Deep Sedation or No Sedation in the ICU
















 +4 Combative +3 Very agitated +2 Agitated +1 Restless 0")


























, 10 October 2002, pp 1196 -1199 Adrenergic-Receptor Polymorphisms and Heart Failure")


: 167 -70")


 and dexmedetomidine (Dex) as local")






: 1427– 1432)")












- Slides: 86
Deep Sedation or No Sedation in the ICU? Where is the Comfort Zone? th Monday June 14 2010 Hong Kong Crit 3 cal Care Medicine and College of Anaesthesiologists Michael Ramsay MD. FRCA Chairman Department of Anesthesia Baylor University Medical Center President Baylor Research Institute.
Speaker Disclosure • I have received research grants and honoraria from: • • Hospira Care. Fusion Ikaria Masimo
• “The body when asleep has no perception; but the soul when awake has cognizance of all things, sees what is visible, hears what is audible, walks, touches, feels pain, ponders. In a word, all the functions of the body and of soul are performed by the soul during sleep. ” Hippocrates, Dreams.
• If the soul is put to sleep by pharmacological agents are our patients at increased risk for adverse events? • In Hippocrates time – 460 – 380 BC, the opium poppy was used for both analgesia and sleep inducing. The notion that the unconscious patient is insensitive to pain was the foundation of anesthesia, analgesia and sedation. • However, at that time, the sleep inducing substances (opium) had analgesic properties as well as sedative effects making this statement true. However, Hippocrates did relate the loss of consciousness in a critically ill patient with a fatal outcome.
ANALGO-SEDATION Good Analgesia FIRST as opposed to SEDATION first may provide the optimal comfort zone for the critically ill patient requiring mechanical ventilation. ANALGO-SEDATION techniques were indeed the first techniques described by Hippocrates and may improve outcomes today!
Goals of Analgesia and Sedation § Optimize safety for acute care patients and their caregivers 1, 2 § Relieve pain and anxiety 1 -3 § Attenuate the harmful adrenergic response 1, 2 § Improve compliance with care 1, 2 § Provide comfort and safety § Facilitate communication with caregivers and family members 1, 2 § Avoid or reduce delirium 1, 2, 4 1 Blanchard AR. Postgrad Med. 2002; 111: 59 -74. Care Med. 2002; 30: 119 -141. 3 Dasta JF, et al. Pharmacotherapy. 2006; 26: 798 -805. 4 Ely EW, et al. JAMA. 2004; 291: 1753 -1762. 2 Jacobi J, et al. Crit
7 Courtesy of M. Ramsay, MD. Sessler CN, et al. Chest. 2008; 133; 552 -565.
Sedation induced Coma in the ICU is Bad Ouimet S et al. Intensive Care Med 2007 8
Petty TL. Suspended Life or Extending Death? Chest 1998; 114: 360 • “But what I see these days are sedated patients, lying without motion, appearing to be dead, except for the monitors that tell me otherwise…. . By being awake and alert…they could interact with family…. feel human…sustain the zest for living which is a requirement for survival”
One Year Outcomes in Survivors of ARDS Herridge et al. NEMJ 2003; 348: 683 -93 • Functional limitations 1 year later • Most patients have muscle wasting and weakness. • Neurocognitive impairments. Hopkins & Brett. Cur Opin Crit Care 2005; 11: 369 • Depression and memory dysfunction increased in ARDS survivors. Chest 2009; 135: 678
Physical limitations after ARDS Herridge et al. NEMJ 2003; 348: 683 -93 • All reported poor function due to: • Loss of muscle bulk, proximal weakness, fatigue • • • Alopecia in most Persistent pain Entrapment neuropathies Immobility from heterotopic ossification Trach site scar problems Contractures/frozen shoulders
Critical Care 2009, 13: 216
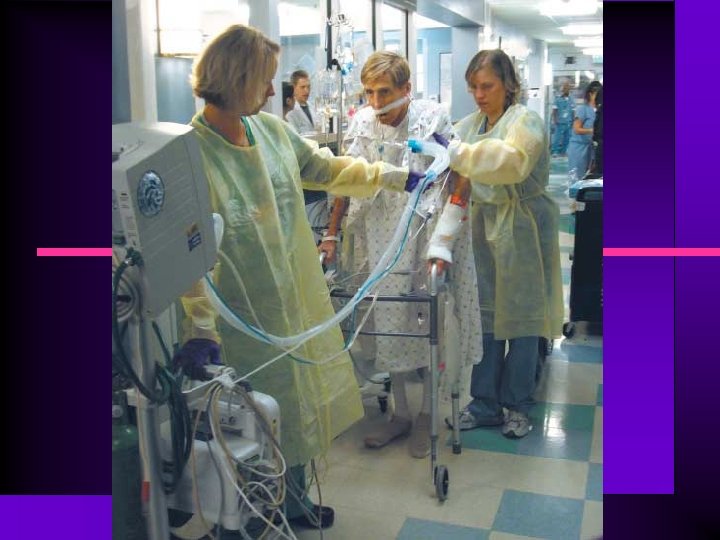
Mobile, Awake and Critically ill Margaret S. Herridge MD MPH CMAJ • March 11, 2008 • 178(6)
Goals of Sedation Scales • • • Avoid oversedation and undersedation Define an optimal endpoint for titration of sedation Provide continuity of care and charting Facilitate cost-effective use of drugs Allow comparison of drugs Enable precise patient management.
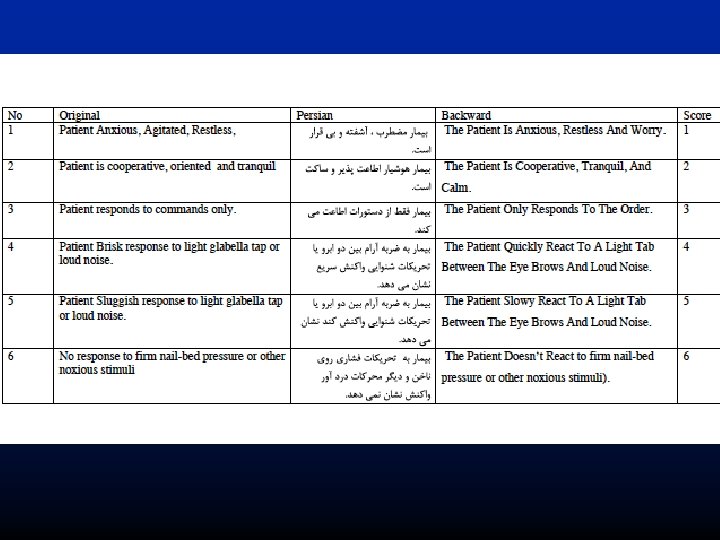
Ramsay Sedation Scale 1 2 3 4 5 6 Anxious and agitated or restless or both Cooperative, oriented, and tranquil Responding to commands only Asleep, brisk response to stimuli* Asleep, sluggish response to stimuli* Asleep, no response to stimuli* * light glabellar tap Ramsay, et al. Brit Med J. 1974; 2(920): 656 -659.
9/10/2020 1: 03 PM
Richmond Agitation-Sedation Scale (RASS) +4 Combative +3 Very agitated +2 Agitated +1 Restless 0 Alert and calm -1 Drowsy -2 Light sedation -3 Moderate sedation -4 Deep sedation -5 Unarousable Sessler, et al. Sem Respir Crit Care Med. 2001; 22: 211 -225. Sessler, et al. Am J Respir Crit Care Med. 2002; 166: 1338 -1344.
Daily Wake-up Study: Clinical Outcomes Wake-up Group Standard of Care Group Mechanical ventilation duration (days) 4. 9 (2. 5 -8. 6) 7. 3 (3. 4 -16. 1) ICU LOS (days) 6. 4 (3. 9 -12. 0) 9. 9 (4. 7 -17. 9) *P=. 004. †P=. 02 Adapted from Kress et al. N Engl J Med. 2000; 342: 1474.
Daily Wake up In ICU • Reduced incidence of: • • PTSD Ventilator-associated pneumonia GI tract bleeding Bacteremia VTE Barotrauma Cholestasis Sinusitis Crit Care Med 2004; 32: 1272 -76
Girard TD, et al. ABC Trial The Lancet 2008; 371 126 -134 • Daily Awakening Sedation combined with Spontaneous Breathing Trial • Adding Respiratory Therapy to Sedation Team • duration of MV; ICU & Hosp LOS; Improved 1 year mortality 21
ICU SEDATION TEAM RN Patient MD
ICU SEDATION TEAM RN Patient MD RPh
ICU SEDATION TEAM RN RT Patient MD RPh
A Randomized Trial of Early Physical & Occupational Therapy in Mechanically Ventilated, Critically Ill Patients WD Schweickert, MC Pohlman, AS Pohlman et al LANCET 2009; 373: 1874 -82
Strategy • Whole-body rehabilitation “Animation” with a highly coordinated, multidisciplinary team implementing: • • Co-operative sedation Spontaneous breathing trials Good Analgesia Physical and occupational therapy • RESULTS IN: Superior functional and cognitive patient outcomes 26
ICU SEDATION TEAM RN PT/OT RPh Patient RT MD
Conclusions: Early exercise training in critically ill intensive care unit survivors enhanced recovery of functional exercise capacity, self-perceived functional status, and muscle force at hospital discharge. Crit Care Med 2009; 37: 2499 – 2505) 29
The Lancet 2010; 375: 475 -80 30
31
32
33
34
The Effect of a Positive Affect • In severe illness a positive affect is related to survival in a dose-response pattern. • Positive affect can be considered a resource for medium-term survival • Scherer & Hermann-Lingen. Gen Hosp Psych 2009; 31: 8 -13
ANALGO-SEDATION Is this the future? 36
37
Clinical Characteristics of Dexmedetomidine § Cooperative sedation 1 § Analgesia 2, 3 § NO RESPIRATORY DEPRESSION § § § Organ protection (ie, neural, renal, cardiac)1 Anxiolysis 2, 3 Controls hyperadrenergic response to stress 1 -3 Reduces shivering 3 Diuretic action 4 Mimics natural sleep 1, 5 1 Aantaa R, et al. Drugs of the Future. 1993; 18: 49 -56. T, et al. Anesthesiology. 2000; 93: 1345 -1349. 3 Wagner BKJ, et al. Clin Pharmacokinet. 1997; 33: 426 -453. 4 Goodman LS, et al. The Pharmacological Basis of Therapeutics. New York, NY: Mc. Graw-Hill; 2004: 232 -235. 5 Huupponen E, et al. Acta Anaesthesiol Scand. 2008; 52: 289 -294. 2 Kamibayashi
a 2 – Agonists and Cognitive Function • There is strong evidence that a 2 – agonists improve prefrontal cortical function (PFC) • PFC shares reciprocal projections with: • Parietal association cortex specialized for visuospatial processing • Medial temporal lobe important to memory abilities • Anterior cingulate cortex involved in organizing complex cognitive function • Caudate nucleus that regulates motor behavior • NE’s beneficial action in the PFC appear to result from stimulation of a 2 (A) – receptors postjunctional to NE terminals Arnstein et el. Arch Gen Psychiatry 1996
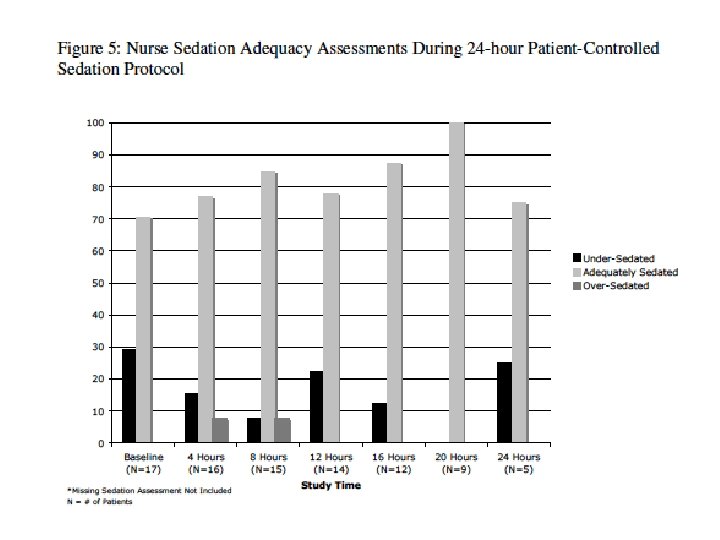
Dexmedetomidine for PCA/S • • • Sedation and analgesia properties Does not cause respiratory depression Rapid distribution (half life 6 mins) and elimination (half life 2 hours) Pharmacokinetics are linear for doses 0. 2 to 0. 7 mcgs/kg/h No active sedating metabolites
Methods • • Loading dose 0. 5 mcgs/kg Basal infusion 0. 2 mcgs/kg/h PCA/S patient trigger 0. 25 mcgs/kg q 20 mins Nurses adjust basal infusion rate up to 0 -7 mcgs/kg/h or down very 2 hours based on patients trigger activity
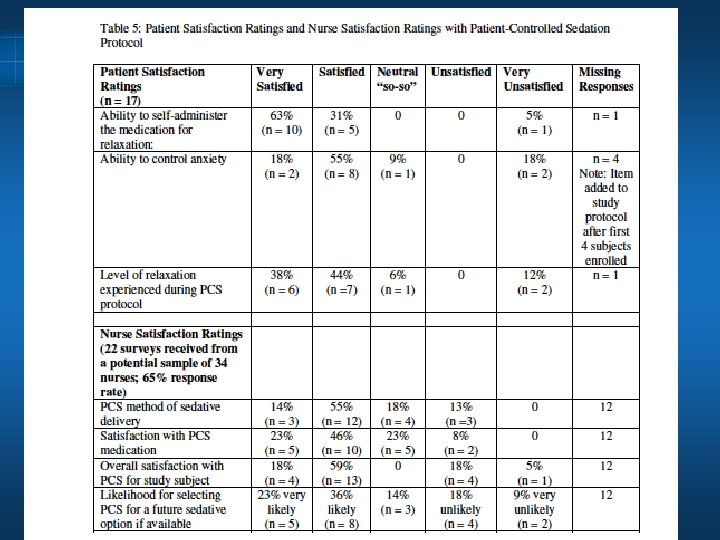
Results • • • 17 patients enrolled 9 females 8 males Mean age was 47. 1 years (+16. 6) Diagnoses included respiratory failure (n =4), pneumonia (n =3), ARDS (n =2), AIDS (n = 2), and n = 1 each for leukemia, COPD, interstitial pneumonitis, lymphangiomyomatosis, myasthenia gravis and pancreatitis.
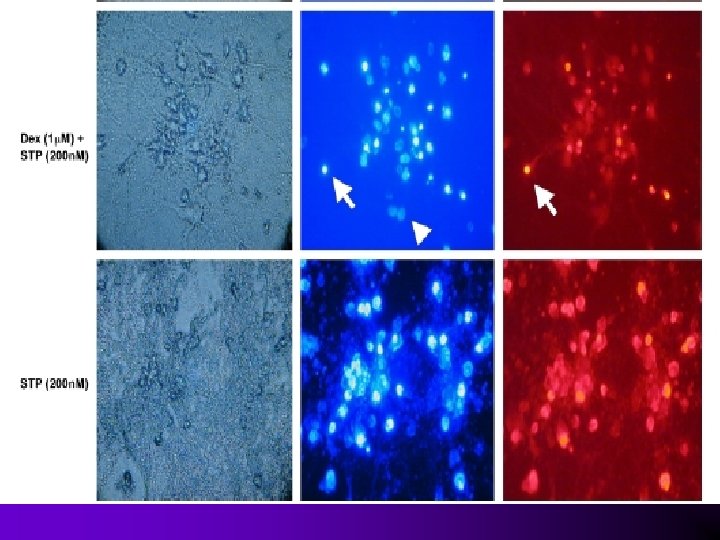
Acta Anaesthesiol Scand 2010; 54: 710– 716
Neuroprotective effects of Dexmedetomidine • Inhibition of ischemia induced NE release may be associated with neuroprotection • Dex prevents delayed neuronal death after focal ischemia • Dex decreased total ischemic volume by 40% compared to placebo Jolkkonen J et al. Euro J Pharm 1999 Hoffman WE et al Anesthesiology 1991 • Dex enhances glutamine disposal by oxydative metabolism in astrocytes Huang R et al. J Cereb Blood Metab 2000
Sedation improves early outcome in severely septic Sprague Dawley rats Hong Qiao, Robert D Sanders, Daqing Ma, Xinmin Wu and Mervyn Maze • Conclusions Sedation with midazolam and dexmedetomidine • Both improve outcome in polymicrobial severely septic rats. • Possible benefits conveyed by one sedative regimen over another may become evident over a more prolonged time course as both IL 6 and apoptosis were reduced by dexmedetomidine but not midazolam. Further studies are required to evaluate this hypothesis. Critical Care 2009, 13: R 136
NEMJ Volume 347(15), 10 October 2002, pp 1196 -1199 Adrenergic-Receptor Polymorphisms and Heart Failure [Editorial] Hajjar, Roger J. ; Mac. Rae, Calum A.
Cardioprotective Action of Alpha 2 Agonists Anesth 2004; 101: 284 -93.
Extubation on Dexmedetomidine • Dexmedetomidine has been continuously infused in mechanically ventilated patients • • • Prior to extubation During extubation And post-extubation • It is not necessary to discontinue prior to extubation • Excellent sedation control before, during and after extubation • Consider converting to dexmedetomidine for weaning protocol
Anesth Analg. 2008 Jul; 107(1): 167 -70
Sedation for Awake Fiberoptic Intubation § Multicenter Phase III trial to evaluate the safety and efficacy of dexmedetomidine for sedation during elective awake fiberoptic intubation (AFOI) § Patients received dex 1. 0 μg/kg and 0. 7 μg/kg/hr (n=55), or placebo (n=50) § The primary end point was the percentage of patients receiving rescue midazolam to maintain appropriate sedation level § Sedation measured according to the Ramsay Sedation Scale (RSS) Bergese SD, et al. Anesthesiol. 2008; 109: A 186.
Sedation for Awake Fiberoptic § Intubation Safety of dex for AFOI assessed through adverse events, lab tests, and vital signs § Hemodynamic stability was determined as a function of the time systolic blood pressure and heart rate were outside the normal range § Incidence of respiratory depression was similar between groups § Hypotension was the most common adverse event in the dex group; hypertension and tachycardia were the most common adverse events in the placebo group § Hemodynamic stability was similar between groups *P<. 001 compared with placebo * * Bergese SD, et al. Anesthesiol. 2008; 109: A 186.
Comparing Agents for Awake Fiberoptic Intubation § Remifentanil (Rem) and dexmedetomidine (Dex) as local anesthetic adjuncts for awake fiberoptic intubation (AFOI) § 30 patients with difficult airways were randomly assigned to receive either Rem (0. 75 μg/kg; 0. 075 μg/kg/min) or Dex (0. 4 μg/kg; 0. 7 μg/kg/hr) for AFOI § Data included heart rate, blood pressure, respiratory rate, bispectral index (BIS) level, Sp. O 2, and Ramsay Sedation Scale (RSS) score Results § Significantly more patients in the Rem group were intubated on the first attempt (P=. 02) § Dex patients had significantly greater oxygen saturation (P=. 03) § Patients receiving Dex had a significantly lower RSS score (P=. 008), but took longer to reach an RSS level of 3 (P<. 05) § The Dex group had a significantly lower mean BIS (P=. 018) Hagberg CA, et al. Anesthesiol. 2008; 109: A 14.
63
Sedation During MAC § Multicenter Phase III trial to evaluate the safety and efficacy of dexmedetomidine for sedation of nonintubated patients under MAC § 326 patients undergoing various elective procedures and/or surgeries under MAC received dex 1. 0 μg/kg (n=129), dex 0. 5 μg/kg (n=134), or placebo (n=63) § Sedation level measured according to Observer’s Assessment of Alertness/Sedation Scale (OAA/S) § Satisfaction was measured with the Iowa Satisfaction With Anesthesia Scale (ISAS) and anxiety was assessed before, during, and after drug administration Candiotti K, et al. Anesthesiol. 2008; 109: A 1202.
Sedation During MAC § Dex maintained sedation level without additional midazolam significantly better than placebo § Significantly fewer patients on dex required postoperative analgesic treatment (P=. 025) § ISAS scores were significantly higher in patients from both dex groups (P<. 001) § Anxiety scores were significantly lower in patients in the dex 1. 0 μg/kg group (P=. 007) § Respiratory depression was significantly greater in the placebo group § The data indicate that dex is safe and effective in patients undergoing various procedures during MAC Candiotti K, et al. Anesthesiol. 2008; 109: A 1202.
Patient having eye surgery using dexmedetomidine 67
Immediate Extubation Following Cardiac Surgery § Horswell et al conducted a study of immediate extubation after off-pump coronary artery bypass graft (OPCAB) in 514 patients § Following surgery, each patient received 2 or more of the following: epidural anesthesia, IV morphine on demand, IV ketorolac on schedule, and/or continuous IV dexmedetomidine § All patients were successfully extubated immediately after dressing application § The investigators concluded that immediate extubation of OPCAB patients is feasible and probably safe Horswell JL, et al. J Cardiothorac Vasc Anesth. 2005; 19: 282 -287.
Pharmacotherapy 2009; 29(12): 1427– 1432)
Jeffrey F. Barletta, et al
ICU SEDATION AFTER CABG • DEXMEDETOMIDINE vs PROPOFOL • • No VTACH Less Morphine Less Beta-Blocker Less antiemetics Less NSAIDS Less epinephrine Less high dose diuretic 5% p<0. 001 p=0. 014 p=0. 015 p<0. 001 p<0. 030 p<0. 001 • Herr DL, Sum-Ping ST. England M J. Cardiothorac
DEXMEDETOMIDINE FOR PEDIATRIC SEDATION TOBIAS JD
Laser Resection of Tracheal Stenosis • • • TIVA with dexmedetomidine Loading dose 1 mcg/kg then 10 mcg/kg/h Weaned to 5 mcg/kg/h Room air O 2 sats > 92% Heart rate stable at 68 bpm BP 180 mm. Hg down to 110 systolic mm. Hg
Compromised Airway Severe subglottic stenosis
10µg/kg/h 5µ/kg/h 10µg/kg/h
CHIN LIFT
Pharmacoeconomic Analysis Reduced Hospitalization and Mortality Mean Length of Stay Mean Days in ICU/CCU Mortality Rate P<. 0001 P=. 0142 M+P, n = 9996 D+M+P, n = 356 1 Dasta JF, et al. Pharmacotherapy. 2006; 26: 798 -805.
Pharmacoeconomic Analysis Reduced Mean Total Treatment Charges P<. 05 § § § 12 -month retrospective administrative claims database analysis 1 Comparison of patients receiving either midazolam plus propofol (M+P) or dexmedetomidine plus M+P (D+M+P)1 The D+M+P cohort showed significant reductions in per patient total charges 1 M+P, n = 9996 D+M+P, n = 356 1 Dasta JF, et al. Pharmacotherapy. 2006; 26: 798 -805.
Summary α 2 -Adrenoceptor agonists have an immensely diverse utility in peri-operative and critical care medicine. Their application as premedicants, analgesics and hypnotics/sedatives is becoming increasingly popular with delivery to a wide spectrum of patients. The ability of these agents to provide renal, cardiac and neurocognitive protection is only just being realized and requires further study.
Summary • Choice of sedation and patient management affects duration of mechanical ventilation in the ICU • Quality of patient outcome from sedation and anesthesia may be affected by choice of drug, depth of sedation and overall patient management
Deep Sedation or No Sedation? • • • Dexmedetomidine hits the COMFORT ZONE Analgesia with cognitive sedation Protects the brain and the mind Allows extubation, mobilization and conversation ANALGOSEDATION with dexmedetomidine