Module 4 HIV Infection in Women HIV Infection

























 (2001). A guide to the clinical care of")
. Recommendations for Use")
. Clinical Nursing Series. Nursing Care of the")
- Slides: 29
Module 4 HIV Infection in Women
HIV Infection in Women • Garrett Colmorgen, MD, Director Maternal Fetal Medicine, Christiana Care Health Services, Wilmington, Delaware • Staff of the Pennsylvania/Mid-Atlantic AIDS Education & Training Center, Delaware Local Performance Site - P. Lincoln, N. Bennett, M. A. Bartkowski
Demographics of HIV in Women • Fastest growing group in the United States • 4 th leading cause of death aged 25 to 44 in the United States • Disproportionately affects African Americans & Hispanics living on the eastern seaboard CDC-2000
Statistics of HIV in Women • Cumulative Statistics as of December 2000 in the United States 074, 997 African American 028, 151 White 025, 643 Hispanic 01, 133 Other • Total 130, 104 CDC 2000
HIV Transmission Risk Behaviors for Women • Heterosexual - 62% 0 African American - 63% 0 White - 18% 0 Hispanic - 18% 0 Other - 1% 0 primary risk behavior for all age groups of women • IVDU - 35% • Other - 3% CDC 2000
Female Condom • “Reality” - only brand currently marketed in the US • Made of polyurethane, sheath closed at one end with flexible rings at both ends Anderson, J. 2001
Microbicides • Strategy enabling women to have control over safer sex/prevention of HIV • Nonoxynol-9 increases risk of HIV infection • Clinical trials of topical microbicides are being conducted Anderson, J. 2001
Gender Bias Transmission • More efficient from man to woman than woman to man • Related to number of infectious particles in body fluid • Related to volume of fluids exchanged • Related to surface area coming in contact with infected body fluid HRSA: BPHC & AETC
Risk Factors for Male to Female HIV Transmission • Anal Intercourse • Lack of male circumcision • Genital ulcers (syphilis, herpes simplex, chancroid) • Sexually Transmitted Diseases • Multiple sexual partners
Special Consideration • Early Adolescent 0 immaturity of the female genital track increases risk of transmission • Women over 50 years of age 0 atrophic vaginitis caused by decreased lubrication 0 older females are generally not perceived to be at risk
Natural History of HIV Disease in Women • Same as in men except for GYN symptoms and disease conditions • 1993 CDC added invasive cervical cancer as an AIDS defining condition • Women are often diagnosed late • Women may have barriers to care HRSA: BPHC & AETC
Challenges in Caring for Women with HIV • Statistically economically poorer than men • More likely to be single parents 0 lack of child care 0 lack of support • More likely to be uninsured HRSA: BPHC & AETC
Signs and Symptoms of HIV in Women • Acute Seroconversion - (No distinct gender differences however many of these s&s often go under addressed) 0 fever 0 swollen glands Bartlett, J. 1999
Signs and Symptoms of HIV in Women cont’ 0 Rash - macular or maculopapular, usually nonpururitic. Truncal / facial distribution can involve arms and legs. Often appears several days past onset of fever. 0 Fatigue 0 Mono-spot test is negative 0 Bartlett, J. 1999
HIV-Related Gynecological Conditions • • • Vaginal candidiasis Human Papilloma Virus Genital Ulcers Pelvic Inflammatory Disease Cervical Dysplasia/Neoplasia Menstrual Disturbances HRSA: BPHC & AETC
Diagnostic Studies • Pap smear 0 two studies the first year of diagnosis 0 annually if normal 0 recommended every 6 months if HIV is symptomatic • Colposcopy USPHS/IDSA 2001
Prenatal & Family Planning HIV Screening • DHHS guidelines suggest universal HIV testing with patient notification as a routine component of prenatal care • Pre and post test counseling & informed consent - laws vary by state USPHS/IDSA 2001
Pregnancy • Does not appear to accelerate HIV infection
Perinatal HIV Transmission May Occur • Antepartum 0 during pregnancy • Intrapartum 0 during labor 0 during delivery • Postpartum-through breast feeding HRSA: BPHC & AETC
Reducing Perinatal Transmission • ACTG 076 0 women given AZT after first trimester 0 AZT administered intravenously during labor 0 newborn receives AZT for 6 weeks 0 transmission reduced by 67. 5% • Combination therapy has reduced the rate even further HRSA: BPHC & AETC
Antepartum/Intrapartum Management Considerations • • Avoid amniocentesis Avoid premature rupture of membranes Avoid fetal scalp monitoring Delay episiotomy HRSA: BPHC & AETC
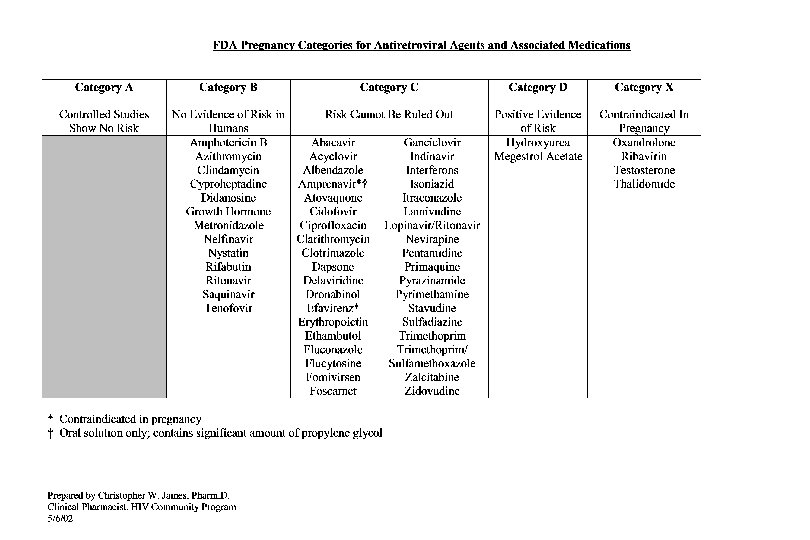
HIV Medications to avoid during Pregnancy • Efavirenz - associated with anencephaly, anopthalmia Neural tube defects in primates • Indinavir - Potential for nephrolithiasis and neonatal hyperbilirubinemia De. Lorenzo, L. 2001
HIV Medications to avoid during Pregnancy, cont’ • Didanosine/Stavudine - combination associated with fatal lactic acidosis in pregnancy • Stavudine/Retrovir -combination is antagonistic, decreasing efficacy of therapy De. Lorenzo, L. 2001
Antiretroviral Pregnancy Registry • Collaborative effort between the CDC, NIH and pharmaceutical companies to monitor for birth defects in infants exposed to antiretroviral agents • antiretroviral exposure during pregnancy should be reported to the registry at 1 -800 -258 -4263 Anderson, J. 2001
Current Prevention Message-Is it Reality ? • • • Abstinence Monogamy Reduce number of partners Ask partner about history of infection Enforce use of condoms Colmorgen, G. 1999
References • Anderson, J. (Ed. ) (2001). A guide to the clinical care of women with HIV. Rockville, MD: HIV/AIDS Bureau, Health Resources and Services Administration. [Available on-line: http: //www. hab. hrsa. gov/publications. html]. • Bartlett, J. & Gallant, J. (2001). 2001 -2002 Medical Management of HIV Infection. [Available on-line: http; //hopkins-aids. edu
References, cont’ • Center for Disease Control and Prevention. (2002, February). Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1 -Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV 1 Transmission in the United States. [Available on-line: http: //www. hivatis. org. ]
References, cont’ • De. Lorenzo, L. (2001). Clinical Nursing Series. Nursing Care of the HIV-Infected Patient. Fourth Edition. Western Schools Press.