International Society of Nephrology Renal Pathology Society 2003


 Classification of Lupus Nephritis (LN) I")
.")



















 2010; 49: 128 -40.")
 FU,LW. et al: British Journal of Rheumatology 1998; 37: 217– 221")
 FU,LW. et al: British Journal of Rheumatology 1998; 37: 217– 221")

 , 治疗 6个月 N 用量 浓度 CR 总有效率 FK 506")











 和CD 27 high浆细胞 ÷ 在这些因子中可溶性的IL-2")




: 189– 195")

SLEDAI评价疾病活动 ,对照组为非狼疮血 透患者,观察 60个月")





- Slides: 109
International Society of Nephrology/ Renal Pathology Society (2003) Classification of Lupus Nephritis (LN) I Minimal mesangial LN II Mesangial proliferative LN III Focal LN* (<50% of glomeruli) A A/C C IV Diffuse LN* (50% of glomeruli) Diffuse segmental (IV-S) or global (IV-G) LN A A/C C V Membranous LN, III+V IV+V VI Advanced sclerosing LN (90% globally sclerosed glomeruli without residual activity)
Lupus nephritis class II. There is mild global mesangial hypercellularity (periodic acid–Schiff, × 400). Lupus nephritis class II. Electron micrograph showing abundant mesangial electrondense deposits (× 12, 000).
Lupus nephritis class III. There is focal segmental endocapillary proliferation (Jones methenamine silver, × 100). The glomerular endocapillary proliferation is discretely segmental with necrotizing features and an early cel- lular crescent (Jones methenamine silver, × 400).
Lupus nephritis class IV. There is global endocapillary pro- liferation with infiltrating neutrophils and segmental wire loop deposits (hematoxylin and eosin, × 320). Lupus nephritis class IV. Electron micrograph show- ing a large subendothelial electron-dense deposit as well as a few small subepithelial deposits (arrow) (× 1200).
Lupus nephritis class V. Silver stain highlights glomerular basement membrane spikes projecting outward from the glomerular base- ment membranes toward the urinary space (Jones methenamine silver, × 800). Lupus nephritis class V. Electron micrograph showing numerous subepithelial electron-dense deposits as well as mesangial deposits (× 5000).
我们能个体化的治疗严重增殖性狼疮性肾炎 吗? 按照以下因素而改变治疗 药物激活或失 活代谢途径的 基因改变 遗传性或获得性 药物摄取和转运 途径的改变 遗传性或获得性 药物作用靶点的 改变 依据生物标志改变治疗 预测疾病的活动 和复燃 预测疾病的严 重性/进展 预测对治疗 的反应 Approaches to individualize therapies of kidney diseases. (Top) Pharmacogenetic, pharmacogenomic, and pharacodynamic approaches. (Bottom) Biomarker approaches. It is likely that both approaches will be used in combination to generate personalized medicine panels to individualize therapies.
诱导治疗:CTX ÷ NIH方案 ÷ Euro-Lupus方案 未发生LN复发比例比较 未发生严重感染比例比较 HD:NIH方案;LD:Euro. Lupus方案 Ann Intern Med 1996; 125: 549 -57; Arthritis Rheum 2002; 46: 2121 -31.
口服及静脉注射CTX治疗LN疗效 Chiu Mok et al : The American Journal of Medicine, Vol 119, No 4, April 2006
CTX治疗完全缓解的预后因素 Chiu Mok et al : The American Journal of Medicine, Vol 119, No 4, April 2006
212例狼疮性肾炎患者的无事件存活 Chiu Mok et al : The American Journal of Medicine, Vol 119, No 4, April 2006
诱导治疗:MMF与CTX 非劣性研究 ÷ 2005, Ginzler等 Ginzler et al: N Engl J Med 2005; 353: 2219 -28.
在增殖性狼疮性肾炎的治疗中MMF 与CTX的比较 a meta-analysis and meta-regression Mak A et al: Rheumatology 2009; 48: 944– 952 37
在增殖性狼疮性肾炎的治疗中MMF 与CTX的比较 a meta-analysis and meta-regression Mak A et al: Rheumatology 2009; 48: 944– 952
在增殖性狼疮性肾炎的治疗中MMF 与CTX的比较 a meta-analysis and meta-regression Mak A et al: Rheumatology 2009; 48: 944– 952
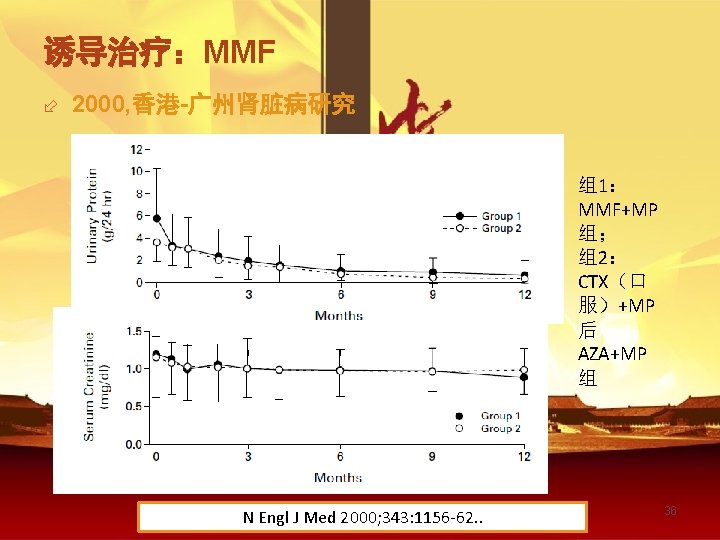
诱导治疗:MMF ÷ ALMS研究:人种对MMF应用的影响 Rheumatology (Oxford) 2010; 49: 128 -40.
新山地明治疗儿童增殖性狼疮性肾炎( 诱导缓解) FU,LW. et al: British Journal of Rheumatology 1998; 37: 217– 221
新山地明治疗儿童增殖性狼疮性肾炎( 诱导缓解) FU,LW. et al: British Journal of Rheumatology 1998; 37: 217– 221
Cs. A治疗增殖性LN Zavada J et al: Lupus 2010 19: 1281 -9
FK 506 与CTX+AZA Chen等多中心随机对照研究,81例增殖型LN(III-V型) , 治疗 6个月 N 用量 浓度 CR 总有效率 FK 506 42 0. 05 mg/kg/d 5 -10 ng/ml 52. 4% 90. 5% CTX 39 38. 5% 82. 1% Chen Wei al: AJKD 2011, 57: 235 -44 Szeto等FK 506 与CTX+AZA对V型LN, 用 6个月, 随访 12 月. FK 506组LN缓解迅速,无明显副作用 N 用量 浓度 CR PR 18 0. 1 o. 2 mg/kg/d 3 -8 ng/ml 38. 9% 44. 4% CTX Szeto C C 19 36. 8% et al: Rheumatology(Oxford) 2008, 47: 1678 -81 57. 9% FK 506
狼疮性肾炎生物治疗的机制 Klippel, J. H. et al. Primer on the Rheumatic Diseases. 13 th ed. pp. 335
狼疮性肾炎生物治疗的机制 B Cell Depletion Klippel, J. H. et al. Primer on the Rheumatic Diseases. 13 th ed. pp. 335
狼疮性肾炎生物治疗的机制 抑制B细胞存活 Klippel, J. H. et al. Primer on the Rheumatic Diseases. 13 th ed. pp. 335
狼疮性肾炎生物治疗的机制 细胞因子抑制剂 Klippel, J. H. et al. Primer on the Rheumatic Diseases. 13 th ed. pp. 335
狼疮性肾炎生物治疗的机制 其他靶点治疗 Klippel, J. H. et al. Primer on the Rheumatic Diseases. 13 th ed. pp. 335
SLE免疫抑制/免疫调节治疗的生物制剂 ÷ B-cell targeted therapies ÷ B-cell depletion:Anti-CD 20 m. Ab; Anti-CD 22 m. Ab ÷ B-cell survival factors. B细胞成活因子: ÷ Anti-BLy. S m. Ab抗B淋巴细胞刺激蛋白单克隆抗体 ÷ TACI Ig(阿噻西普) 是可溶性的结合BLy. S 和 APRIL的受体。 ÷ Toleragen:P-394 ÷ Co-stimulatory blockade ÷ CTLA 4 -Ig ÷ Anti-CD 40 ligand m. Ab ÷ Anti-cytokine therapies: Anti-IL-10 m. Ab; Anti-TNF-α ÷ Anti-complement therapy: Anti-C 5 b-9 m. Ab ÷ Non-specific immunotherapy:iv IG , BMT
Response to rituximab according to LN type Ramos-Casals M et al: Clinic Rev Allerg Immunol (2011) 40: 159– 169
EULAR/ERA-EDTA recommendations for the management of adult and pediatric lupus nephritis 血清C 3 一般较C 4 更为敏感(72% to 85% vs 28% to 74%),对狼疮肾炎活动的预测都具有中等程度 的特异性。 ÷ 抗-ds. DNA 的诊断精确性也只是中等程度的,阳 性及阴形的可能性比分别为 1. 5– 4. 8 and 0. 3– 0. 8。 ÷ Bertsias GK et al: Ann Rheum Dis 2012; 71: 1771– 1782
狼疮性肾炎活动的生物标志 ÷ 新的生物标志:IFN-alfa 或其基因的表达, 淋巴 细胞激活的标志如可溶性IL-2 R、内皮细胞激活的 标志如VCAM-1以及血清凝血调节因子(Serum Thrombomodulin) 和CD 27 high浆细胞 ÷ 在这些因子中可溶性的IL-2 R以及血清凝血调节因 子与狼疮性肾炎的活动特异性相关 Illei GG, Tackey E, Lapteva L, et al: Biomarkers in systemic lupus erythematosus: II. Markers of disease activity. Arthritis Rheum 50: 2048 -2065, 2004
HD PD技术患者存活率 血透 5年为 86% ; 10年为 86% ;腹透 5年为 70% 10年为 23% Seok-Hui Kang: The Korean Journal of Internal Medicine Vol. 26, No. 1, March 2011
透析开始后狼疮活动逐年下降 Cheigh JS. Am J Kidney Dis 1990 16 (3): 189– 195
Disease activity in systemic lupus erythematosus patients with end-stage renal disease: systematic review of the literature MEDLINE (1966 to 2011), SCielo, 和 LILACS 数据库, 以 : “chronic renal failure”, “systemic lupus erythematosus”, “end-stage renal disease”, “lupus activity”, “disease activity”, “lupus flare”, “hemodialysis”, and “renal replacement therapy”关 键词进行检索 • 24篇文章符合要求,15篇文章报告进入ESRD后临床及血 清学的活动指标减轻,9篇报告与前无差别。至少 50%的 病例存在狼疮活动。 • Mattos P & Santiago MB:Clin Rheumatol (2012) 31: 897– 905
Survival of lupus patients on dialysis 20个透析中心,2003年 5月-2004年 2月进入研究, 以进 入研究时(nr)SLEDAI评价疾病活动 ,对照组为非狼疮血 透患者,观察 60个月 • nr. SLEDAI>8 (HR) 6. 368; 95% CI 1. 798, 22. 548; P = 0. 004], 和尿素下降率 (HR. 953; 95% CI 0. 917, 0. 990; P = 0. 014) 与狼疮病人的死亡率相关。 • 5年存活率对照组与SLE nr. SLEDAI≤ 8 (n = 51)类似, (83% and 73%) ,显著好于SLE nr. SLEDAI>8 (n = 6, 17%), P<0. 001. • 结论:nr. SLEDAI高的透析患者有显著高的5年透析死亡率 • Ribeiro FM et al: Rheumatology 2013; 52: 494 -500
Survival of lupus patients on dialysis 狼疮与非狼疮的累积存活率 活动与非活动性狼疮累积存活率 Ribeiro FM et al: Rheumatology 2013; 52: 494 -500
狼疮透析患者的累积存活 Ribeiro FM et al: Rheumatology 2013; 52: 494 -500 Kaplan-Meyer cumulative survival comparing SLE with nr. SLEDAI > 8 (refined Kaplan-Meyer cumulative survival dashed line) and nr. SLEDAI 4 -8 (coarse comparing SLE 60 months (P = 0. 096). dashed line) with the control group (continuous line) over 60 months.
不同替代治疗方式与存活率 Seok-Hui Kang. The Korean Journal of Internal Medicine Vol. 26, No. 1, March 2011
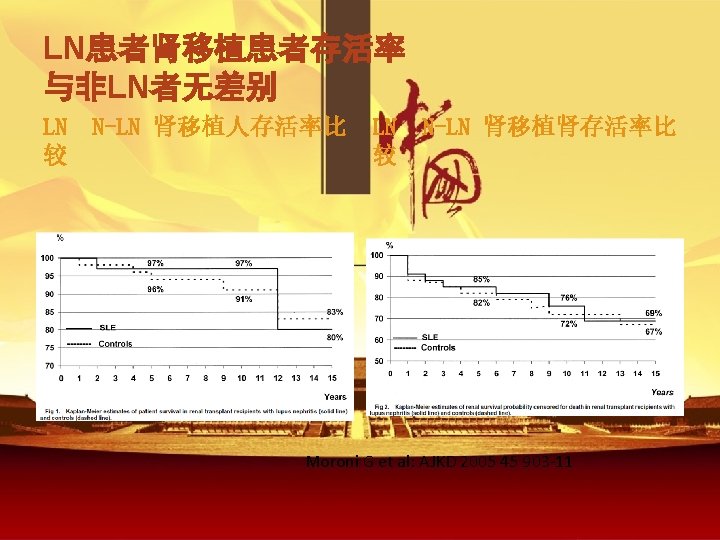
狼疮患者的肾移植 ÷ 从1959年开始成功的进行了尸体肾移植 ÷ 1975报告了56例SLE患者的移植,其 2年及3年的成活与 非狼疮患者类似 Renal transplantation in congenital and metabolic diseases: a report from ASC/NIH Renal Transplant Registry. JAMA 1975; 232: 148 -153.
THE OPINION OF LUPUS NEPHRITIS • 狼疮性肾炎,其临床过程、进展及适当的治疗是 一个“被过度权威观点所左右而可利用的科学信息 有限的”课题。 Edmund Lewis: Nature history and treatment of lupus nephritis in LUPUS NEPHRITIS first ed 1999 Oxford • 十余年的时间已经过去了,权威观点的作用丝毫 没有减轻,而“可利用的科学信息”确实已经在增 Glassock RJ: The treatment of severe proliferative lupus 加 nephritis, in LUPUS NEPHRITIS second ed 2011 Oxford • 狼疮性肾炎的不可预测性、多样性、发病机制的 不均一性、RCT固有的局限性