Dermatologic Consequences of HIV Infection Dr Arjan Hogewoning



")

 Natural Courses of HIV Infection symptoms 1000 clinical")









































 • Increase of several cytokines")



 • Exaggerated responses to insect")











- Slides: 76
Dermatologic Consequences of HIV Infection Dr. Arjan Hogewoning MD Dermatovenereologist Korle Bu Teaching Hospital Akai house clinic Accra, Ghana TM
Agenda • Introduction • Relation HIV/Dermatology • HIV and skin infections (viral, bacterial, fungal) • HIV and other skin diseases • Discussion
CD 4 -count (dells per µL) Natural Courses of HIV Infection symptoms 1000 clinical latency constitutional symptoms 800 opportunistic diseases: tuberculosis, lymphoma Candidiasis, herpes KS, PCP Toxoplasmosis Cryptosporidiosis 600 400 200 acute HIVinfection weeks CMV, MAI years death 0 1996
HIV Related Skin Diseases • Impairment of the skin immune system is responsible for both infectious and non infectious skin diseases, even before the development of full immunodeficiency
HIV Related Skin Diseases • Impairment of the immune system, a well recognised consequence of pharmacological immunosuppression , leads to microbial and malignant invasion
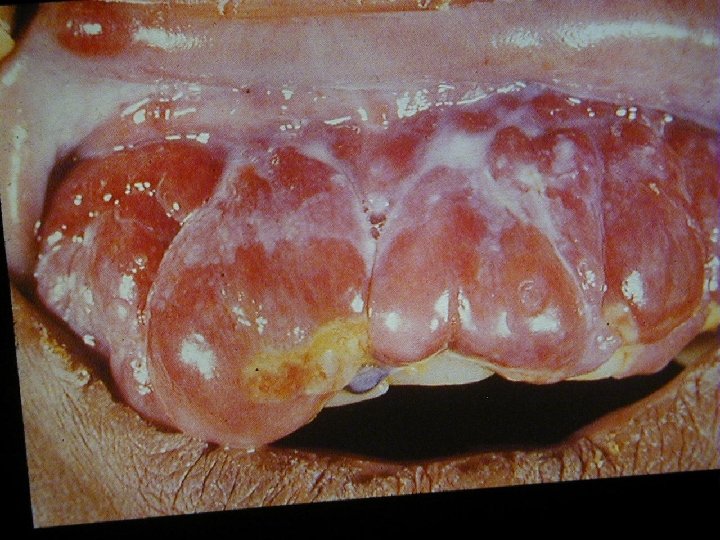
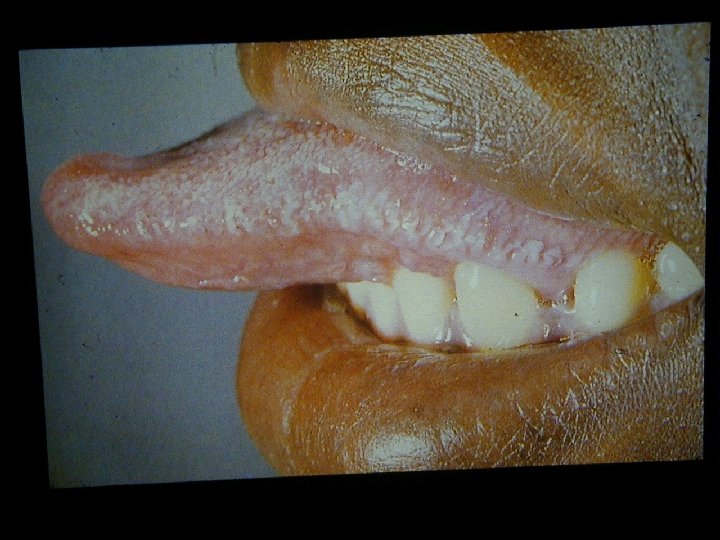
HIV Related Skin Diseases • Diseases of the skin and mucous membranes are among the first recognised clinical manifestations of AIDS • More than 90% of patients develop skin or mucous membrane conditions at some time during their diseases • Often the skin is the first organ affected
HIV Related Skin Diseases • Primary mucocutaneous signs of HIV infection • Viral, Bacterial, Fungal infections • Miscellaneous disorders – – Seborrhoic dermatitis Deteriorating of existing dermatoses like psoriasis or eczema Pruritus Adverse cutaneous drug reactions • Tumors – Non Hodgkin lymphoma – Basal cell carcinoma, Melanoma – Kaposi Sarcoma
Proportion of HIV- attributable Tuberculosis in the World Estimates for 1990, 1995, 2000 Estimated cases (million) 10. 2 m 12 10 8 8. 8 m 7. 5 m 6 4 2 0 4. 2 m 1990 8. 4 m 13. 8 m 1995 2000 HIV-attributable Tuberculosis Programme/WHO Not related to HIV
Herpes Infections • • Herpes Simplex Virus 1 Herpes Simplex Virus 2 Epstein-Bar Virus Cyto Megalo Virus Varicella Zoster Virus Humane Herpes Virus 6 Humane Herpes Virus 7 Humane Herpes Virus 8
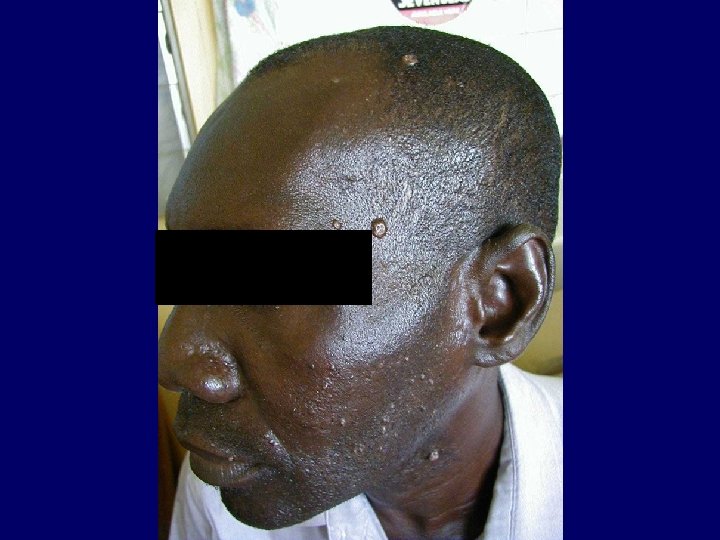
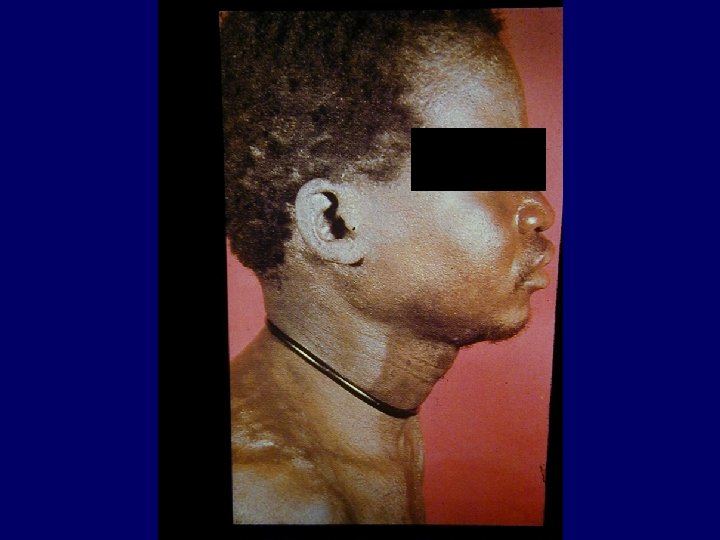
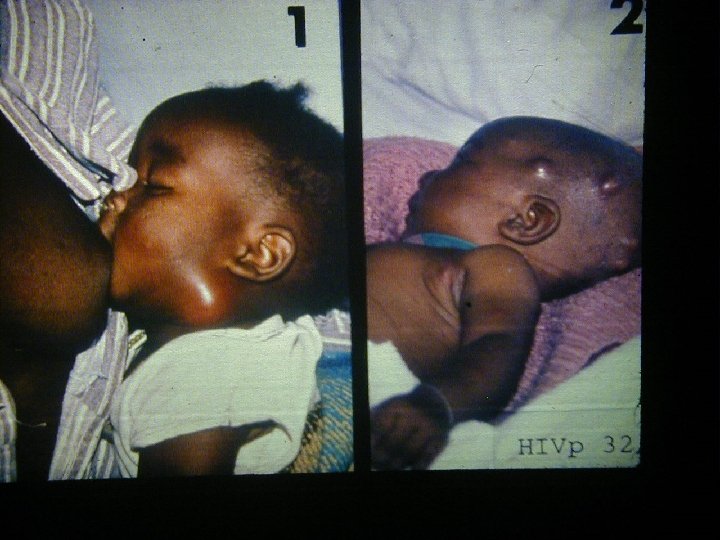
Varicella Zoster • Primary VZV infection in HIV infected children is often severe (dissemination, pneumonia, encephalitis, pancreatitis) • Frequency of reactivation of latent VZV leading to Herpes Zoster is greatly increased for HIV infected persons • Herpes Zoster can occur at any stage of HIV disease but presents often in the beginning
Varicella Zoster • The decrease in CD 4+ cell function is not solely responsible for the increased Herpes Zoster risk • CD 8+ cells may also play an important role in reactivating VZV and are known to increase early in HIV infection
Kaposi Sarcoma • Classical Kaposi sarcoma • African endemic Kaposi sarcoma • Latrogenic, immunosuppressive, drug associated Kaposi sarcoma • AIDS-associated, epidemic Kaposi sarcoma
Xerosis Cutis • Weight loss and cachexia (nutritional deficits) • Increase of several cytokines like IFN-Alpha, TNF, IL-1 and IL-6 • IFN-Alpha and TNF alter lipid metabolism (increase levels of triglycerides and decrease cholesterol) • The lipid metabolism in the epidermis is changed and leads to transepidermal water loss
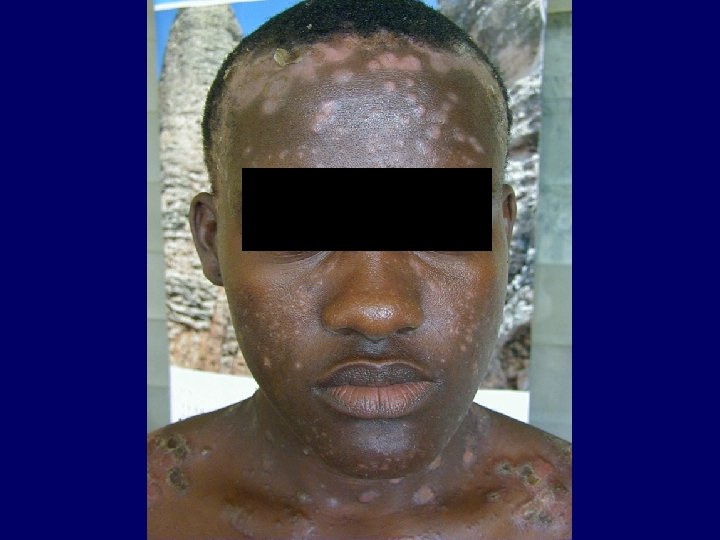
Pruritus • A common complaint in HIV infected patients • Multitude of disorders and microorganisms may give rise to pruritus
Causes of Pruritus • Folliculitis (Staphylococcus Aureus and Pityrosporum) • Exaggerated responses to insect bites • Sarcoptes Scabiei • Adverse cutaneous drug eruptions • HIV related asteatosis • HIV associated eosinophilic folliculitis • Ill defined HIV related pruritic papular eruptions