Urinary Tract Infection UTI Urethral Terrorist Incident UTI
 Urethral Terrorist Incident? 鲍一歌 四川大学华西医院")








. Risk of pyelonephritis")






 • Hematuria • And")




 • Chlamydia trachomatis • Mycoplasma (Ureaplasma urealyticum) • Fungi")
 • Klebsiella")





")
 A")
 • By hiding inside the cells,")



 • Different strains of pathogen, re-enter the urinary tract")







 • Short")
 • stasis and obstruction:")

 •")












- Slides: 66
Urinary Tract Infection (UTI) Urethral Terrorist Incident? 鲍一歌 四川大学华西医院
UTI: a quick view • Definition of UTI • Presence of pathogen in the urinary tract and invasion and reaction of the urinary tract to the disease producing organisms and their toxins. The reaction usually includes inflammation of the involved organ. • Key: Bacteria + inflammation
UTI: a quick view • The inflammation cause by pathogenic microorganism involving any parts of genitourinary tract. • These infections can spread from a given locus to any or all of the others.
UTI sites Necrotizing papillitis Renal abscess Renal carbuncle Perinephric abscess • Pyelonephritis Pyonephrosis • Cystitis Prostatitis Epididymitis Urethritis
Pathways of pathogen infect urinary tract: 1. Ascending route Most common cause 2. Hematogenous spreads To kidney, prostate, testis Usually are straptococcus 3. Lymphatogenous spreads Through the lymphatic channels from the neighbor infection 4. Direct extension from another organ Intraperitoneal abcesses like Appendiceal abcess.
UTI: a quick view • UTIs are the most common infections just secondary to those involved respiratory system. • Women are especially prone to UTIs, One woman in five develops a UTI during her lifetime. Why? • UTIs in men are not so common, but they can be very serious when they do occur. Why?
UTI in a nutshell • Typical clinical scenario • Young female • Dysuria, frequency • Urianalysis • WBC +++ • Nitrite +ve • Urine C&S • Escherichia coli growth • Resistant to all beta lactams and beta lactamase inhibitor except carbapenems • Rx • Levofloxacin 500 mg qd po x 3 d
UTI in a nutshell • Typical clinical scenario • Young female • Dysuria, frequency • Urianalysis • WBC +++ • RBC + • Nitrite +tive • Urine C&S • Escherichia coli growth • Resistant to all beta lactams and beta lactamase inhibitor except carbapenems • Rx • Levofloxacin 500 mg qd po x 3 d
1. Female UTI: more common and more recurrence • Short urethra • Shorter route for bacteria to enter the bladder • Antimicrobial effect of urine • Close to vagina & anus • Reservoirs • Men are less common in UTI, but more likely to have recurrence after the 1 st episode. Why?
UTI in other population: more complicated • Pregnancy: asymptomatic bacteriuria (5%). Risk of pyelonephritis and miscarriage. Screen at 1 st trimester • Senior male: asymptomatic bacteriuria, intertwisted with BPH • Pediatric: more likely to become pyelonephritis, screen for congenital abnormalities (VUR etc)
UTI in a nutshell • Typical clinical scenario • Young female • Dysuria, frequency • Urianalysis • WBC +++ • Nitrite +ve • Urine C&S • Escherichia coli growth • Resistant to all beta lactams and beta lactamase inhibitor except carbapenems • Rx • Levofloxacin 500 mg qd po x 3 d
Clinical Manifestation of UTIs: Could be asymptomic in some chronic infections. • Abnormal urination: Vesical irritability: frequency, urgency, burning Difficulty of urination • Abnormal urine: Reddish urine, Bloody urine, Hematouria Milky, cloudy urine, pyauria, bacteriuria • Pain: Local pain and referred pain • GI tract symptoms: Nausea, vomitting, etc. • Systematic symptoms: Fever, chills, headache, etc. Bacteremia, toxicemia, sepsis, infectious shock
Cystitis vs. pyelonephritis: manifestation Cystitis: localized Pyelonephritis: generalized • Bladder irritation/ lower urinary tract symptoms (LUTS) • Dysuria • Frequency, urgency • Fever, chills, nausea and vomiting • Myalgia and malaise • Risk of urosepsis • Local: flank pain, CVA tenderness, dysuria and frequency
LUTS vs. bladder irritation symptoms: Very similar LUTS: sphincter/detrusor dysfunction Bladder irritation: inflammation • Core symptom: difficult urination • Core symptom: dysuria storage symptoms: frequency, urgency, dysuria voiding symptoms: hesitancy, post-void dribbling other: suprapubic pain, hematuria, foul-smelling urine
Clinical manifestations • 3 components: symptoms, bacteriuria, pyuria • Symptoms + bacteriuria + pyuria = Symptomatic UTI • (location? Acute or chronic/recurrent? ) • Bacteriuria only = Asymptomatic bacteriuria • Pyuria only = healthy or stone or cystitis or bladder cancer etc. • Symptom only = interstitial cystitis etc.
UTI in a nutshell • Typical clinical scenario • Young female • Dysuria, frequency • Urianalysis • WBC +++ • Nitrite +ve • Urine C&S • Escherichia coli growth • Resistant to all beta lactams and beta lactamase inhibitor except carbapenems • Rx • Levofloxacin 500 mg qd po x 3 d
Urianalysis 尿常规 • Look for evidence of pyuria (WBC counts) • Hematuria • And bacteriuria • Nitrite • Bacteria in urine pellets
Bacteriuria or contamination? Bacteriuria • > 105 CFU/ml on voided samples • > 102 CFU/ml on catheterized/ suprapubical aspiration • 103 – 105 CFU/ml: suspicisous • Common microbes: E. coli, enterococcus Contamination • Microbes from external genitals during sample collection • S. aureus, S. epidermidis, mixed flora • < 103 CFU/ml
UTI in a nutshell • Typical clinical scenario • Young female • Dysuria, frequency • Urianalysis • WBC +++ • Nitrite +ve • Urine C&S • Escherichia coli growth • Resistant to all beta lactams and beta lactamase inhibitor except carbapenems • Rx • Levofloxacin 500 mg qd po x 3 d
What bacteria causes UTI? • Common pathogens for cystits • These bugs “KEEPS” KEEPS you busy • Klebsiella sp. (克雷白杆菌属) • E. coli (most common), other Gram-negatives • Enterococci (肠球菌属) • Proteus mirabilis (奇异变形杆菌), Pseudomonas (假单 胞菌属) • S. saprophyticus (腐生葡萄球菌)
Special pathogens • Tuberculosis (TB) • Chlamydia trachomatis • Mycoplasma (Ureaplasma urealyticum) • Fungi (Candida)
What bacteria causes UTI? Community-acquired UTI • Most common: E. coli (85%) • Klebsiella (克雷白杆菌属 ) • Enterococcus fecalis (粪 肠球菌) • Staphylococcus saprophyticus (腐生葡 萄球菌) • Proteus mirabilis (奇异变 形杆菌) Hospital-acquired UTI • Most common: E. coli (3050%) • Enterococcus (肠球菌属) • Klebsiella (克雷白杆菌属 ) • Citrobacter (柠檬酸细菌 属) • Seratia (赛氏杆菌属) • Pseudomonas (假单胞 菌属)
Hospital acquired UTIs • 35~50% in total hospital acquired infection, again just secondary to respiratory infection. • Among them, 75~80% caused by catheterization • Bacteria usually have high resistance to antibiotics, so the infection could be very severe. • Catheter Care: • Choice of catheter: appropriate size • Drainage system: closed, not open drainage • Clean or sterile of urethral openning.
How do bacteria enter the bladder? • Rectum -> vagina -> periurethral perineum -> urethra • Activities that increase the risk • Simple movement of underwear • Wiping from back to front after a bowel movement • Sexual intercourse • diaphragm with a spermicide • delayed postcoital micturition
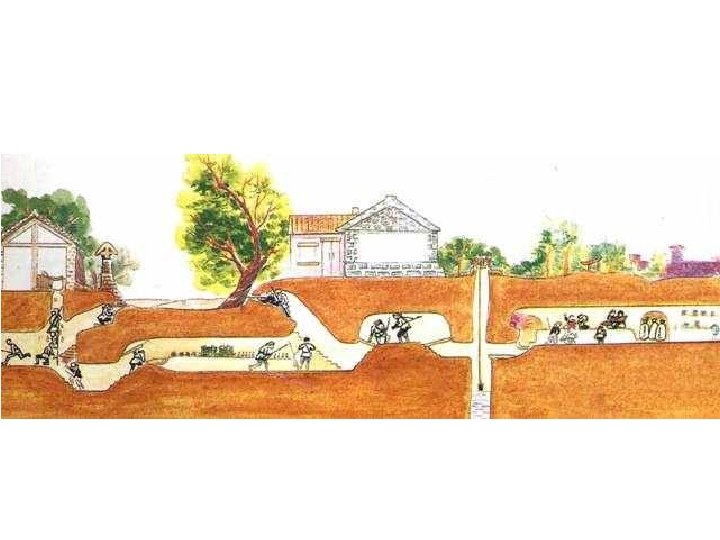
Reservoir: war trench for bugs!
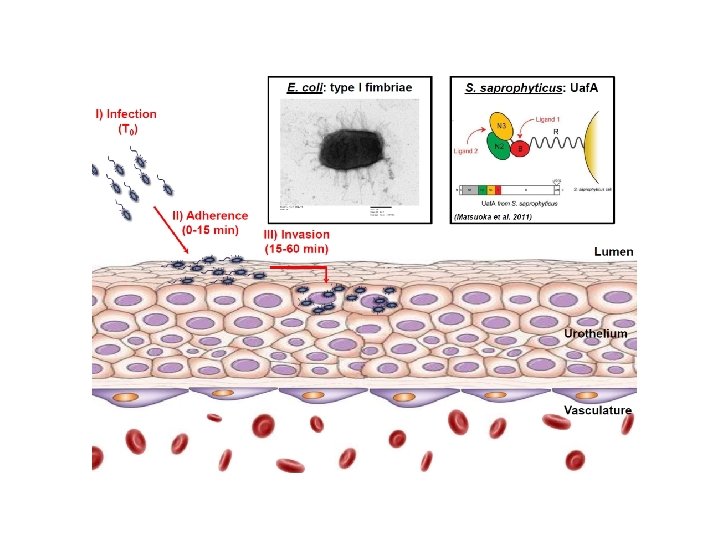
Bacterial invasion, adhesion, and colonization Host defence mechanism • Urine flushing • Shedding of urothelia Bacterial colonization mechanism • Adhesion to surface • Form intracellular bacterial community Factors promoting host defence • Increased water intake • Frequent urination Factors promoting bacterial colonization • Foreign body • Anatomical abnormaly • Urinary stasis/obstruction/reflux
Host defence: Urine • Osmaolarity • Urea concentration • Organic acid concentration • Acidic p. H value
Bacterial invasion, adhesion, and colonization • Uropathoge nic E. coli expresses fimbrae (or pili) to adhere to urothelia
Factors promoting bacterial colonization Bacteria adhering to foreign body (ureteral stent and stone) A patient with anatomical abnormaly (Ureteral duplication)
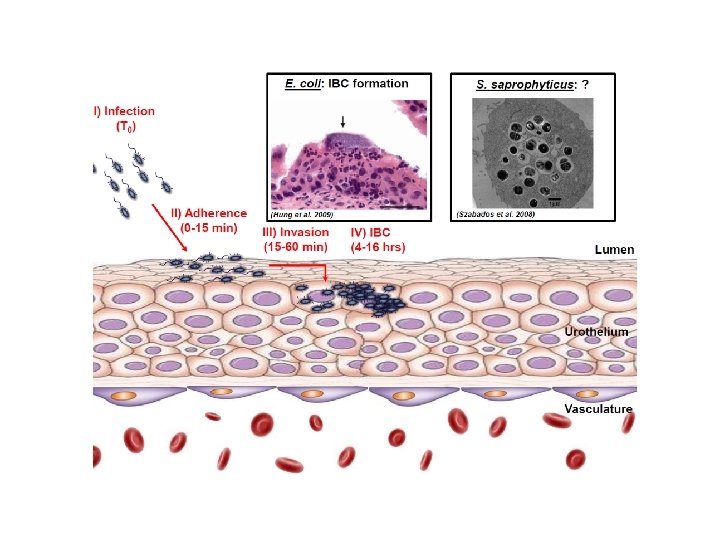
Some bacteria could form intracellular bacterial community (IBC) • By hiding inside the cells, the bacteria are able to escape from host immune defence and luminal antibiotics
IBC
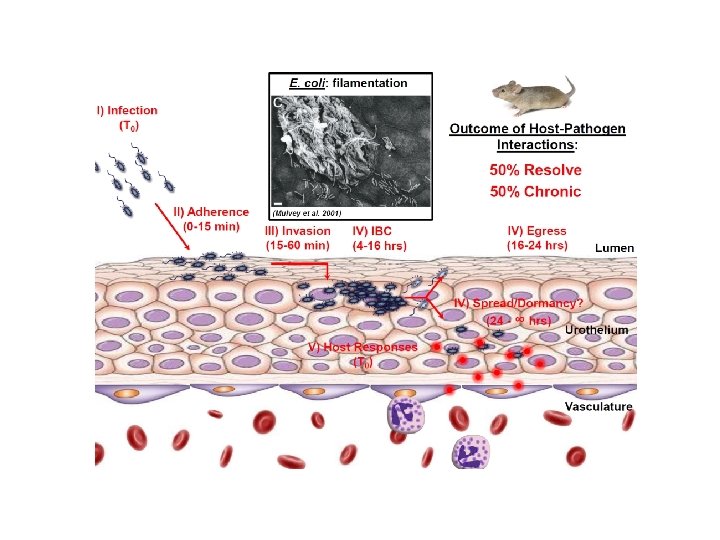
UTI: the natural history No recurrences Infection resolved Initial UTI Reinfection Relapse Unresolved UTI Chronic UTI
Classification of UTI: simple, complicated and recurrent Simple/ uncomplicated • lower UTI in a setting of functionally and structurally normal urinary tract Chronic • Recurrent: ≥ 3 UTIs/12 mo • Unresolved, reinfection and relapse Complicated: with risk factors! • Structural and/or functional abnormality • Immunocompromised • Iatrogenic complication • Pregnancy • Pyelonephritis • Catheter-associated
Recurrent UTI Reinfection (common, 80%) • Different strains of pathogen, re-enter the urinary tract • Usually >= 2 weeks (for same pathogen cultured) • Any organism with an intermittent sterile culture Relapse (less common but difficult) • Same strains of pathogen, persists within the urinary tract • Usually <= 2 weeks • Despite sensitivitybased therapy
Recurrent UTI Cause of reinfection: extraurinary Reservoirs! • Poor personal hygene • Bacterial vaginosis • Multiple sexual partners Relapse: ~ complicated UTI • • Infection stones Chronic bacterial prostatitis Foreign bodies Urethral diverticula and infected periurethral glands Nonrefluxing, normal-appearing, infected ureteral stumps after nephrectomy Infected urachal cysts Infected communicating cysts of the renal calyces Papillary necrosis
Discussion on diagnosis of UTIs: • Typical simple UTI: symptom + sign + routine test of urine • Recurrent or persistent infection: Relapse, Reinfection, persistent Need to check both offense and defence side: • Microscopy and culture of urine (MSU): Before treatment + One week after treatment Clean catch of midstream of fresh urine • Bacteriuria with clinical significance: >105 cfu(colony forming unit) per ml of urine <103 cfu/ml = contaminant, 103~104 cfu/ml = suspected Should combined with symptom, strain of bacteria, etc. • Sensitivity test of antibiotics:
UTI in a nutshell • Typical clinical scenario • Young female • Dysuria, frequency • Urianalysis • WBC +++ • Nitrite +ve • Urine C&S • Escherichia coli growth • Resistant to all beta lactams and beta lactamase inhibitor except carbapenems • Rx • Levofloxacin 500 mg qd po x 3 d
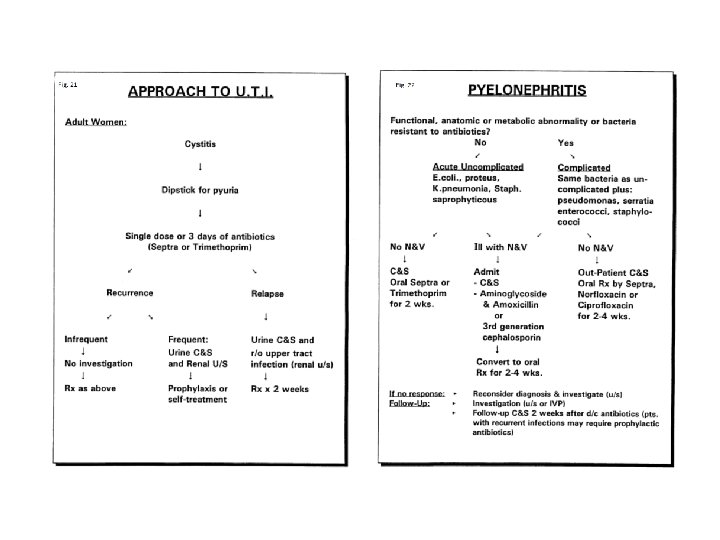
Treatment: antibiotics based therapy Cystitis Pyelonephritis • Oral Abx: empirical • Urine culture/no culture • Intavneous ABx -> oral Abx • Blood culture/urine culture, needs follow up • All patients needs to rule out risk factors (abnormalities? Foreign body? Immune compromise? )
Treatment of UTIs: • Principle: To offense side: sensitive, effective antibiotics To defence side: primary lesion, complication Supportive approach, symptomatic treatment. • Route uncomplicated infection: Single antibiotics, short-term rather than long term full course of treatment. • Severe or complicated infection: Chose antibiotic by sensitivity test, Stop drugs one week after symptom disappear, MSU one week after treatment. • Recurrent uncomplicated infections, especially in Women: low doses antibiotic daily for 6 months or longer single dose of an antibiotic after sexual intercourse short course (1 or 2 d) antibiotics at symptoms appear
What ABx to choose? TMP-SMX Nitrofurantonin Simple, Uncomplicated UTI √ Prevention for recurrence √ Ceftriaxone Ampicillin √ Ciprofloxacin ± Complicated UTI √ √ √ Pyelonephritis √ √ √ ABx of note: Fluoroquinolones Forsfomycin
Indications for investigations • • • pyelonephritis persistence of pyuria/symptoms following adequate therapy severe infection with an increase in Cr recurrent/persistent infections atypical pathogens (urea splitting organisms) hx of structural abnormalities/decreased flow • Investigations: • • • U/A, urine C&S UA: leukocytes ± nitrites ± hematuria C&S: midstream, catheterized, or suprapubic aspirate if hematuria present and persistent need hematuria workup CT scan if indicated
Summary • Adult female are most vulnerable (Pediatric? Senior male? Pregnancy? ) • Short urethra, vagina as reservoirs (in recurrent patients) • Host defense mechanisms: urine flush, urothelial shedding and more • Uropathogenic E. coli are most common pathogen (community vs. iatrogenic? ) • Invasion mechanisms: adhesion, intracellular bacterial community • Factors that increase and decrease risk of UTI (urine flush, bacterial adhesion, reservoir, host immunity)
Summary • Risk factors of UTI (complicated UTI, recurrent UTI) • stasis and obstruction: • residual urine due to impaired urine flow e. g. PUVs, reflux, medication, BPH, urethral stricture, cystocele, neurogenic bladder • foreign body • introduce pathogen or act as nidus of infection e. g. catheter, instrumentation (stone) • decreased resistance to organisms: • DM, malignancy, immunosuppression, spermicide use, estrogen depletion, antimicrobial use • other factors: • trauma, anatomic abnormalities, female, sexual activity, fecal incontinence
Summary • Typical presentation of UTI: • Dysuria, frequency • Bacteriuria • Pyuria • Mainstay of Abx • Quinolones for E. coli, ampicillin for enterococcus • Forsfomycin as a new option
Summary • Prevention of UTI • Maintain good hydration (especially with cranberry juice) • Wipe from front to back to avoid contamination of the urethra with feces from the rectum • Avoid feminine hygiene sprays and scented douches • Empty bladder immediately before and after intercourse
Urinary Tuberculosis
Clinical case • 37 -year-old female patient • Experienced vesical irritability for 5 yrs. Five years ago she had the symptom every 3 to 4 months, which was released by the antibiotics every time. • In recent 2 years, vescial irritability did not disturb her any more, but she felt mild dull pain on her left lumbar area and frequency of urination. She worried about there was something wrong, so came to see the doctor. • what is your consideration and how to make the diagnosis?
• B-Ultrasound image of this patients, left kidney
Urinary Tuberculosis: 1. How does TB occurs in urogenital system? 2. What are the differences between pathological renal TB and clinical renal TB? 3. What are the basic pathological changes of urinary TB, and what are characteristic pathological changes of kidney, ureter, bladder and urethera? 4. What are the pathophysiological results of TB disease in urinary tract? 5. How to diagnose urinary TB, what kind of diagnostic approaches do you like to orderly chose? 6. After the diagnosis, how could you select the different treatments?
Etiology of Urinary TB • Pathogen: Tubercle bacilli, mycobacterium tuberculosis • Immunity of human to TB: lack natural immunity Pathogenesis of Urinary TB: • Secondary to the primary tuberculosis in lung. • Spreads from lung to urinary system by hematogenous route. • Kidney (and possibly the prostate) is the primary sites of genitourinary tract TB, and then involve other sites by descent route.
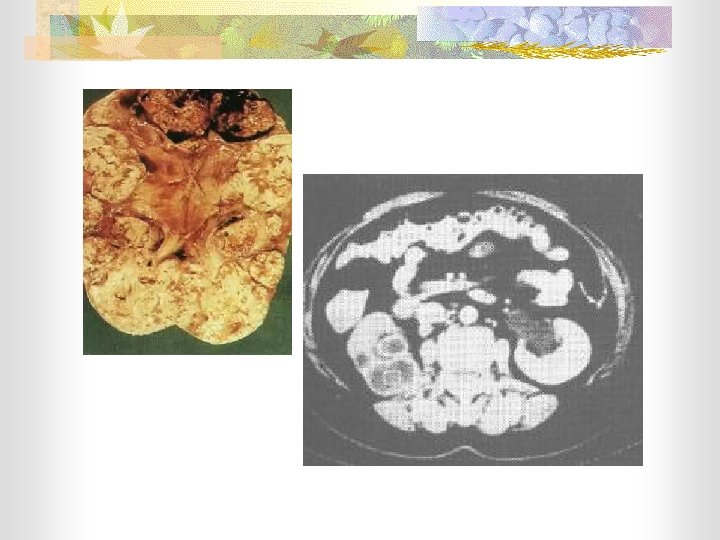
Pathological kidney TB: • Renal cortex of both kidney involved • Granulomatous tubercule formed in cortex • TB may be destroyed by normal tissue defense • Recovery without symptom, found by autopsy Clinical kidney TB: • Renal medullar of unilateral kidney involved • Tubercule formed, and then the destructive and proliferative changes occur. • TB destroyed the parenchyma and enter the collective system, clinical symptom appears.
Basic pathologic change of urinary TB: Caseous abscess Caseous cavity Destructive Changes Caseous Necrosis Scars formation Parenchyma Of kidney Calcification Tubercle Fibrosis Proliferative Changes Mucosa of Urinary tract Caseous ulcer Stenosis Stricture
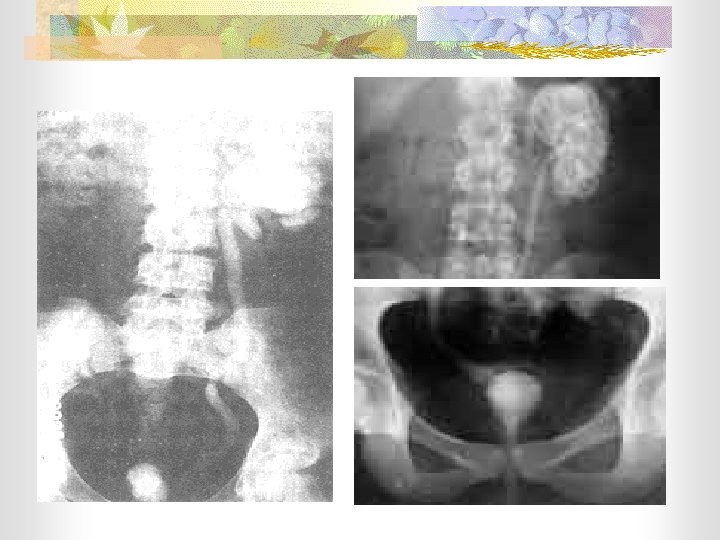
Pathological change of various urinary organs: Contralateral Hydronephrosis Stenosis Ureteral reflux Caseation Abscess, Cavity Tubercular nephritis Calic-pelvis stenosis UPJ stricture Multiple sites involved Hydronephrosis Thicken, Ureterstraight dilationwall Segmental stenosis Autonephrectomy White yellow nodules Deep, ragged ulcer Fibrosis Vesical contracture
Pathological change of various urinary organs: Contralateral Hydronephrosis Caseation Abscess, Cavity Tubercular nephritis Calic-pelvis stenosis UPJ stricture Pathophysiological results of urinary TB: Stenosis Ureteral reflux sites involved Unilateral renal function Multiple Hydronephrosis Thicken, straight wall Total renal function Ureter dilation stenosis Bladder urinating funtion Segmental Autonephrectomy Antireflux function of ureter orifice White yellow nodules Deep, ragged ulcer Fibrosis Vesical contracture
Diagnosis of urinary tuberculosis: • Genitourinary tuberculosis should be considered: 1. Chronic cystitis not responds to adequate therapy 2. ‘Sterile’ pyuria ( finding of pus without bacteria ) 3. Positive sign found at epididymis, prostate, etc. • Four aspects of diagnosis: 1. Etiology Structure 2. Pathology Symptom Pathogen 3. Pathophysiology 4. Symptom Function
Principle of urinary TB treatment: 1. Treatment of Pathogen 2. Protect the function 3. Reconstruct the structure Remove the destroyed organ 4. Symptomatic treatment