Sedation RASS Sedation Holds and Delirium Critical Care




 4 Combative Overtly combative or violent; immediate danger to staff 3")


















, liver")



 you can ◦ Sleep deprivation, drugs etc.")

- Slides: 30
Sedation, RASS, Sedation Holds and Delirium Critical Care Fellow Teaching James Bonnington– Consultant in Critical Care 26 th September 2016
Plan � What is “sedate”? � What is RASS and why does it matter? � Why bother with a sedation hold if we’re not going to extubate? � Which drugs should I be prescribing? � What about level 2 patients? � How do I spot delirium? � Why does delirium matter? � What do I do about delirium?
What is “sedate”? � From the Latin “sedere” meaning to sit � “Sedare” – to settle � Tranquil, calm, not sore or painful � Note – this is not the same as “render unconscious” � So our patients should be tolerant of our care but not under a general anaesthetic
What is RASS and why does it matter? � Richmond � Used Agitation & Sedation Score to quantify in an objective manner the agitation or sedation level of a patient
Score Classification (RASS) 4 Combative Overtly combative or violent; immediate danger to staff 3 Very agitated Pulls on or removes tube(s) or catheter(s) or has aggressive behavior toward staff 2 Agitated Frequent nonpurposeful movement or patient–ventilator dyssynchrony 1 Restless Anxious or apprehensive but movements not aggressive or vigorous 0 Alert and calm -1 Drowsy Not fully alert, but has sustained (more than 10 seconds) awakening, with eye contact, to voice -2 Light sedation Briefly (less than 10 seconds) awakens with eye contact to voice -3 Moderate sedation Any movement (but no eye contact) to voice -4 Deep sedation No response to voice, but any movement to physical stimulation -5 Unarousable No response to voice or physical stimulation
Why does this matter? � Think � How about the definition of “sedate” many of our patients are sedated and how many are unarousable?
Negative effects of sedation? � Drug side effects � Accumulation of drugs � Haemodynamic instability � Prolonged ICU stay � More likely to develop complication of ICU stay (e. g. chest infection) � Patients left disconnected from reality
Sedation hold/holiday � Daily discontinuation of all sedative drugs until such time as the patient is… � Able to be safely extubated � Alert and responding to voice � Unmanageable and becoming a danger to themselves or others
Why bother? � Less likely to accumulate � Less haemodynamic instability � Keep patient orientated in time and place � Potentially easier to wean from the ventilator � Potentially shorter stay on the ICU � Potentially fewer complications of ICU care � (“Potentially” as evidence although in favour has been questioned recently) � (Certainly no harm demonstrated with sedation holds)
What to do during daily r/v � “Please do a sedation hold” � “Extubate if you are happy” � “Let me know when they wake up a bit” � “Re-sedate when they are waking” � “When you re-sedate please aim for a RASS of -2 / -3”
When should we not do sedation holds? � Neuromuscular blockade � TBI with raised ICP � >60% oxygen, PEEP >10, APRV/HFOV � C-spine injury proven or suspected � Locally acting chemotherapy drugs requiring immobilisation � CVS instability � Palliative care � Grade 3/4 laryngoscopy � No airway trained personnel immeadiately available
Ideal sedatives � Quick onset and offset � Easy to titrate � CVS stability � ICP stability � Doesn’t rely on renal or hepatic function to be eliminated � Non-toxic � Not addictive � Cheap � Easy to prepare
Which drugs? � NUH ◦ ◦ Propofol Midazolam Alfentanil Morphine
Which drugs? � Propofol � Ketamine � Alfentanil � Thiopentone � Midazolam � Morphine � Clonidine � Remifentanil � Dexmedetomidine � Fentanyl � Isoflurane
When prescribing think about… � What are you trying to achieve? � Sedation or pain control or both? � Sedation – propofol, midazolam, clonidine � Analgesia – morphine, alfentanil, enteral route, epidural, nerve block(s), paracetamol
Propofol – pros and cons � Advantages ◦ ◦ Quick onset and offset No preparation required Easily titratable Reduces ICP � Disadvantages Negative inotrope and vasodilator Abolishes protective airway reflexes Produces apnoea Liver metabolised (but actually safe in those with liver disease) ◦ Calories – 1 ml of 1% = 1 cal ◦ Propofol infusion syndrome ◦ Cost ◦ ◦
Propofol infusion syndrome � Cardiac failure � Rhabdomyolysis � Metabolic acidosis � AKI � Hyperkalaemia � Hypertriglyceridaemia � Hepatomegaly � Often fatal �> 4 mg/kg/h for more than 24 hours � Does occur at lower doses too
Midazolam – pros and cons � Advantages ◦ Quick onset ◦ Reduces ICP ◦ Cheap � Disadvantages Vasodilator Long offset (after infusion) Very unpredictable dose requirements Benzo’s worsen delirium Can cause apnoea Liver metabolised but metabolites are still active and need renal excretion ◦ Physical and psychological addition ◦ ◦ ◦
Alfentanil – pros and cons � Advantages ◦ Quick onset ◦ Easy to titrate ◦ Strong analgesic effect � Disadvantages Negative chronotrope Potent respiratory depressant Not a very good sedative Reduced GI motility Nausea and vomiting Accumulates Liver metabolised but active metabolites are renally excreted ◦ Cost ◦ ◦ ◦ ◦
Morphine – pros and cons � Advantages ◦ Excellent analgesic ◦ Fairly CVS stable ◦ Cheap � Disadvantages ◦ ◦ ◦ Histamine release Accumulates Liver metabolites – active – renal excretion Addictive – physically and psychologically Respiratory depression
So what should I prescribe? � First line ◦ Propofol and morphine � Renal/hepatic dysfunction? ◦ Alfentanil rather than morphine � Alcohol dependence? � Hepatic dysfunction? ◦ Clonidine ◦ Caution with doses of opioids and midazolam
Sedation in level 2 patients � Are they delirious? � Yes – follow the delirium guideline, extra nursing support � No – reassurance and follow the night sedation guideline if they want help sleeping
What is delirium? � Disturbance � Acute of consciousness onset � Fluctuating course � Inattention � Change in cognition � Perceptual disturbance � Results in loss of a patient’s ability to receive, process, store, and recall information
What are the risk factors? � Medical condition ◦ Brain injury (any cause), liver failure, sepsis etc. � Substance abuse or withdrawal � Prescribed drugs ◦ Alcohol, opiates, benzo’s ◦ Opiates, benzo’s, neuroleptics � Toxins � Lack of sleep
How do I spot delirium? � Hyperactive ◦ Easy to pick up ◦ Agitated, restless, attempting to remove tubes and lines ◦ Purely hyperactive is uncommon - <5% � Hypoactive ◦ Easy to miss ◦ Withdrawn, flat affect, apathic, lethargic and decreased responsiveness � Mixed � CAM-ICU
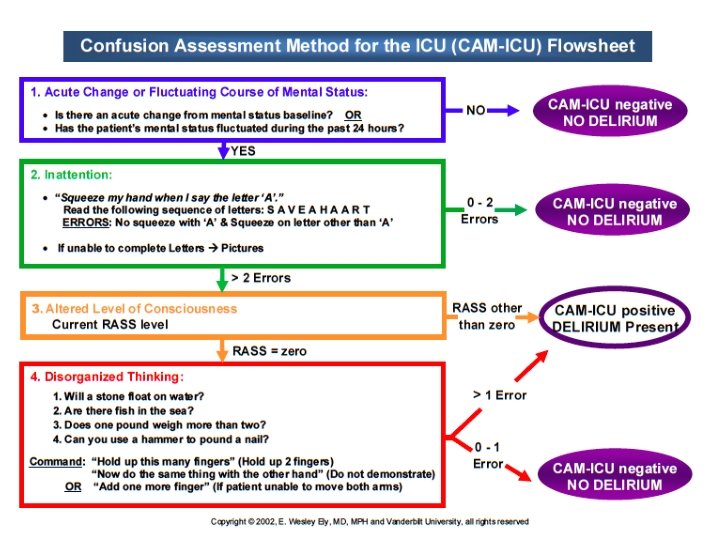
CAM-ICU � Confusion Assessment Method for the ICU � Step one – check level of consciousness (RASS ≥ -3) � Step two – check content of consciousness ◦ Acute or fluctuating changes AND ◦ Inattention AND ◦ Altered level of consciousness OR disorganized thinking
Why does delirium matter? �↑ �↑ mortality length of stay time on vent costs re-intubation long-term cognitive impairment discharge to long-term care
Treatment of delirium � Remove any cause(s) you can ◦ Sleep deprivation, drugs etc. � Hyperactive ◦ Haloperidol, quetiapine ◦ Clonidine, low dose propofol, benzo’s (last choice) � Hypoactive ◦ Risperidone, low dose haloperidol � TBI associated ◦ Quetiapine
Summary � Sedation holds � Sedatives � Delirium