Urinary Tract Infection Dr Reham Almardini Urinary tract













 & AAP 2011, 2015 : VCUG should not be performed")













,")















 guidelines presume that few kidney defects")





- Slides: 63
Urinary Tract Infection Dr. Reham Almardini
Urinary tract infection In Childhood • Common problem: Risk of UTI is ~5% • 1% of boys and 1 -3% of girls • May be a marker of an underlying urinary tract abnormality • Cause significant long- term morbidity, renal scarring, hypertension & renal impairment • The risk of scarring is greatest in infants; in whom diagnosis is often overlooked or delayed because clinical features are non-specific
• The most common bacterial cause of UTI in children is Escherichia coli (UPEC), 80% of cases • Ascending UTI can lead to pyelonephritis, AKI, renal abscess, bacteremia • Chronically, UTIs can result in renal scarring, proteinuria, hypertension, and CKD
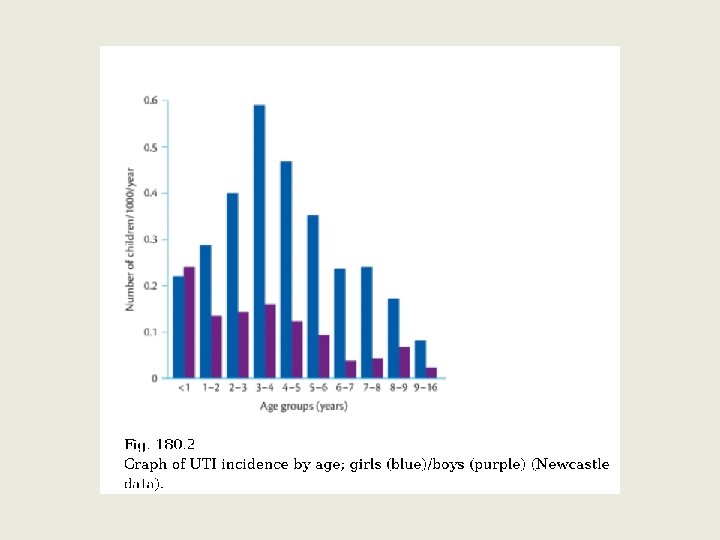
• 1 st yr of life, the male : female ratio is 2. 8 -5. 4 • Beyond 1 -2 yr, male : female ratio of 1 : 10 • Pyelonephritis is the most common serious bacterial infection in infants < 24 mo of age who have fever without an obvious focus
Urinary Tract Infection In Children • Delay in treatment is associated with an increased risk of scarring in susceptible children • Accurate & rapid diagnosis of UTI is essential and requires a very high index of suspicion particularly in the youngest • Scarring, once present, is irreversible and if severe may lead to chronic renal failure • Reflux nephropathy is probably the most important factor in the development of hypertension in children and young adults
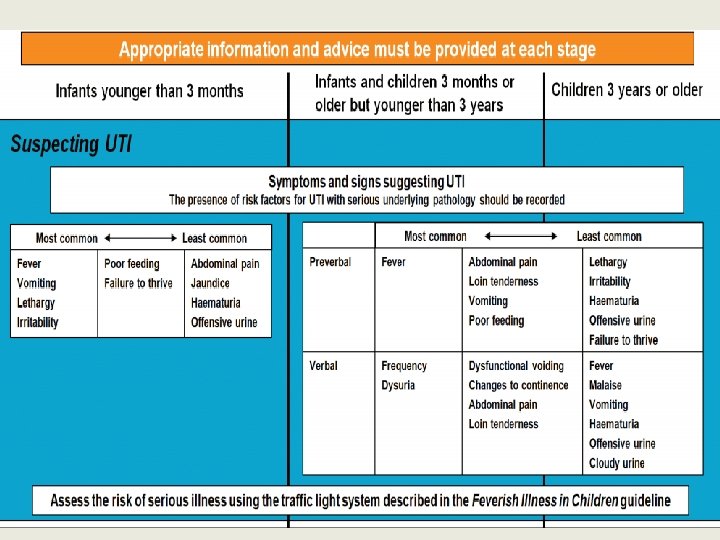
UTI Symptoms and Signs CYSTITIS PEYLONEPHRITIS • Hematuria, dysuria, frequency, Urgency, Hisitancy, Dripling, New Onset Enuresis • No fever or low grade • potentially severe, but « variable » • Suprepupic Pain and Tenderness expression • Signs in neoborn: non specific, Sepsis • High Fever, Chills, Vomitting , LOIN pain, Loin Tenderness • Leukocytosis • Acute phase reactantant • urine analysis
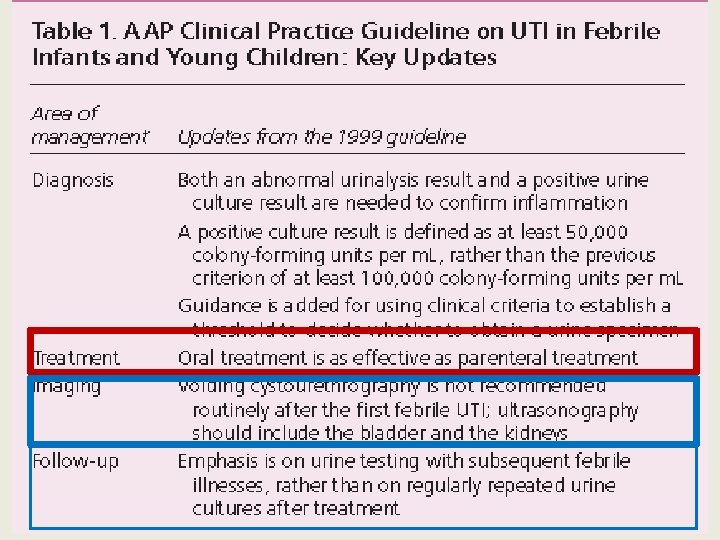
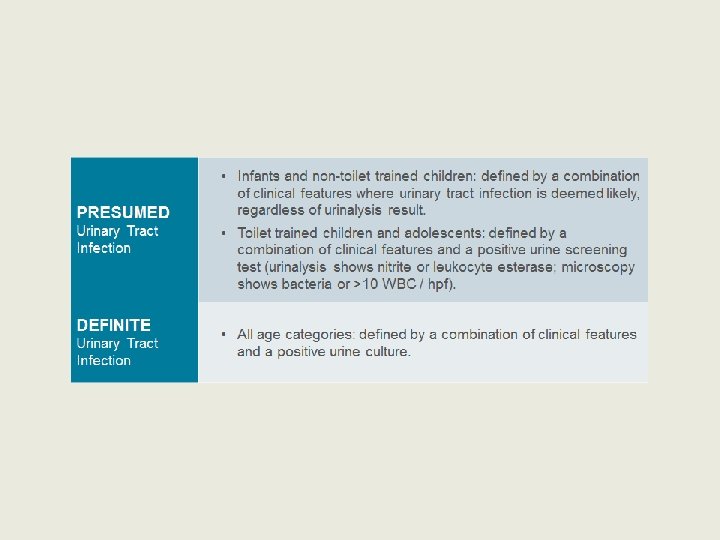
Criteria for Diagnosis of UTI • Both urinalysis results that suggest infection (pyuria or bacteriuria) & the presence of at least 50, 000 CFU/ m. L of a uropathogen cultured from a urine specimen obtained • Pyuria is a hallmark of true UTI and helps distinguish UTI from Asymptomatic Bacteruria • Change in this action statement is that the threshold criterion for a positive urinalysis result was reduced from 100, 000 to 50, 000 CFU/ m. L
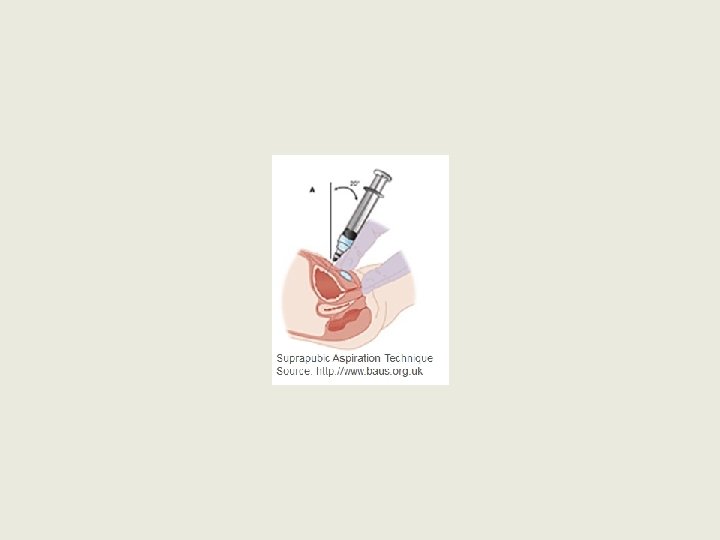
Urine sample collection • A clean catch urine sample is the recommended method for urine collection • when it is not possible to collect urine by non-invasive methods, catheter samples or suprapubic aspiration should be used • In an infant or child with a high risk of serious illness it is highly preferable that a urine sample is obtained; however, treatment should not be delayed if a urine sample is unobtainable
• Urine specimen should be obtained for both culture & urinalysis before an antimicrobial is administered • The specimen should be obtained by catheterization or suprapubic aspiration because the diagnosis of UTI cannot be established reliably by a culture of urine collected in a bag (Evidence Quality A)
Scaring After Initial UTI • In a meta-analysis 2010; the risk of renal scarring after an initial UTI in childhood was estimated to be 15% • About 50% in children having acute pyelonephritis and those with VUR being more likely to develop permanent scarring compared to those without VUR, and those with higher grade VUR more than those with lower grades
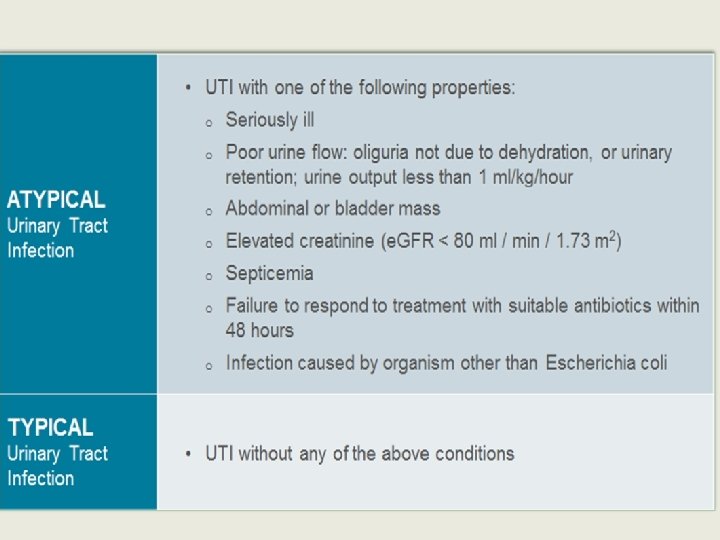
Atypical UTI • • • Seriously ill Poor urine flow Abdominal or bladder mass Septicemia Failure to respond to treatment with suitable antibiotic within 48 hours • Infection with non-Ecoli organism
Recurrent UTI • Two or more episodes with acute pyelonephritis/ upper urinary tract infection , or • One episode of UTI with acute pyelonephritis plus one or more episode of UTI with cystitis • Three or more episodes of cystitis • In six months periods
Simple versus complicated UTI • Complicated 1. Presence of fever > 39 C 2. Systemic toxicity 3. Persistent vomiting 4. Dehydration 5. Renal angle tenderness 6. Raised creatinine • Simple 1. Low grade fever Dysuria frequency urgency Absence of complicated UTI
• NICE 2007) & AAP 2011, 2015 : VCUG should not be performed routinely after first, febrile, UTI in patients less than 24 months old unless • RUS reveals abnormalities as HN, scarring or findings suggest high-grade VUR or obstructive uropathy • Atypical or complex clinical circumstances such as atypical/recurrent febrile UTI • In contrast, the American (2012) and European (2015) Urological Associations have continued to recommend performing a VCUG after first febrile UTI in children less than 2 years of age
NICE-2007 revised 2011 < 6 months
NICE…. 6 Months -3 Years
NICE…. . > 3 years
Urologic Imaging • Febrile infants and young children with UTI should undergo renal and bladder Ultrasonography
Urologic Imaging • VCUG should not be performed routinely after the first febrile UTI • It is indicated if kidney & bladder US reveals HN, scarring, or findings that suggest high-grade VUR & in other atypical or complex clinical circumstances • Further evaluation should be conducted if there is a recurrence of febrile UTI
Antimicrobial Therapy • Initiating treatment orally or parenterally is equally effective • The clinician should base the choice of agent on local antimicrobial sensitivity patterns (if available) • Should adjust the choice according to sensitivity testing of the isolated uro-pathogen
Treatment of children with urinary tract infection…. • Treatment of infection • Prevention of renal injury • Relief of the symptoms • Association between delayed treatment and increased risk of renal scarring • A ‘best guess’ antibiotic should be started whilst awaiting results of the urine culture, and antibiotics altered accordingly Coulthard et al. , 2014 a, Smellie et al. , 1985, 1994; Dick and. Feldman, 1996; Coulthard et al. , 2009
Parental Education and Follow-up • After confirmation of UTI, the clinician should instruct the child’s caregivers to seek prompt (ideally within 48 hours) medical evaluation for future febrile illnesses to ensure that recurrent infection can be quickly detected and treated (Evidence Quality C) • In the past, frequent follow-up cultures were recommended to identify asymptomatic recurrences. However, it is now recognized that this likely misidentified girls with asymptomatic bacteriuria as having recurrent or chronic UTI.
Usual indications for hospitalization and/or parenterally therapy include 1. Age <2 months 2. Clinical uro-sepsis (toxic appearance, hypotension, poor capillary refill) 3. Immunocompromised patient 4. Vomiting or inability to tolerate oral medication 5. Lack of adequate outpatient follow-up (eg, no telephone, live far from hospital) 6. Failure to respond to outpatient therapy
Empiric Antimicrobial Therapy • Early and aggressive antibiotic therapy (eg, within 72 hours of presentation) is necessary to prevent renal damage • Initiate immediately after appropriate urine collection in children who are at increased risk for renal scarring if UTI is not promptly treated: 1. 2. 3. 4. 5. Fever (especially >39°C [102. 2°F] or >48 hours) Ill appearance Costovertebral angle tenderness Known immune deficiency Known urologic abnormality
Type of Antibiotic for Empiric Therapy • Antibiotic that adequate cover E. coli. The agent of choice should be guided by local resistance patterns • Approximately 50% E. coli are resistant to Amoxicillin, Ampicillin High rates of E. coli resistance to first-generation Cephalosporins, TMP-SMX • Third-generation Cephalosporins & Aminoglycosides are appropriate firstline • Oral agents; Cefixime, Amox –Clav , Quinolones ( Pseudomonus) • Local microbiology advice is required about local resistance patterns • Recent antibiotic use, including prophylaxis, should also be taken into account when medication is chosen
Switch to oral antibiotics when the patient is tolerating oral fluids and has been afebril for 24 hours
Response to Antibiotic • In children who worsen or fail to improve within 48 hours of; 1. broadening antimicrobial therapy may be indicated if the culture and sensitivity results are not yet available. Enterococcus coverage by ampicillin or amoxicillin 2. RBUS to evaluate the presence of a renal abscess or surgically correctable anatomic abnormalities or obstruction • Repeat urine culture — Observational studies suggest there is little utility in children who are treated with an antibiotic to which their uropathogen is susceptible
NICE / Tips • For infants and children who receive aminoglycosides (gentamicin or amikacin), once daily dosing is recommended • If parenteral treatment is required and IV treatment is not possible, intramuscular treatment should be considered • If an infant or child is receiving prophylactic medication and develops an infection, treatment should be with a different antibiotic, not a higher dose of the same antibiotic. • Asymptomatic bacteriuria in infants and children should not be treated with antibiotics
• There is no evidence of benefit from treatment of Asymptomatic Bacteriuria in girls with normal urinary tracts
VUR grading
QUESTIONS
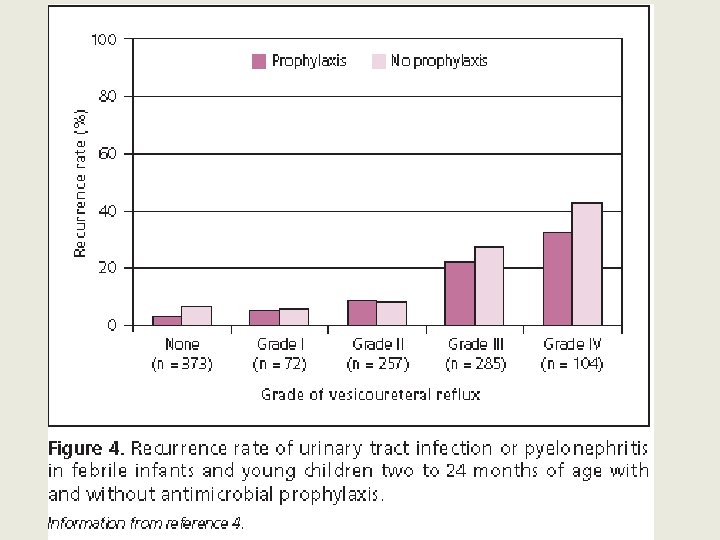
Prophylactic Antibiotic • Since 2006, six RCTs comparing prophylaxis with no prophylaxis. Data from all six trials were provided, resulting of 1, 091 children; • No statistically significant benefit could be demonstrated for prophylaxis in those without VUR or those with grades I to IV VUR (only five children with grade V were included in the trials)
Prophylactic antibiotics • Decisions for children following initial febrile UTI should be made on a case-by-case basis • 2011 AAP does not recommend prophylactic antimicrobials following the first febrile UTI in children 2 to 24 months • NICE antibiotic prophylaxis should not be routinely recommended following the first UTI, but may be warranted after recurrent UTI • For children who have no VUR but had a severe or protracted course of illness or have risk factors for recurrence (eg, febrile seizures, prolonged hospitalization, renal abscess, single kidney, bladder and bowel dysfunction), and in whom prevention of any recurrence would be desirable, we discuss the risks and potential benefits of antimicrobial prophylaxis with families
Follow UP; NICE • Infants and children who do not undergo imaging investigations should not routinely be followed up • The way in which the results of imaging will be communicated should be agreed with the parents • When results are normal, a follow-up outpatient appointment is not routinely required • Infants and children who have recurrent UTI or abnormal imaging results should be assessed by a paediatric specialist • Assessment of infants and children with renal parenchymal defects should include height, weight, blood pressure and routine testing for proteinuria
Follow Up • Infants and children with a minor, unilateral renal parenchymal defect do not need long-term follow-up unless they have recurrent UTI or family history or lifestyle risk factors for hypertension • Infants and children who have bilateral renal abnormalities, impaired kidney function, raised blood pressure and/or proteinuria should receive monitoring and appropriate management by a paediatric nephrologist to slow the progression of chronic kidney disease • Infants and children who are asymptomatic following an episode of UTI should not routinely have their urine re-tested for infection • Asymptomatic bacteriuria is not an indication for follow-up.
• multidrug resistance as non-susceptibility to at least one antimicrobial in three or more classes, based on in vitro antibiotic susceptibility testing • Extensively drug-resistant (XDR): isolates with susceptibility to only one or two antimicrobial classes, with resistance to agents in all remaining categories • Pan-drug resistance is resistant to all agents in all antimicrobial classes
ESBL • Beta-lactamases: ESBL producers hydrolyse penicillins, first- to third-generation cephalosporins and aztreonam but may remain susceptible to clavulanic acid combinations (e. g. amoxicillin/clavulanic acid) in vitro. • The most frequently cited risk factors are: previous antibiotic use, urinary tract anomalies previous hospitalization
Natural Course of VUR • Vesicoureteral reflux improves and resolves with time. The spontaneous resolution is higher in grades I and II and less in those patients with dilated VUR (grades III to V)
After 5 year • • 80% of grade II 46% of ureters with grade III 38% of patients with grade IV VUR had resolved in 50% of children (no VUR grading given) at the end of the 2 years follow-up • Pennisi, saw persistence of grade IV VUR in 52% of patients on prophylaxis at the end of 4 years of follow-up
How often does VCUG need to be repeated in a patient known to have VUR • VUR grade I and II, since VUR does not get worse with time, there is no need to repeat the VCUG but to continue aggressively treating episode(s) of recurrent UTI • Grade III to V, especially grade IV and V, and knowing that sterile reflux does not cause renal damage, VCUG may be repeated every 2 to 3 years to look for spontaneous resolution
• There is evidence that the vast majority of novel scarring takes place within the first few years of life, but there is also evidence • that scarring can occur at any age (Coulthard et al. , 2002).
THANK YOU
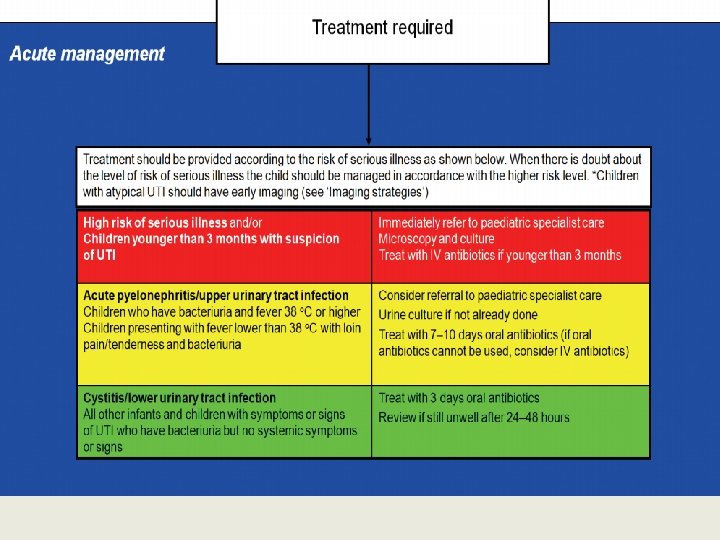
• Infants and children who have bacteriuria and fever of 38°C or higher should be considered to have acute pyelonephritis/upper urinary tract infection. Infants and children presenting with fever lower than 38°C with loin pain/tenderness and bacteriuria should also be considered to haveacute pyelonephritis/upper urinary tract infection. All other infants and children who have bacteriuria but no systemic symptoms or signs should be considered to have cystitis/lower urinary tract infection
• Recent childhood urinary tract infection (UTI) guidelines presume that few kidney defects can be prevented, and strive to minimise renal tract imaging. • All published childhood UTI guidelines advise prompt treatment, but none provide target times. • Treating children’s urinary tract infections in ≤ 3 days, more than halves the risk of them acquiring kidney scars. • GPs can halve the kidney scarring rates in young children by active management using a direct-access service.
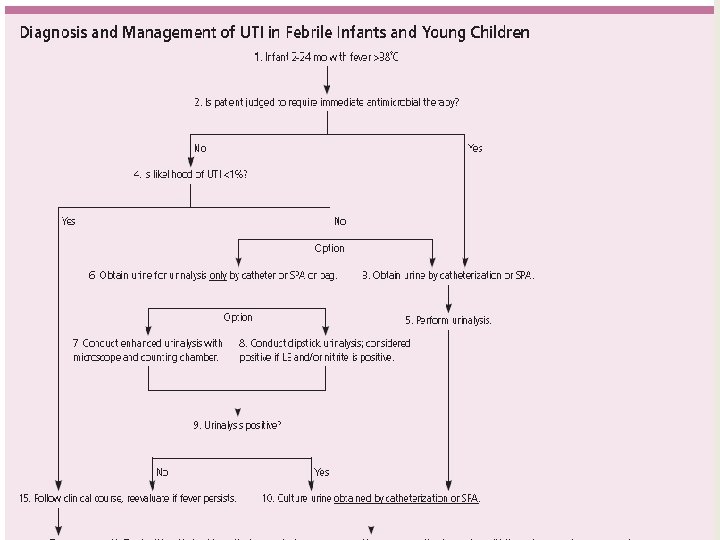
• Suitable urine sample for culture should be obtained before antimicrobials • A urinalysis helps interpret the results of the urine culture, to distinguish UTI from asymptomatic bacteruria • SPA is not recommended unless necessary • Urine dipstick is slightly less sensitive, but satisfactory if microscopy not available. Positive LE or nitrites or microscopy positive for WBCs or bacteria is a positive urinalysis • Base route on practical consideration, eg, unable to retain oral fluids • Pure growth of ≥ 50, 000 CFUs/m. L of a uropathogen and urinalysis demonstrating bacteriuria or pyuria • Sensitivities vary by region and time • Antimicrobial sensitivities should be used to adjust antimicrobial choice • Look for anatomic abnormalities that require further evaluation • Proven UTI, RBUS indications for VCUG should be judged by the clinician. • After a second UTI, the risk of grade IV-V VUR, is estimated to be 18% • Evaluation ideally within 48 h. Early detection and treatment of febrile UTI may reduce the risk of renal scarring.
NICE guideline for paediatric UTI • Aim: To reduce the numbers of referrals and imaging procedures undertaken as part of the care of children with UTIs
Resistance to ampicillin were the highest and nitrofurantoin rates lowest,
Revised AAP Guideline on UTI in Febrile Infants and Young Children 2011 2 months infant up to 24 month toddler with unexplained fever • The recommendations summarized 2012 in American Family Physician article. The new guideline is based on an extensive literature review
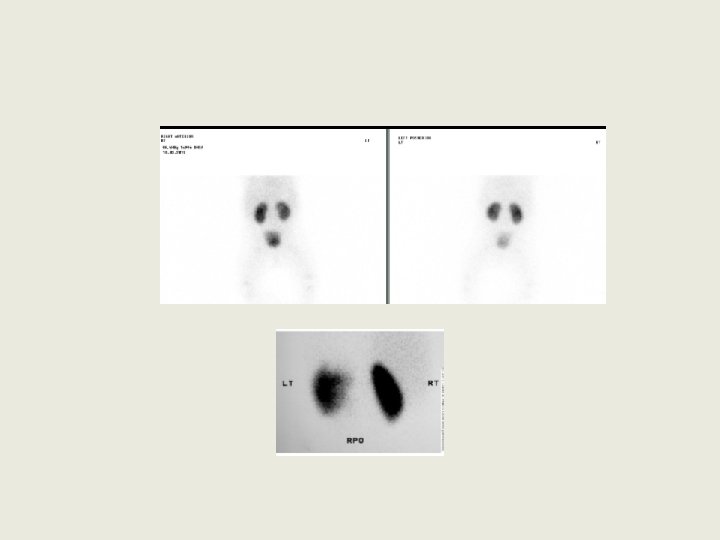
Management of a child with a febrile urinary tract infection become controversial. • The old model investigations : • Ultrasound , DMSA , and a voiding cystourethrogram VCU or MCUG • The aim was to identify child with VUR or any uptake defect on the nuclear images. (old model ) • Children with VUR of any grade were treated with prophylactic antibiotics. • All children with a febrile UTI : hospitalized for intravenous treatment with antibiotics. 63