LTC Karen S Vogt Pediatric Endocrinology WRNMMCB March

LTC Karen S. Vogt Pediatric Endocrinology, WRNMMCB March 2013 Rickets

PREP 2013 Content Specifications �Understand the necessity of adequate vitamin D intake in children and adolescents �Understand the necessity of calcium and phosphorous intake in children and adolescents �Know that hypocalcemia with hypophosphatemia suggests vitamin D deficiency

PREP 2013 Content Specifications �Understand the mechanism of rickets in children with hepatic disease �Plan the treatment of a child with familial hypophosphatemic rickets

Outline �Case �Nutritional rickets and Vitamin D deficiecy �Prevention �Other types of rickets �PREP Questions

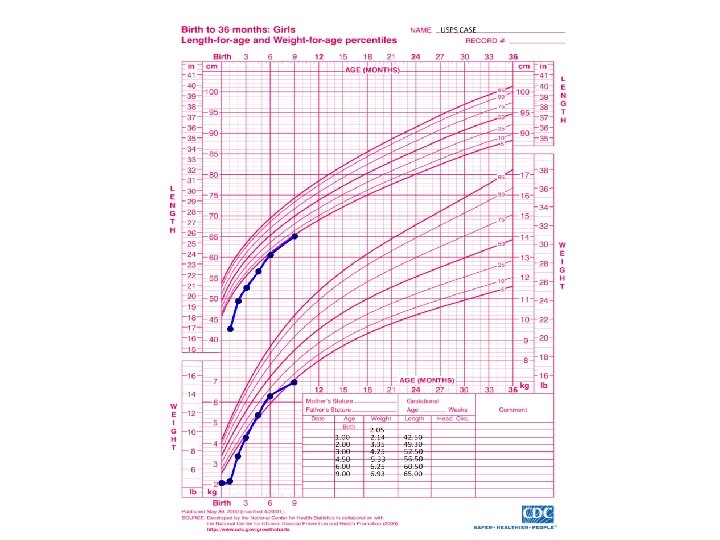
Case � 9 month old female presents in January for her well baby visit

History �Birth: C-section at 34 weeks for placental abruption Required PRBC transfusion x 2 PDA - closed after indomethacin x 1 18 day NICU stay �PMH: healthy �Immunizations: up-to-date

More History �Diet: exclusively breastfed until 6 months of age, now taking stage 2 baby foods and soft table foods �Meds: Poly-vi-sol in first 3 months of life, no current meds �Development: sits unsupported when placed, pulls to stand, cannot get from lying to sitting, immature pincer grasp, waves bye-bye, plays peek-a-boo, consonant babbling

History and Physical Exam �Family History: parents healthy, mom no longer taking prenatal vitamins, mom is Filipino, dad is half caucasian/half Filipino �Physical Exam : Unremarkable

Plan…. �Weight check in one month �Mom comes back in 2 weeks for concern for difficulty feeding �Less appetite for solids than previously and no weight gain from well visit

Labs �TSH, CRP, Celiac Panel – unremarkable �Fecal fat, reducing substances and alpha-1 - antitrypsin – normal �Sweat test – normal �CMP� � Alk Phos 736 U/L Calcium 9. 2 mg/dl Albumin 4. 0 g/dl (150 -420) (8. 7 -10. 4) (3. 5 -5)

Labs �CBC � � WBC 12. 6 Hgb 10. 8 Hct 34. 7 Plt 547 MCV 64. 6 (70 -86)

Pediatric Endocrinology Consult �More History: Mom drinks no milk, occasional cheese, doesn’t like yogurt �Infant light skinned and born in early spring �Minimal time in the sun per mom – spent most of summer indoors �PE: subtle wrist widening, slight concavity of lateral chest walls, mild generalized low tone
 � Calcium: 8. 8 mg/dl")
More Labs…. � Alk Phos: 568 U/L (150 -420) � Calcium: 8. 8 mg/dl (8. 7 -10. 4) � Albumin: 4. 7 g/dl (3. 5 -5) � Corrected Ca: 8. 24 mg/dl (8. 7 -10. 4) � Phosphorus: 2. 5 mg/dl � PTH: 346. 1 pg/ml (13 -75) � 25 OH Vit D: < 4. 0 ng/ml (2. 7 -4. 5)




 2000 IU")
Diagnosis �Rickets due to vitamin D deficiency �Treatment: Ergocalciferol (Drisdol® 8000 IU/ml) 2000 IU daily Calcium carbonate 40 mg/kg/day div bid

Pediatrics Aug 2008: 122: 398 -417
 in")
Rickets - Definition �Failure in the mineralization of newly synthesized bone matrix (osteoid) in growing bone �Due to deficiencies in calcium, phosphorous, or both �Most common cause is Vitamin D deficiency

Definitions �Osteomalacia – equivalent in mature bone �Contrast to osteoporosis Low bone mass due to decreased mineralization and decreased bone matrix

Vitamin D Synthesis
 – plant source Cholecalciferol (D 3)")
Vitamin D - Sources �Dietary Ergocalciferol (D 2) – plant source Cholecalciferol (D 3) – animal source �UVB exposure Promotes conversion of 7 -dehydrocholesterol to cholecalciferol (D 3) in the skin
D by 25 - hydroxylase in")
Vitamin D Metabolism �Vitamin D is converted to 25(OH)D by 25 - hydroxylase in the liver � 25(OH)D A. k. a calcidiol Inactive form Reflects total body stores (2 -3 week ½ life)
D is converted to 1, 25(OH)2 D by 1α- hydroxylase")
Vitamin D Metabolism � 25(OH)D is converted to 1, 25(OH)2 D by 1α- hydroxylase in the kidney � 1, 25 -OH 2 D A. k. a calcitriol Active form More tightly regulated (4 -6 hour ½ life)
 �Stimulated by PTH Low phosphorous levels")
1α-hydroxylase (kidney) �Stimulated by PTH Low phosphorous levels
")
1, 25 -OH 2 Vitamin D �Acts on the vitamin D receptor (nuclear receptor) at the target organs �Major effect: absorption of calcium and phosphorous from the GI tract �Immunomodulary effects
 �Actions: keep serum calcium normal Bone – stimulates reabsorption Kidney: ▪")
Parathyroid Hormone (PTH) �Actions: keep serum calcium normal Bone – stimulates reabsorption Kidney: ▪ Stimulates 1α-hydroxylase ▪ Increases calcium reabsorption ▪ Increases phosphate excretion �Stimulated by decreased serum calcium levels �Hypomagnesemia impairs its secretion

Alkaline Phosphatase �Produced by active osteoblasts, which form unmineralized matrix �Levels increase with increased osteoblast activity

Pathophysiology �Deficient GI absorption of : Calcium → hypocalcemia → ↑PTH: ▪ Release of calcium and phosphorous from bones ▪ Activation of 1α-hydroxylase → increased formation of 1, 25 -OH 2 D ▪ Increase in renal phosphate loss Phosphorous

Pathophysiology �Net effect: decreased calcium and phosphorous available for bone mineralization �Osteoid continues to form without mineralization Expansion of the growth plate Metaphyseal irregularities, fraying, flaring �Bones become “soft” and less rigid

Increasing Prevalence of Vitamin D Deficiency Rickets �Reasons for increasing prevalence Exclusive breastfeeding Breastfeeding moms with insufficient vitamin D stores Increasing use of sunscreen Less time spent outdoors Pediatrics 2008; 122: 398 -417

Patient Risk Factors �Prematurity �Exclusive breastfeeing for 6 months (although was on poly-vi-sol for the first 3 months) �Probable vitamin D deficient breastfeeding mother �Winter season �Minimal sun exposure

Other Risk Factors – Vit D deficiency �Nutritional �Dark skin �Malabsorption �Obesity (sequestration in body fat) �Liver or kidney disease

Drugs �Anticonvulsants �Glucocorticoids �HIV medications �Rifampin �Isoniazide �Ketoconazole

Clinical Presentation - Rickets �Incidental finding �LE bowing �Delayed walking �Failure to thrive �Bone pain �Pathologic fracture �Hypocalcemia (to include seizure) �Weakness �Pneumonia, other respiratory infection �Anorexia �Restlessness/irritability

Frontal Bossing

Rachitic Rosary

Chest Deformity

Leg Bowing - genu varus

Wide Wrists

Wide Ankles

Physical Exam Findings �Poor growth or weight gain �Delayed anterior fontanelle closure �Teeth: delayed eruption, enamel defects �Generalized muscular weakness/hypotonia

Radiographic Findings �Wrist and/or knee films usually �Metaphyseal fraying, widening, flaring, cupping �Periosteum separated from the diaphysis �Generalized osteopenia

Associated Lab Findings �Iron deficiency anemia �Renal Fanconi syndrome

Vitamin D Deficiency Screening �Who? Nonspecific symptoms: poor growth, gross motor delays, unusual irritability Dark skin infants in higher latitudes in the winter and spring Children taking chronic glucocorticoids or anticonvulsants Chronic diseases associated with malabsorption Frequent fractures and low BMD Pediatrics 2008; 122: 398 -417
 If elevated: 25 OH Vitamin")
Vitamin D Deficiency Screening �How? Serum Alkaline Phosphatase (ALP) If elevated: 25 OH Vitamin D, PTH, Calcium and Phosphorus Films: ▪ Wrist ▪ Knee Pediatrics 2008; 122: 398 -417

Treatment of Vitamin D Insufficiency or Deficiency �< 1 month of age: 1000 IU/day � 1 -12 months of age: 1000 -5000 IU/ day �> 12 months of age: >5000 IU/day �Teens/adults: 50, ooo IU/week x 8 weeks �Consider Stoss therapy if compliance a concern (100, 000 – 600, 000 IU over 1 -5 days) Pediatrics 2008; 122: 398 -417
 Drops (8000 IU/m. L) Capsules")
Vitamin D Preparations �Ergocalciferol = D 2 (Drisdol®, Calciferol®) Drops (8000 IU/m. L) Capsules (50, 000 IU) Injection (500, 000 IU) – no longer available �Cholecalciferol = D 3 Capsules (5000 IU)

What about Calcium? ? � Simultaneous calcium supplementation necessary � Concern for “Hungry Bone” hypocalcemia � 30 -75 mg/kg/day divided TID – elemental calcium � Symptomatic hypocalcemia requires parenteral calcium replacement � Calcitriol (Rocaltrol®) can help treat hypocalcemia associated with rickets but does NOT build up vitamin D stores Pediatrics 2008; 122: 398 -417

Treatment Caveats �Vitamin D is fat soluble so must not overtreat Hypercalcemia ▪ Weakness ▪ Polyuria ▪ Nephrocalcinosis

Monitoring Therapy � 1 Month: Calcium, Phosphorus, ALP � 3 Months: Calcium, Phosphorus, ALP PTH, 25 OH Vit D, Urine calcium/creatinine ratio Recheck films �Check 25 OH Vit D at one year and then annually Pediatrics 2008; 122: 398 -417

Rickets Follow-up �Alk phos may increase initially due to increased bone formation �Healing is usually complete by 4 months �Lack of response to treatment may indicate a different etiology (or lack of adherence) �Once healed, continue a maintenance dose of at least 600 IU vitamin D daily (often more)

Reported Associations with Vit D Deficiency �Cardiovascular disease, BMI, Insulin resistance �Autoimmune disease �Cancers – breast, prostate, colon �Asthma �Schizophrenia, Mood disorders �Tuberculosis �Analogs used to treat psoriasis
D level? �No established reference range in children � 2008")
What is a normal 25(OH)D level? �No established reference range in children � 2008 AAP Review �IOM Report 2012 > 20 ng/ml �Endocrine Society 2011 CPG Deficiency < 20 ng/ml Insufficiency < 30 ng/ml

Prevention �Adequate dietary intake of calcium and vitamin D �Adequate sunlight exposure
 �Vitamin D supplementation (400 IU) for: Breast-fed or partially breast-fed")
AAP Clinical Report (2008) �Vitamin D supplementation (400 IU) for: Breast-fed or partially breast-fed infants beginning in the first few days of life Infants receiving <1000 ml formula/day (33 oz) Older children/adolescents who don’t obtain 400 IU/day of Vit D through diet (milk, other foods) �IOM Nov 2010 recommends 600 IU for children and adolescents (RDA) Pediatrics 2008; 122: 1142 -1152

Vitamin D Content �Breastmilk Vit D sufficient mother �Infant formula �Prenatal vitamins 15 -50 IU/L 400 IU

IOM Report: Dietary Reference Intakes for Calcium and Vitamin D �Released Nov 2010 �Supplementation for healthy infants, children, and adults �Prevention �Not treatment recommendations �Assumed little to no sun exposure
 �Children/Adolescents �Adults (19 -70 years)")
IOM – Vitamin D RDA �Infants (0 -12 months) �Children/Adolescents �Adults (19 -70 years) 400 IU 600 IU �Upper level intakes 0 -6 months 1000 IU 6 -12 months 1500 IU 1 -3 y/o 2500 IU 4 -8 y/o 3000 IU 9 -70 y/o 4000 IU IOM Report Nov 2010

IOM – Calcium per Day AGE RDA 0 -6 months 6 -12 months 1 -3 years 4 -8 years 9 -18 years Adults 19 -50 years 200 mg (AI) 260 mg (AI) 700 mg 1000 mg 1300 mg 1000 mg UPPER INTAKE LEVEL 1000 mg 1500 mg 2500 mg 3000 mg 2500 mg IOM Report Nov 2010
 � Cod liver")
Dietary Sources of Vitamin D � Fish oils (salmon, mackerel, sardines) � Cod liver oil � Liver and organ meats � Egg yolks 20 -25 IU/yolk � Fortified milk/juice 400 IU/L � Fortified cereals 40 IU/serving
 Plain low-fat yogurt Cheese Tofu Sardines Salmon")
Dietary Sources of Calcium SOURCE Milk (2%) Plain low-fat yogurt Cheese Tofu Sardines Salmon Spinach Almonds MG CALCIUM 285 Per cup 415 Per cup 220 Per oz 163 Per ¼ firm block 325 Per 3 oz 181 Per 3 oz 250 Per cup 126 Per 1/3 cup

Sunlight Exposure – Vit D �UVB 290 -315 nm – highest at 1200 noon (1000 -1500) �Minimal Erythema Dose (MED, slight pink skin) → 10, 000 -20, 000 IU vitamin D � 40% body to ¼ MED → approx 1000 IU vitamin D Pediatrics 2008; 122: 398 -417
 Poly-Vi-Sol® (400 IU/m.")
Vitamin D Preparations �Formulary Cholecalciferol = D 3 D-Vi-Sol® (400 IU/ml) Poly-Vi-Sol® (400 IU/m. L) 400 IU tab 1000 IU tab �OTC Most standard multivitamins (400 IU) Viactiv® chews (500 IU D 3/chew) Many other OTC vitamin D supplements

Calcium Preparations - Formulary �Calcium Carbonate – with food Oral suspension (500 mg/5 m. L) 500 mg tab 600 mg/tab + 400 IU D 3 �Calcium Citrate – absorbed with/without food 200 mg tab Citracal® (315 mg/tab + 250 IU vit D 3)

Calcium Preparations �Tums® Reg 500 mg/tab Extra Strength 750 mg/tab �Viactiv® chews (500 mg + 500 IU vit D 3)

Other Types of Rickets � 1α-hydroxylase deficiency �Vitamin D receptor mutation Associated alopecia totalis �X-linked hypophosphatemic rickets �Other inherited hypophosphatemic rickets

X-linked Hypophosphatemic Rickets �Renal phosphate wasting �Defective 1α-hydroxylase activity in kidney �Due to PHEX mutation increased levels of FGF-23 �X-linked dominant �Low serum phos, low/inappropriately normal 1, 25 -dihydroxyvitamin D �Treatment: phosphorous replacement, calcitriol (Rocaltrol®)

Key Points - Vitamin D �Prevention of vitamin D deficiency is key �Don’t forget about sunlight exposure �Supplement all breast-fed infants with 400 IU vitamin D within the first few days �Vitamin D RDA 600 IU for children and adolescents (IOM Report) �Vitamin D may be important for more than just bone health �If rickets is not responding to vitamin D treatment, consider other causes

PREP Question 1 �A 12 year old boy presents to your office for follow-up after his third wrist fracture in 3 years. As part of his evaluation in the emergency department, a complete metabolic panel was obtained and revealed a low calcium (7. 5 mg/d. L), low phosphorous (2. 8 mg/d. L), normal magnesium (1. 9 mg/d. L), and normal albumin (4 g/d. L).

PREP Question 1 �With the exception of his fractures, the boy has had no other medical problems and has not been taking any long-term medications. His height and weight are both at the 75 th percentile. His physical exam is unremarkable except for his casted left wrist. �Of the following, the MOST appropriate next step in this boy’s evaluation and management is to measure:

PREP Question 1 A. B. C. D. E. Ionized calcium Serum 1, 25 -dihydroxyvitamin D Serum 25 -hydroxyvitamin D Serum parathyroid hormone Urine N-telopeptide

PREP Question 2 �A 14 y/o boy suffers a nondisplaced fracture of his left radius and ulna while playing soccer. He had a similar injury to his radius and ulna 9 months ago. Physical exam reveals SMR 2 pubic hair and testicular volume of 6 ml. A thorough review of his dietary history suggests that his daily intake of calcium and phosphorous are 800 mg each. He takes 400 IU of vitamin D supplement daily.

PREP Question 2 �Serum calcium measures 7. 9 mg/d. L, serum phosphorous measures 2. 7 mg/d. L, and 25 hydroxyvitamin D measures 55 ng/m. L (normal 30 -80). �Of the following, the most appropriate recommendation for this boy is to increase his:

PREP Question 2 A. B. C. D. E. Calcium and phosphorous intake to 1300 mg/day Calcium and phosphorous intake to 2000 mg/day Calcium intake to 1000 mg/day Phosphorous intake to 1000 mg/day Vitamin D supplementation to 2000 IU/day

PREP Question 3 �A 7 -month-old child presents for a follow-up visit after undergoing a Kasai procedure for biliary atresia at 6 weeks of age. The mother states that the boy is irritable when his right arm is moved. On physical exam, the infant is jaundiced. You detect tenderness in the anterior radial head. Radiography of the affected region demonstrates metaphyseal fraying and a fracture.

PREP Question 3 �The MOST appropriate laboratory studies to obtain next are: A. Calcium, phosphorous, bone densitometry (DEXA scan) B. Calcium, phosphorous, urinary calcium-tocreatinine ratio C. Calcium, phosphorous, 25 -hydroxyvitamin D D. Calcium, phosphorous, magnesium E. Magnesium, phosphorous, parathyroid hormone

PREP Question 4 �You diagnose familial hypophosphatemic rickets in a boy who presents with rickets and whose mother had rickets as a child and required osteotomies as an adult. You explain to the parents that treatment can help the boy reach normal height and lessen his rachitic bone changes. �Of the following, the most appropriate treatment is:

PREP Question 4 A. B. C. D. E. Daily injections of human growth hormone and oral calcium twice daily Oral calcitriol once daily Oral calcium twice daily with oral cholecalciferol once daily Oral neutral phosphate salts every 6 hours with calcitriol once or twice daily Oral neutral phosphate salts once daily

References � � � * Misra M, Pacaud D, Petryk A, Collett-Solberg PF, Kappy M. Vitamin d deficiency in children and its management: review of current knowledge and recommendations. Pediatrics. 2008; 122: 398 -417. * Wagner CL, Greer FR. Prevention of rickets and vitamin d deficiency in infants, children, and adolescents. Pediatrics. 2008; 122: 1142 -1152. Institute of Medicine Report on Dietary Reference Intakes for Calcium and Vitamin D. Released 30 Nov 2010. Available at http: //books. nap. edu/openbook. php? record_id=13050. Holick MF. Vitamin D deficiency. N Engl J Med. 2007; 357: 266 -281. Adams JS, Hewison M. Update in vitamin D. J Clin Endocrinol Metab. 2010; 95: 471 -478. Carpenter TO et al. A clinician’s guide to X-linked hypophosphatemia. JBMR. July 2011; 26(7): 1381 -1388.
- Slides: 82