Urinary tract infections UTI ewa demidowicz Urinary tract


 source of infections regarding")














 Nelaton’s B) Couvelaire’s C) Tiemanna’s D) Malecot’s E) Pezzer’s")
















, pyuria (-), symptoms (-)")
 Acute")
")

















 Vesicoureteric reflux is a developmental anomaly of vesicoureteric junctions. Urine reversion from the")


 Posterior urethral valve (PUV) disorder is an obstructive developmental anomaly")
 Ultrasonograph test result PUV surmise Bilateral widening")













- Slides: 74
Urinary tract infections UTI ewa demidowicz
Urinary tract infections Definition: Presence of germs in urinary tract above the urinary bladder sphincter
Epidemiology the second Urinary system forms (after the respiratory system) source of infections regarding their frequency. Urinary system infections are the cause of about 5% of pyrexic episodes in the case of children <1 year of age UTI occurs in approximately 8% of girls and 2% of boys below 7.
Epidemiology Below the third of month of life, there is a 5 -6 times greater dominance of male sex, which may enventuate from a higher frequency of the occurence of urinary system malformations. Above the 8 th month grows the number of urinary infections among girls In the case of females, urinary infections develop 10 -50 times more frequently than in the case of men.
Etiology Most frequently Gram-negative bacteria 80 -85% Echerichia coli
Etiology • • Apart from that, in cultures are also found: Proteus mirabilis (most commonly found under the prepuce) Klebsiella, Enterobacter, Morganella morgani, Pseudomonas aeruginosa Gram positive bacteria - Staphylococcus: Staph saprophyticus characterisic for teenage girls, - Streptococcus spp: UTI mainly in the case of newborns
Epidemiology – other Fungi – candida albicans, especially after a long-term antibiotic therapy, immunosuppresive treatment, and application of cytotoxic agents Viruses – adenovirus, causes hemorrhagic cystitis Chlamydia trachomatis – such etiology should be taken into consideration in the case when aseptic leukocyturii is accompanied by suppurative leakage from the urethra Trichomonas vaginalis – newborns/infants
98 % of all infections develops in ascending tract. urethra- bladder – kidney. UTI is usually result of bowel flora entering the urinary tract via the urethra 1% of urinary infections develops through blood, together with septicaemia.
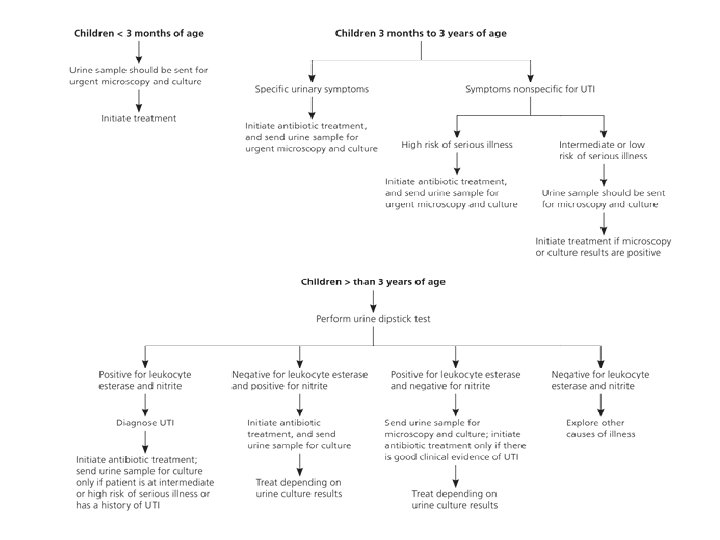
symptoms 1. Newborns and children <3 month Untypical Symptoms vomiting, diarrhoea, apetite loss, prolonged jaundice, anxiety, polyuria In severe conditions symptoms of general infection Only in 40% UTI of children <3 month fever is present !
symptoms 2. Children from 3 months to 3 years Fever, apetite loss, nausea , vomiting, stomach pain, weight gain inhibition, anxiety/pain accompanying urination, change of colour and smell of urine Rare classical symptoms of dysuria • (bladder tenesmus, frequency, pain and burning while urinating)
Symptoms 3. Children >3 years. Symptoms characteristic for urinary tract infections = dysuria, fever, abdominal pain Pyelonephritis – fever >38, 5 degrees, pain in lumbar region, positive Goldflam’s symptom Cystitis – fever <38, 5 degrees, dysuria, without the pain in lumbar region or the Goldflam’s symptom • ! In the case of children with recurrence the course is most commonly asymptomatic.
Diagnostics: Laboratory tests 1. Urinalysis/ Urine culture 2. Complete blood count, white blood cell count 3. Markers of inflammation (C Reactive Protein, procalcitonin) 4. Radiological investigations !!! physical examination , anamnesis,
Recommended ways of urine collection • 1. A ‘clean-catch’ midstream specimen • a urine specimen obtained after the external urethral area is washed with a liquid soap and rinsed well; then the patient starts a urinary stream, stops it and voids into a sterile specimen container. The purpose of obtaining such a specimen is to minimize contamination by external organisms. ! The reliability of urine culture for the method - 45% • •
Recommended ways of urine uptake 2. Bladder cannulation – if there is urgency in obtaining a sample and no urine has be passed • ! The reliability of urine culture for the method - 90% 3. Suprapubic aspiration – fine needle attached to a syringe is inserted directly into a bladder just above symphysis pubis under ultrasound guidance. It is an invasive procedure rarely used in the case of newborns and infants below the 3 rd month of life ! reliability of the method - 97%
• 4. An adhesive plastic bag applied to the perineum after washing. • !!! There may be contamination from the skin. • !!! reliability of the method - ? ? ? lack • !!! method is not recommended
Bladder cannulation 1. Diagnostic cannulation – serves the purpose of urine uptake for urine culture, mainly in the case of younger girls, allows for avoiding abnormalities connected to impurities in urine specimen 2. Cannulation with the purpose of performing diagnostic examination cystourethrography of urine and urinodynamic examinations 3. Cannulation with therapeutic purpose- urination obstruction or anuria
Bladder Cannulation 1. 2. Contraindications Suspicion of a possible urethra traumatic injury, characterized by bleeding from urethra (crutch injury, pelvis injury, dull stomach injury) Haematoma of the crutch region
Different kinds of catheters A) Nelaton’s B) Couvelaire’s C) Tiemanna’s D) Malecot’s E) Pezzer’s F) Foley’s 1 – urine draining port and canal 2 – balloon’s port and canal
A. Nelaton’s Catheter With one side slot May be used for one-time cannulation as well as for holding for several days B. Couvelaire’s Catheter • straight with slots at the side and end • used for draining urine while bleeding, which requires bladder rinsing, the best choice to allow urine outlet C. Tiemanna’s Catheter • with folded end • mainly used in the case of boys, especially with posterior urethral valve, who not only have a contraction within the valve, but also an distended bladder and raised bladder cervix • Catheter should be inserted by directing the bended end of the catheter towards the head
D+E. Melcot’s and Pezzer’s Catheter • Used for guaranteeing correct urine discharge in the case of patients after surgeries F. Foley’s Catheter • Self-maintanable catheter used for long-term bladder draining • the balloon should be filled with sterile water (as saline may become crystalized)
Rules for choosing the right kind and size of catheter Age Boys Girls Catheter Newborns 4 F 4 -6 F Nelaton 1 -2 years 6 F 6 -8 F Nelaton, Foley, Tiemann 3 -5 years 8 F 8 -10 F As above 6 -10 years 8 -10 F 10 -12 F As above >10 years 12 F 12 -14 F As above Catheter size is defined according to French scale, which determines the catheter’s circuit in milimeters. 1 F equals approximately 0, 33 mm, so a 9 F circuit equals approx. 3 mm.
Urine screening test DIPSTICK testing Used as a screening test for urinary infections, diabetes, kidney diseases or kidney complication resulting from hypertension. With a multi-parameter test strips (dipstick) it is possible to evaluate the presence of : erythrocytes, bacteria, leukocytes, protein, glucose, acetone bodies, bilirubin, urobilinogen, ascorbic acid, as well as state p. H and urine’s specific gravity. • Urine test strip consists of several testing fields which react with specific urine components. Drowning the strip in a test-tube causes chemical reactions occurence which results in the strip’s colour change. Quantitative analysis is carried out with test-stripes analyser which evaluates the intensity of the colour of testing fields.
The parameters of the test strip : Leukocytes: in the presence of leukocytes in urine indicates leucocyte esterase activity - an enzyme found in granulocytes and macrophages Nitrites: a positive result indicates UTI caused by Gram-negative bacteria, reducing present in the urine of nitrate to nitrite, Bilirubin: increasing its excretion occurs, in case of hyperbilirubinaemia. The result of bilirubin can be overestimated in the presence of chlorpromazine metabolites and the downside in the presence of vitamin C in urine, urinary nitrites and exposure to sunlight. Urobilinogen: increasing its concentration in urine occurs when excessive amounts of bilirubin in the blood, eg. In hemolytic jaundice or to impaired urobilinogen portal circulation due to the damage of hepatocytes or liver cirrhosis. No urobilinogen in urine shows the complete cholestasis Ketones are intermediate metabolites transformation of fats and proteins. The presence of ketones in the urine confirms ketoacidosis, which may be associated with diabetes, fever, vomiting, diarrhea or pregnancy. Glucose, its presence is confirmed impaired resorption in the distal tubules, increased blood glucose (diabetes, glucose intolerance). False negative results we observe at high concentrations in the urine of vitamin C, ketones, and the p. H <5 of urine. Ascorbic acid, the presence of vitamin C in urine affect the result of the analysis, causing undervaluation result of leukocytes, nitrite, glucose, and bilirubin.
General urinalysis Leukocyturia - definition Pathological number of leukocytes in urine sediment: more than 5 leukocytes not spinned urine, and more than 10 leukocytes in spinned urine Addis’ number 2, 5 -5 mln leukocytes per 24 hours(norm); Hamburger’s number 1500 -3000 leukocytes per minute
Urine Culture– detecting urinary tract infections Bacteriuria is stated on the basis of urine culture examination only when the number of colonies from the culture per 1 ml of urine amounts > 10 E 5 or less (if symptoms of urinary tract infection are observed). Depending on the method of collecting urine: Urine draw from the mid stream >=10 E 5 in the case of girls >10 E 4 in the case of boys Bladder catheterization >10 E 5 – definite diagnosis 10 E 3 -10 E 5 – possible diagnosis Draw through suprapubic centesis any number of G-negative bacteria, >10 E 3 G-positive bacteria
It is very unusualin the case of children with urinary tract infections to observe a negative result of culture examination. Most commonly the phenomenon is observed in the case of inborn urinary tract malformations (e. g. infection within the cyst or a total blockage of urinary tract) or when the culture is carried out while antibiotic therapy is in progress.
Radiological investigation in the case of urinary tract infections Purpose – exclusion of urinary tract malformations - evaluation of infection extent. National Institute’s for Health and Clinical Excellence guidelines suggest carrying out radiological investigation in the case of children with the highest risk of kidney damage and urinary tract malformations To this group the followig cases are qualified: Stymied urine outlet, - Palpable resistance within abdomen - Increased creatinine concentration - Sepsis - Lack of response to antibiotic treatment Infections caused by bacteria other than E. Coli Children with recurring urinary tract infections
1. Ultrasonography Urinary tract structure evaluation (kidney location, kidney abscess, calcium deposits, dilatation of the renal pelvis and calyces and urether widening, thickened bladder wall)
Renal scintigraphy Diagnostic test enabling accurate evaluation of kidney structure (detects functional defects, such as scars created after the infllamation) as well as their excretory function. The test is carried out after an intravenous injection of radiological marker (99 m. Tc). The isotope is abstracted by kidneys and than transmitted to the bladdder together with urine. Such examination enables evaluation of kidneys’ dynamics. The only contraindication for scintigraphy is pregnancy. Isotope examinations include: • dynamic tests (based on the evaluation of radioactivity course change in time (evaluation of particular renograme phases). • static tests (analysis based on the evaluation of radioactivity distribution) In the case of static scintigraphy the result is the image of radioactivity distribution within kidney ‘s pulp, which allows for the evaluation of the kidney’s structure. In the case of dynamic scintigraphy, the radioactivity pattern depicts kidney’s functions. It enables excretion evaluation , obstructive uropathy and hydronephrosis detection. • Radioactivity change in time curve, is called a renograme. It consists of 2 basic parts: - vascular phase, - excretory phase,
Renal scintigraphy • The accumulation mechanism of this marker is not exactly known. • The marker is accumulated in active cells of proximal ducts – thus it marks their functional state. • Marker accumulates within the cells gradually, 1 hour after application, around 50% of the applied amount, gather within the kidney. • The marker stays within the kidney’s pulp for about 24 hours. • The result of scintigraphy is read 2 -4 hours after the marker’s application.
Clinic use of radioisotopic tests Kidneys’ function - each kidney functioning evaluation, regional evaluation of kidney’s functions. Abnormalities in urine outlet - evaluation of kidneys’ activity, - diagnosing abnormalities in urine outlet. Reflux nephropathy: - kidneys’ functioning evaluation, - diagnosing reflux. Diagnosing post-inflamatory scars, Kidney’s injury: - evaluation of the kidney’s perfusion, - diagnosing discontinuation of urinary tract – urine leakage. - Acute kidneys’ failure: blood-flow evaluation, - evaluation of kidneys’ functions return. Kidney tumor: - diagnosis of the so called pseudo-tumor / cancer Inborn kidney malformations
Micturating Cystouretrography Indications: After every infection in the case of all newborns and infants After severe infections in the case of older children • ( acute pyelonephritis) In the case of recurring infections of urinary tract - in the case of other malformations diagnosed during other imaging tests (ultrasonography, scintigraphy, urography) - in the case of children suffering from nocturnal enuresis
Micturating Cystouretrography The test is based on the introducing of a catheter into the bladder. Then through the catheter a contrasting agent is being passed. After filling the bladder, the catheter is removed and the distal portion of the test is performed during micturition. In the test, the shape of bladder and urinary tract is made visible thanks to the introducing of the contrasting marker. The accuracy of bladder emptying during urination is evaluated. The test allows for determinig whether an abnormal reflux of the contrasting marker to the ureter and kidneys appears. during the test are performed X-rays It is necessary to carry out X-rays of a full bladder, as well as the moment of urinating and the condition of urinary tract after urination. Most commonly 2 -4 Xrays are taken, however depending on the course of the test, the number of photos taken may be increased.
Clinical Forms of urinary tract infections Asymptomatic bacteriuria bacteria (+), pyuria (-), symptoms (-) Asymptomatic infection bacteria (+), pyuria +, symptoms (-) Symptomatic infection of the lower urinary tract (bladder, urethra) Acute/long-term pyelonephritis
Clinical forms of urinary tract infections 1. Infections with kidney’s tissue occupancy A) Acute pyelonephritis - fever >38, 5 st - pain in lumbar region - stomach pain - in 25% cases, dysuria - significant bacteriuria B) Urosepsis - symptoms similar to pyelonephritis - severe general condition - symptoms of general infection - culture – the same microbes in blood and urine C) Long-term pyelonephritis - usually accompanies urinary tract malformations - scars in kidneys’ tissue - hypertension - symptoms of kidney failure •
Clinical forms of urinary tract infections 2. Infections of the lower urinary tract A) Symptomatic infection of the lower part of urinary tract - dysuria - temp <38, 5 st - leukocyturia - significant bakteriuria B) Asymptomatic infections of urinary tract - leukocyturia - significant bacteriuria C) Asymptomatic becteriuria - two fold, diagnosis of the same microbe in culture
Acute urinary tract infection – treatment Children <3 rd month of life - require hospitalization - parenteral antibiotic therapy 10 -14 days in the case of infants, newborns up to 21 days • Children >6 month with a severe disease course - possible use of sequencial treatment (3 days of perenteral antibiotic therapy, next oral antibiotic therapy. )
Microbe - treatment Gram-negative bacteria microbe Intravenous therapeuticals Oral therapeuticals Amoxicillin/clavulanate 90 mg/kg/24 h divided every 8 hours Amoxicillin/clavulanate 90 mg/kg/24 h divided every 12 hours Amoxicillin 90 mg/kg/24 h diveded 8/12 h Enterobacteriaceae Cefuroxime 150 mg/kg/24 h divided every 8 hours Cefuroxime axetyl 30 mg/kg/24 h divided in 2 doses Ceftriaxone 50 -75 mg/kg/24 h in one dose Cefotaxime 150 mg/kg/24 h in 3 doses Trimethoprim/sulfamethoxazole 8 -12 mg /kg mc/24 hdivided every 12 hours Ceftazidime 150 mg/kg/24 h divided every 8 hours Pseudomonas aeruginosa Quinolone should not be used in children under eighteen Piperacillin + Tazobactam 112, 5 mg/kg/dose, 3 times per day + Aminoglycoside
Gram-positive bacteria Ampicillin 200 mg/kg/24 h divided every 6 hours Ampicillin 200 mg/kg/24 hdiveded every 6 hours Enterococci Vanoomycin 40 mg/kg/24 h + Gentamycin in newbornor children with immune deficiency Streptococcus gr B Ampicillin 200 mg/kg/24 h divided every 6 hours
Preventative treatment ? ? ? In the case of about 20% of children who underwent a urinary tract infection, a symptomatic infection recurrence occurs However, it is still not known what is the probability of avoiding a clinically significant kidneys injury by preventing urinary tract infections Most likely, the probability is really low, the risk of kidneys injury seems unlikely , and thus the benefits of preventative treatment appear insignificant.
Prophylaxis? ? ? Usually in the case of children with a bladder-ureteral reflux or with a recurring urinary tract infection antibacterial therapeuticals in small quantities were given in order to prevent further infections Medaical data confirming the legitimacy of such treatment is insufficient In 2009 results of a 600 -children examination with reflux were published. The results show that children whoo were treated for 12 months with small quantities of cotrimoxazol did not benefit much from the teratment in comparison to the placebo group Before making a decision about preventative treatment, the insignificant decrease of the risk (from 19 to 13%) of the infection recurrence should be taken into acconut. What is more, the negative outcomes of such a treatment, namely bacteria resistance development in the case of infection recurrence, should also be considered.
Prophylaxis! Routine prophylaxis after the first urinary tract infection episode is not advised Preventative treatment with antibacterial therapeuticals should be considered in the case of children included in the so called high-risk group, namely the youngest infants, children with urinary tract malformations as well as those with recurring urinary tract infections. •
Urinary tract infections - complications Systemic infection Abscess formation within kidney tissue Post-inflammatory scars appearance
Prognosis In the case of 6 -23% of patients with bladder-ureteral reflux and scars in kidneys, hypertension is diagnosed The presence of scars multiplies the risk of hypertension development three-fold, in comparison to children without scars The frequency of a persistent kidney disease occurence on the grounds of an undergone acute pyelonephritis reaches 5 -6%
Urinary tract malformations
Inborn urinary tract malformations Definition: inborn malformations of urinary tract and kidneys are abnormalities arising from embryogenesis disfunction on different levels, which explains their phenotypic diversity The following are included: - kidneys malformations(aplasia, hypoplasia, displasia, duplications) - abnormalities in urine draining tract (ureter duplication, macro-ureter, vesicoureteral reflux) - urethra malformations (posterior urethral valve)
Epidemiology Inborn kidney and urinary tract malformations occur in 1 of 500 live births Malformations are the cause of 30 -43% cases of terminal kidney failure Malformations are responsible for 60% of cases of persistent kidney diseases
Kidneys malformations 1. Inborn absence of both kidneys - occurs rarely -1: 4000 births, more frequently with boys - Newborns are not able to live extrauterinally independently, mailny because of the lungs hypoplasia caused by reduce volume of amniotic fluid , which also causes child’s face deformation ( flat nose, drawn-back chin, low ears, epicanthus). Intrauterine pressure causes also crooked deformations of limbs as well as joint contractions.
Kidneys malformations 2. Inborn absence of one kidney - Occurs in 1: 1300 births More frequent with males and involves the left kidney Usually accompanied by ureter absence and bladder triangle hypoplasia Is the cause of a compensatory kidney hyperplasia on the opposite side In approx. 41% of cases a vesicoureteral reflux is diagnosed.
Kidneys malformations 3. Kidney Hypoplasia Means lowering proper nephron number - Occurs in 1: 600 -800 births, more frequently with girls - Hypoplastic kideny is small, has a lower number of calyxes and narrowed blood vessels - May be one- , or less frequently two-, sided -
Kidneys malformations 4. Kidney displasia - Presence of embryonal structures is characteristic, which may come from vascular, nephroblastic or uretheral primordium. - The organs have different sizes, which depends on the presence of cysts. - It includes: multi-cyst displasia, oligomeganephronia (nephrone hypoplasia as well as decrease in the number and overgrowth of nephrones)
Kidneys malformations - 5. Kidney Ectopia Unusual kidney location Occurs with the frequency of 1 in 1000 births Depending on its location, pelvic, hip and lumbar kidney may be observed. The displacement (ectopia) is usually accompanied by incomplete rotation
Kidneys malformations 6. Inborn hydronephrosis - Widening of the renal pelvis and calyces caused by difficulties in urine drain - Belongs to the most commonly diagnosed malformations of urinary tract - May be caused by: posterior urethral valve, urethral obstruction, vesicoureteric reflux, neuropathic bladder
(VUR) Vesicoureteric reflux is a developmental anomaly of vesicoureteric junctions. Urine reversion from the bladder to the ureter, or even kidney Develops as a result of an abnormal bladder-ureter junction or may be secondary to the obstacle below the bladder – urethral obstruction VUR may be hereditary, in 50% of children whose mothers had VUR during childhood, or in 40% of children whose siblings suffer from VUR destroys kidneys – outlet nephropaty occurs, progressive scarification of kidneys, more frequently in the case of children with one urinary tract infection, or with urinary tract infections recurrence. More frequently the outlet is observed in the ureter draining the lower region of the duplicated kidney. VUR accompanies, in 50% of cases, the neuropathic bladder.
Vesicoureteric reflux An international 5 -degree classification is used for describing VUR FIRST DEGREE – reflux to an unwidened ureter SECOND DEGREE – to renal pelvis and calyces, without any widening THIRD DEGREE – benign or sedate widening of the ureter, renal pelvis and calyces FOURTH DEGREE – mildly twisted ureter course, renal pelvis and calyces widening with minimum flattening of their canopy FIFTH DEGREE – twisted course and severe widening of the ureter, renal pelvis and calyces, thinning of renal cortex
The 1 st and 2 nd degree of the reflux subsides spontaneously after conservative therapy. A persistent anti-inflammatory prophylaxis is used. Degrees 3 rd-5 th require surgical intervention which means endoscopic treatment. Scars are visible in renoscintigraphy in 15% in the case of low refluxes, and in 65% in the case of the high ones. Long-term observation proves the occurence of hypertension and persistent kidney failure as a result of discharge nephropaty.
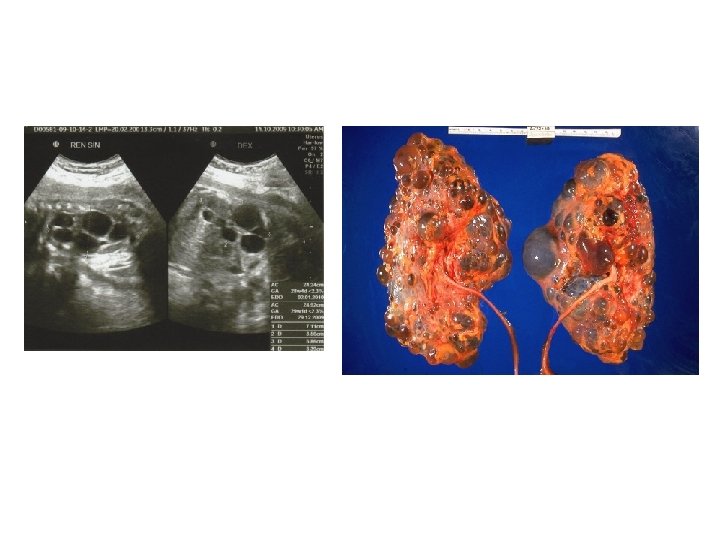
Posterior urethral valve (PUV) Posterior urethral valve (PUV) disorder is an obstructive developmental anomaly in the urethra and genitourinary system of male newborns Incidence is from 1 in 5 000 to 1 in 12 500 Anatomically, it is an overdeveloped mucous membrane fin in the membranous urethra between septum and seminal colliculus It causes in-bladder pressure increase, widening of the posterior valve, detrusor muscle overgrowth , Vesicoureteral reflux, macro-ureters. May coexist with an inborn kidneys displasia Characteristic syndromes include: Bilateral widening of the upper urinary tract ( bilateral hydroureteronephrosis) small, thick-walled bladder, widened posterior urethra , Oligohydramnios, Increased echogenicity of kidneys
Possibility of diagnosing posterior urethral valce (PUV) Ultrasonograph test result PUV surmise Bilateral widening of the upper urinary tract (bilateral hydronephrosis) fetus’s enlarged bladder High probability of PUV Bilateral widening of the upper urinary tract ( bilateral hydroureteronephrosis) enlarged, thick-walled bladder dilated posterior urethra („key-hole” syndrome) Very high probability of PUV = PUV diagnosis Bilateral widening of the upper urinary tract ( bilateral hydroureteronephrosis) enlarged, thick-walled bladder dilated posterior urethra („key-hole” syndrome) Oligohydramnios Increased echogenicity of kidneys
Prenatal diagnosis elements Standard prenatal diagnosis procedure in the case of a correct pregnancy includes three phases: Examination between the 11 th and the 14 th week of pregnancy, Between 18 th. and 22 nd. between 30 th. and 34 th. Ultrasonograhy of the fetus is the key test which enables confirming the pregnancy and the normality of fetus development, as well as detecting inborn malformations of single systems and organs. The first test of the urinary tract is intended to evaluate teh presence of kidneys pulp and bladder, The second test enables accurate evaluation of the pulp’s structure, widening of the urinary tract and the amniotic fluid volume. The third test serves the purpose of malformation evaluation and enables makig the decision about the place and way of the delivery.
Polish Society of Children’s Nephrology constituted a group of experts which developed guidelines for doctors involved in post-natal diagnosing of inborn urinary tract malformations The document is intended for neonatologists, peadiatricians and general doctors who are the first in line to plan the diagnostic procedure on the grounds of a pre-natal screening.
General guidelines 1. ultrasound is the basic test for diagnosing inborn malformations of the urinary tract in the case of children in the pre-natal and post-natal period. 2. in the case of a newborn or infant with urinary tract malformation suspicion, ultrasonography screening should be carried out by a qualified specialist, and in suitable conditions. 3. Delivery of a baby with a severe urinary tract malformation suspicion should be carried out in a referential unit of a 3 rd level, providing peadiatric urologist and nephrologist consultation.
General guidelines 4. It is suggested that in the case of all children with a prenatal urinary tract malformation suspicion, an ultrasonography screening of the abdomen should be carried out within the first 7 days of life. The time of the test is determined by the condition of the child and the kind of the suspected malformation. (urgent test within the 1 st and 2 nd day, planned test within the 3 rd and 7 th day). 5. Proceeding schemata should be determined on the basis of the next abdomen ultrasonograph screening which should be carried out within 4 -6 weeksafter the first test.
Specific guidelines 6. If the pre-natal ultrasonograph test demonstrated an isolated singleor double-sided widening of the urinary tract, and there is no suspicion of a compound malformation. The delivery and preliminary post-natal verification of the malformation may be carried out in a community hospital. 7. A significant widening of the urinary tract that requires monitoring is understood as the widening of the renal pelvis in anteroposterior diameter (A-P)by over 5 mm in 3. – 7. day of life and 10 mm in 4. – 6. week of life or later. 8. in the case of an isolated, uncomplicated, single- or double-sided widening of the urinary tract, there are no indications for micturating cystourethrogram.
Specific Guidelines 9. After confirming the diagnosis of a widened urether, the newborn shuld be directed to children; s nephrology or urology unit with the aim of carrying out further diagnostic tests. 10. Diagnosing macro-ureter on the grounds of a post-natal ultrasonograph test in the case of a child who did not have a confirmed widened urether in the pre-natal period, is also an indication for directing the patient to further diagnostic tests. 11. Further diagnostics includes micturating cystourethrogram with the aim of specifying the etiology of the malformation and renoscintigraphy with the aim of assessing kidneys functions.
Specific guidelines 12. In the case of posterior urethral valve suspicion catheterization is necessary in order to decompress the urinary tract and draw material for tests (urinalysis, culture). Ultrasound screening should be carried out as urgent in order to evaluate the urinary tract, Within prophilaxis antiobiotic therapy should be implemented as well as a regulation of all hydro- electrolyte disorders. A newborn should be transferred to a specialist children’s urology or nephrology unit with the aim of further diagnosing and therapy. Optionally, (before the transfer) an evaluation of kidneys may be carried out (after the second day of life).
Specific guidelines 13. Diagnosing hyperechogenic kidneys is the basis for advising delivery in a specialist perinatologist unit. 14. A newborn with isolated kidneys echostructure disorders requires kidney function evaluation (creatinine concentration in serum) and an ultrasound test between the 3 rd and the 5 th day of life. 15. Infants with normal test results (ultrasound, kidney functioning evaluation) carried out between the 4 th and the 6 th day of life probably do not require further diagnosing.
Specific guidelines 16. Bilateral kidney agenesia suspicion as a lethal inborn malformation, requires urgent verification at a unit equipped with adequate technical resources and massive experience in the field of pre-natal diagnostics. 17. Delivery of a newborn with bilateral kidney agenesia suspicion should be planned in a referential unit providing intensive infant therapy care, diagnostic screening with the use of a wide range of testing techniques and kidey-substitute therapy. 18. In the process of pre-natal diagnosing and deciding on the possibility of kidney-substitute therapy implementation, a peadiatric nephrologist should be involved.
Specific guidelines 19. In the case of diagnosing kidney pulp absence and a correct amniotic fluid volume during pre-natal testing, there are no indications for extended dioagnosing or therapeutical intervention in the pre-natal period. 20. In the case of a clinical examination of a newborn, a special attention should be given to the possible coexistence of malformations within genital organs 21. First ultrasonograph in the case of a child with a diagnosed cystdisplasia of both kidneys should be done within 24 -48 hours after delivery. 22. Monitoring ultrasound test in the case of a child without a diagnosed cyst-displasia of kidneys suspected in the pre-natal period, should be carried out with the aim of final disqualification of the malformation within 4 -6 week of life. An ultrasonograph test carried out in the first 2 days of life gives a falsely negative result.
Specific guidelines 23. Monitoring ultrasonograph test in the case of a child without any pre-natally diagnosed isolated kidneys cysts should be carried out in the 6 th month of life. 24. Monitoring ultrasonograph test in the case of a child with diagnosed isolated kidneys cysts and a positive family history of kidneys cysts, should be carried out every 6 -12 months.
Conclusions 25. Pharmacological prophylaxis of urinary tract infections in the case of newborns with a pre-natal suspicion of urinary tract malformation is not advised. However, urinary tract infections occurence should be monitored till complete diagnosing has been completed. The only exception are children with Posterior urethral valve suspicion and a massive bilateral widening of the urinary tract, who require diuresis monitoring. Those children should be included in a pharmacological urinary tract infections profylaxis, till a full diagnosis of the urinary tract is complete. 26. After diagnostic catheterization, newborns should be treated with anti-bacterial medicines for up to 3 days.
Conclusions 27. Early identification of urinary tract malformations and their treatmant have basic significance. 28. In the case of newborns and infants with urinary tract malformation kidneys efficiency evaluation is of a great significance, especially in the case of boys with a bilateral urinary tract widening. 29. Special attention should be given to the urinary tract infections prophylaxis, detection and early treatment, blood pressure monitoring and hypertension treating as well as modification of pharmaceuticals advised with urinary tract infections depending on kidneys efficiency.