns Glycated hemoglobin: testing frequency, goals Nutrition management • Healthy food choices • Role of major nutrients: Effects on BG • Sick day management • Label reading • Dining out/convenience foods
Educational Curriculum (cont. ) n n Effect of exercise Interaction of exercise, diet, and medication Hypoglycemia: causes, treatment, prevention Glucagon
Mimicking the Pancreas Delivery of Insulin
Basal/Bolus therapy Pancreas Delivery Meal Boluses Basal Rate
Insulin Preparations Class Agents Human insulins Regular, NPH, lente, ultralente Insulin analogues Aspart, glulisine, lispro, glargine Premixed insulins Human 70/30, 50/50 Humalog mix 75/25 Novo. Log mix 70/30
Profiles of Human Insulins Plasma insulin levels Regular 6– 8 hours NPH 12– 20 hours Ultralente 18– 24 hours 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 Hours
Action Profiles of Insulin Analogues Plas ma insuli n levels Aspart, glulisine, lispro 4– 6 hours Regular 6– 8 hours NPH 12– 20 hours Ultralente 18– 24 hours Glargine 24 hours 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 Hours
Split-Mixed Regimen U/m. L NPH Regular 100 B Human Insulins NPH Regular L D 80 Normal pattern 60 40 20 0600 0800 1200 B=breakfast; L=lunch; D=dinner 1800 Time of day 2400 0600
Basal-Bolus Insulin Treatment With Insulin Analogues U/m. L 100 Lispro, glulisine, or aspart B L D 80 Glargine 60 40 Normal pattern 20 0600 0800 1200 B=breakfast; L=lunch; D=dinner 1800 Time of day 2400 0600
Symptoms of Hypoglycemia n n n n Headache Sweating Shakiness/tremors Irritability Weakness Confusion Personality changes Rapid heart rate
“Rule of 15” n n Treat a low blood sugar with 15 grams of fast-acting carbohydrate Wait 15 minutes and recheck BS If BS is not above 70 mg/dl, then retreat with 15 grams, and recheck in 15 minutes Once BS is corrected, give a small snack, or the regularly scheduled meal within 30 minutes.
Fast-Acting Carbs n n n n Orange/apple juice Regular soft drink Glucose tablets Glucose gel Honey or corn syrup Sugar packets Life Savers/hard candy n n n n 4 oz = ½ cup 3 tablets 1 tube 1 tablespoon 3 packets 3 -8 pieces
Preventing Hypoglycemia n Check BG 4 -6 times per day n Carry glucose tablets n Have glucagon kit available
Symptoms of Hyperglycemia n n n Polyuria Polydipsia Headache Fatigue Blurred vision
“Sick Day Management” n n n SICK DAY RULES Remember to check the urine for ketones if: • Blood sugar is > 240 mg/dl • You are sick • You are vomiting You must always take some insulin, even if you are unable to eat. If you feel a lower insulin dose might be needed for a few days because you/your child may be unable to eat the usual amount of food, contact the diabetes team to discuss a new dose.
SICK DAY MANAGEMENT (CONT) n n If you are unable to eat, you can sip regular Coke, Sprite or juice to provide equivalent amounts of carbohydrate to meet your meal plan. Keep a close check on blood sugar and ketone levels. • Check blood sugar levels every 2 -4 hours during illness. • Check urine ketone levels every 4 hours during illness.
Exercise and Diabetes Mellitus n n n n Increased insulin sensitivity Increased glycogen stores Increased amino acid uptake Decreased Hb. A 1 c Decreased circulating lipids Lower resting B/P Increased cardiac dynamics
Medical Nutrition Therapy n n n Provide adequate energy for growth and development Attain optimal metabolic control Healthy food choices Reduce lipid-related macrovascular disease Prevent nephropathy
Somogyi Effect n n High glucose and sometimes ketones upon awakening Caused by a low glucose level during the night A result of over-insulinization Treatment is to lower nocturnal insulin doses
Dawn Phenomenon n n A tendency to wake up with high glucoses Normal insulin secretion is lowest at about 2 -3 a. m. and then increases at dawn
Dawn Phenomenon n Thought to be the result of early morning secretion of GH and cortisol When NPH is given at supper, it peaks at 2 -3 a. m. and dwindles at dawn, and may cause early morning hyperglycemia Treatment is to move the NPH injection to bedtime
SEX DIFFERENTIATION AND INTERSEX CONDITIONS
Factors Leading to Abnormal Sexual Differentiation n Chromosomal abnormalities • Too many: 47, XXY • Too few: 45, X/46, XY n Deficiencies in testicular hormones in males • Testosterone deficiency • MIF deficiency n End organ unresponsiveness to testosterone • Androgen receptor deficiency • 5 -α-reductase deficiency n Excessive androgen in females • Congenital adrenal hyperplasia • Placental transfer of androgens n Congenital malformations • Exstrophy of the bladder • LUB syndrome
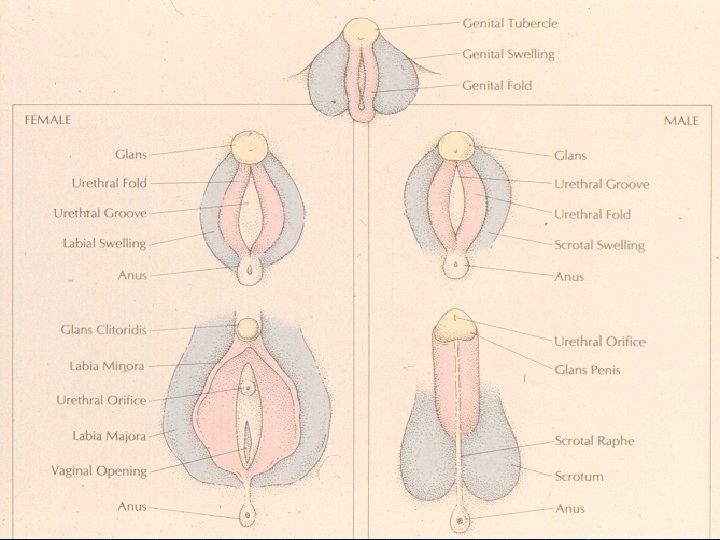
Sexual Differentiation n Genetic sex • Karyotype n Gonadal sex • Determined by genetic sex n Phenotypic sex • Appearance of external genitalia n Psychological sex • Gender identity/sex of rearing
Presence of Y chromosome generally determines testicular differentiation XY XXY Testis XYY X XX XXX • Exceptions: XY females; XX males Ovary
Sexual Differentiation Y Chromosome Testis Determining Gene TESTOSTERONE Testis MIF (passive) Ovary Wolffian Ducts Vas Deferens Seminal Vesicles Epididymis Mullerian Ducts Wolffian Ducts Mullerian Ducts Fallopian Tubes Uterus Upper ⅓ of Vagina
MALE DIFFERENTIATION Testosterone (5 -αreductase) Di-Hydro-Testosterone Androgen Receptor (X q 11 -12) Virilization of External Genitalia Note: this is effect of systemic androgen Wolffian Ducts Note: this is local effect of testosterone
Androgen Excess n n n An excessive amount of androgen in the female can virilize the internal and external genitalia Excess androgen can be exogenous Most likely cause of endogenous androgen in congenital adrenal hyperplasia (more about that later)
Gender-male development Chromosomes Genes. SRY, and others Gonad Hormones steroids peptides
IN NEWBORN NURSERY YOU ARE EXAMINING YOUR NEW PATIENTS AND NOTICE THIS.
Micropenis
QUESTIONS n n n WHAT COULD CAUSE THIS? IS THIS AN OVER VIRILIZED FEMALE OR AND UNDER VIRILIZED MALE? GENDER ASSIGNMENT ISSUES WHAT DO YOU WANT TO KNOW ON PHYSICAL? WHAT LABS DO YOU WANT?
MICROPENIS (CONT) n n ARE THERE PALPABLE TESTES IN THE SCROTUM? IS THE BABY HYPERPIGMENTED? ARE THERE ANY OTHER SIGNS OF MIDLINE DEFECTS? HYPOGLYCEMIA? ULTRASOUND OF PELVIS OFTEN USEFUL
MICROPENIS (CONT) n n n GENDER ASSIGNMENT SHOULD BE MADE EXPEDITIOUSLY, BUT NOT FRIVOLOUSLY. FAMILY HX OFTEN VERY USEFUL. LABS-CHROMOSOMES, SEX STEROID LEVELS, GLUCOSE, ADRENAL STEROID LEVELS?
MICROPENIS n n THIS BABY HAD NORMAL TESTES PALPABLE IN THE SCROTUM NO MIDLINE FEMALE STRUCTURES WERE FOUND ON ULTRASOUND HIS MATERNAL UNCLE ALSO HAD MICROPENIS, AS DOES HIS COUSIN DX : PARTIAL ANDROGEN INSENSITIVITY.
NEXT CASE n n n You are called to nursery to see baby delivered 1 hour ago. Baby term, uncomplicated P, L and D. Birth Wt 7# 8 oz. APGARs 8 and 9. Abnormal genitalia noted in delivery room.
SAME QUESTIONS n n NO PALPABLE TESTES KARYOTYPE 46 XX 17 HYDROXYPROGESTERONE 25 X UPPER LIMIT OF NORMAL NO FAMILY HISTORY OF SIMILAR PROBLEMS, BUT BROTHER DIES AT 2 WEEKS OF AGE WITH “SEPSIS”.
Cholesterol Adrenal Pathway Pregnenolone 17 -OH Pregnenolone Progesterone 17 -OH Progesterone Deoxycorticosterone 11 -Deoxycortisol (Compound “S”) Corticosterone 18 -OH-Corticosterone Aldosterone Cortisol (Compound “F”) DHEA Androstenedione Testosterone
21 -Hydroxylase Deficiency: Treatment n Replace cortisol with hydrocortisone • Often need at least 15 mg/M 2/day to control ACTH secretion. n Replace mineralocorticoid with fludrocortisone (Florinef). n Follow growth velocity, blood pressure. n Follow labs: 17 -OH progesterone, androstenedione, plasma renin, bone age.
Adrenal Physiology CRF ACTH CORTISOL ADRENAL GLAND
Normal Cortisone Production n Production rate: 8 -12 mg/M 2/day ACTH peaks at 4 -8 a. m. , and is low in the afternoon During times of physiologic stress, the production increases 3 -5 fold
Disorders of the Adrenal insufficiency: Addison’s disease Cushing syndrome (or disease) Congenital adrenal hyperplasia
Overproduction n Cushing’s Syndrome • Clinical features of excess cortisol n Cushing’s Disease • Refers to ACTH-producing adenoma • Loss of diurnal variation in ACTH/cortisol secretion is key to diagnosis
Cushing’s Syndrome n n n n Central obesity “Moon Face” “Buffalo Hump” Muscle weakness Growth failure May have androgen excess Most often iatrogenic
These girls are monozygotic twins celebrating their 11 th birthdays. The shorter of the two girls has not grown well for the past two years. Appropriate workup should include: A. B. C. D. FSH, LH Cortisol determinations Pelvic ultrasound Serum GH determination after provocative stimuli
A. FSH, LH B. Cortisol determinations C. Pelvic ultrasound D. Serum GH determination after provocative stimuli
NEXT CASE n n JANICE IS A 10 YEAR OLD GIRL REFERRED TO ME FOR POSSIBLE CUSHINGS SYNDROME. SHE HAS ALWAYS BEEN “A LARGE GIRL” BUT OVER PAST 6 MONTHS SHE HAS GAINED 16 POUNDS AND HAS A NUMBER OF STRIAE ON HER ABDOMIN AND UPPER THIGHS
CUSHING SYNDROME (CONT) n ON REVIEW OF HER HISTORYJANICE GREW AT THE 90 -95% FROM AGE 6 -9 AND SINCE THEN HAS INCREASED HER GROWTH RATE SO THAT NOW SHE IS WELL ABOVE THE 99% FOR HEIGHT AND HER WEIGHT IS EVEN FARTHER FROM THE CURVE.
CUSHINGS SYNDROME? n n DOES SHE HAVE CUSHINGS SYNDROME AND HOW DO YOU KNOW? CUSHINGS SYNDROME ASSOCIATED WITH DECREASED GROWTH RATEJANICE’S GROWTH HAS ACCELERATED WITH HER WEIGHT GAIN. SHE DOES NOT HAVE CUSHINGS.
Cortisol Deficiency: Addison’s Disease n n In 1855, Thomas Addison first described adrenal insufficiency His cases were caused by tuberculosis of the adrenal Most cases today are autoimmune Increased incidence in type 1 diabetes
Addison’s Disease: Symptoms n n Fatigue Weight loss Hypoglycemia MAY BE SUBTLE
Addison’s Disease: Signs n n n Hypotension Muscle wasting Hyperpigmentation • No “tan line” • Favors scars, gums, creases in palms • May be vitiligo
Addison’s Disease: Lab n n Low Na+ High K+ Hypoglycemia High ACTH
Addison’s Disease: Treatment n Acute treatment for crisis, shock • IV Normal saline, glucose • IV Hydrocortisone 50 -100 mg, then 25 -50 mg IV q 6 -8 hrs n Maintenance therapy • Hydrocortisone 15 -25 mg/M 2/day • Florinef (0. 1 mg tabs) 0. 5 -2. 0 mg/day
Congenital Adrenal Hyperplasia n n Caused by enzyme deficiencies in the adrenal pathway-MOST COMMON CAUSE OF ADRENAL INSUFFICIENCY IN PEDIATRICS. Different enzyme deficiencies produce different clinical findings. The degree of the deficiency influences the clinical findings. Boys and girl affected differently.
Sorting Out the Adrenogenital Syndrome n Virilizing • 21 -Hydroxylase deficiency n n Salt-losing Non-salt-losing • 11 -Hydroxylase deficiency n n n Hypertensive Non-hypertensive Mixed • 3β-OH-Steroid dehydrogenase (usually salt-losing) n Non-virilizing • • • 17 Hydroxylase deficiency 20, 22 Desmolase deficiency 17, 20 Desmolase deficiency
Sorting Out the Adrenogenital Syndrome n Virilizing • 21 -Hydroxylase deficiency n n Salt-losing Non-salt-losing • 11 -Hydroxylase deficiency n n n Hypertensive Non-hypertensive Mixed • 3β-OH-Steroid dehydrogenase (usually salt-losing) n Non-virilizing • • • 17 Hydroxylase deficiency 20, 22 Desmolase deficiency 17, 20 Desmolase deficiency
21 -Hydroxylase Deficiency n Most common adrenal enzyme deficiency • Accounts for about 95% of all cases of CAH n n Presents as virilization or sexual ambiguity in girls, as in our case. Currently many states screen for this.
21 -Hydroxylase Deficiency n n Boys usually present at 10 -14 days in adrenal crisis Boys may have adrenal rest tissue in testes, which are palpable masses (10%)
21 -Hydroxylase Deficiency n Less severe enzyme deficiencies may not cause salt-losing • Has been called “Simple Virilizing CAH. ” n n May present as “precocious pseudopuberty. ” Very mild enzyme deficiency may be “cryptic” and present at puberty as excess androgen in girls.
11 -Hydroxylase Deficiency n n n Next most common adrenal enzyme deficiency • Accounts for almost 5% of all cases of CAH Presents as virilization or sexual ambiguity in girls. • Does not cause adrenal mineralocorticoid crisis--may be hypertensive at diagnosis Boys may present with precocious puberty
11 -Hydroxylase Deficiency: Treatment n Replace cortisol with hydrocortisone • Often need at least 15 mg/M 2/day to control ACTH secretion n Do not need mineralocorticoid replacement Follow growth velocity, blood pressure Follow labs: 17 -OH progesterone, androstenedione, plasma renin, BA
This female infant (karyotype 46, XX) with enlarged clitoris was also noted to be hypertensive (180/120) at the first newborn check‑up. Labs had been drawn immediately after birth, and have just returned. What would explain her combination of virilization and hypertension? A. 21 hydroxylase deficiency B. Addison’s disease. C. Cushings disease D. 11 hydroxylase deficiency.
n n ENDOCRINOLOGY IS FUN. ENDOCRINE DISEASES PRESENT THE WAY THEY SHOULD AS PREDICTED BY THEIR BIOCHEMISTRY AND PHYSIOLOGY EACH DISEASE MIGHT BE RARE, BUT IN COMBINATION THEY ARE NOT RARE. THUS IT IS IMPORTANT TO KEEP THEM IN MIND.