Acid Base Physiology and Arterial Blood Gas Interpretation

Acid Base Physiology and Arterial Blood Gas Interpretation By: Dr. behzad barekatain, MD Assistant professor of pediatrics neonatalogist

Selected Acid-Base Web Sites http: //www. acid-base. com/ http: //www. qldanaesthesia. com/Acid. Base. Book/ http: //www. virtual-anaesthesia-textbook. com /vat/acidbase. html#acidbase http: //ajrccm. atsjournals. org/cgi/content/full/162/6/2246 http: //www. osa. suite. dk/Osa. Textbook. htm http: //www. postgradmed. com/issues/2000/03_00/fall. htm http: //medicine. ucsf. edu/housestaff/handbook/Hosp. H 2002_C 5. htm
 Severe respiratory or metabolic disorders (2) Clinical")
Indications for ABG • • • (1) Severe respiratory or metabolic disorders (2) Clinical features of hypoxia or hypercarbia (3) Shock (4) Sepsis (5) Decreased cardiac output (6) Renal failure (7) Ideally any baby on oxygen therapy (8) Inborn errors of metabolism (9) ventilated infant ………………….
 is a test that measures the oxygen tension")
INTRODUCTION An arterial blood gas (ABG) is a test that measures the oxygen tension (Pa. O 2), carbon dioxide tension (Pa. CO 2), acidity (p. H), oxyhemoglobin saturation (Sa. O 2), and bicarbonate (HCO 3) concentration in arterial blood. Some blood gas analyzers also measure the methemoglobin, carboxyhemoglobin, and hemoglobin levels. Such information is vital when caring for patients with critical illness or respiratory disease. As a result, the ABG is one of the most common tests performed on patients in intensive care units (ICUs).

The sites, techniques, and complications of arterial sampling are reviewed here, as well as the transport and analysis of the arterial blood. Normal ABG values are provided and a common clinical situation in which the ABG results may be misleading is also described. Interpretation of abnormal ABG values and venous blood gases are also discussed

ARTERIAL SAMPLING Arterial blood is required for an ABG. It can be obtained by percutaneous needle puncture or from an indwelling arterial catheter. • A) Needle puncture — Percutaneous needle puncture refers to the withdrawal of arterial blood via a needle stick. It needs to be repeated every time an ABG is performed, since an indwelling catheter is not inserted.

Site selection The initial step in percutaneous needle puncture is locating a palpable artery. Common sites include the radial, femoral, brachial, dorsalis pedis, or axillary artery. There is no evidence that any site is superior to the others. However, the radial artery is used most often because it is accessible, easily positioned, and more comfortable for the patient than the alternative sites.

1. The radial artery is best palpated between the distal radius and the tendon of the flexor carpi radialis when the wrist is extended. To get the wrist into this position, the arm should be positioned on an arm-board with the palm facing upward and a large roll of gauze should be placed between the wrist and the arm-board in a position that extends the wrist. Taping the forearm and palm to the arm-board helps maintain the position.

2. The brachial artery is best palpated medial to the biceps tendon in the antecubital fossa, when the arm is extended and the palm is facing up. The needle should be inserted just above the elbow crease.

3. The femoral artery is best palpated just below the midpoint of the inguinal ligament, when the lower extremity is extended. The needle should be inserted at a 90 degree angle just below the inguinal ligament.

4. The dorsalis pedis artery is best palpated lateral to the extensor hallucis longus tendon. It receives collateral flow from the lateral plantar artery through an arch similar to that in the hand.

5. The axillary artery is best palpated in the axilla, when the arm is abducted and externally rotated. There is good collateral flow to the arm through the thyrocervical trunk and subscapular artery; thus, the risk of ischemic complications to the arm is low. The needle should be inserted as high into the axilla as possible

Collateral circulation We believe that patients undergoing radial or dorsalis pedis artery puncture should have the collateral flow to those vessels evaluated prior to puncture, even though studies have found variable accuracy associated with such evaluations. Our belief is based upon the notion that the evaluation can be performed quickly at the bedside at no cost and with little risk for harm, but has substantial potential for benefit (ie, to identify patients who have impaired collateral circulation and, therefore, may be at increased risk of an ischemic complication).

The Allen test or modified Allen test can be performed in patients undergoing radial artery puncture. These are bedside tests that demonstrate collateral flow through the superficial palmar arch. To perform the modified Allen test, the patient's hand is initially held high with the fist clenched and both the radial and ulnar arteries compressed. This allows the blood to drain from the hand. The hand is then lowered, the fist is opened, and pressure is released from the ulnar artery. Color should return to the hand within six seconds, indicating that the ulnar artery is patent and the superficial palmar arch is intact. The test is considered abnormal if ten seconds or more elapses before color returns to the hand.
 is performed")
• The Allen test (from which the modified Allen test evolved) is performed identically, except these steps are executed twice: once with release of pressure from the ulnar artery and once with release of pressure from the radial artery.

For patients undergoing dorsalis pedis artery puncture, the dorsalis pedis artery can be occluded, followed by compression of the nailbed of the great toe and assessment of the rapidity with which color returns to the nailbed after pressure is released from the great toe

Technique Once a palpable artery has been located, blood is withdrawn using the following steps. 1. The planned puncture site should be sterilely prepped. 2. Local analgesia prior to arterial puncture should be considered, since it appears to prevent pain without adversely impacting the success of the procedure. This was illustrated by a trial that randomly assigned 101 patients undergoing arterial puncture to receive 2 percent lidocaine, normal saline, or no agent prior to the procedure. The lidocaine decreased pain without increasing the difficulty of the procedure (ie, the number of attempts), compared to the other groups.

3. The seal of a heparinized syringe should be broken by pulling its plunger. The plunger can then be pushed back into the syringe, leaving a small empty volume (eg, less than 1 m. L) in the syringe. A small needle (eg, 22 to 25 gauge) should then be attached to the syringe. Arterial blood gas kits are available, which contain a heparinized plastic syringe with the plunger already pulled back to allow for the collection of 2 m. L of blood without the need to break the seal. 4. Using one hand to gently palpate the artery and the other to manipulate the syringe and needle, the artery should be punctured with the needle at a 30 to 45 degree angle relative to the skin. The syringe will fill on its own (ie, pulling the plunger is unnecessary). Approximately 2 to 3 m. L of blood should be removed.

5. To prevent coagulation, the syringe should be rolled between the hands for a few seconds to allow blood to mix with the heparin. 6. After withdrawing a sufficient volume of blood, the needle should be removed and pressure applied to the puncture site for five to ten minutes to achieve hemostasis.

Complications due to percutaneous needle puncture are rare. They include: *persistent bleeding *Bruising *injury to the blood vessel *Circulation distal to the puncture site may also be impaired following percutaneous needle puncture, presumably due to thrombosis at the puncture site.
 Indwelling catheters Arterial blood can also be obtained via an indwelling arterial")
. B) Indwelling catheters Arterial blood can also be obtained via an indwelling arterial catheter. Indwelling catheters provide continuous access to arterial blood, which is helpful when frequent blood gases are needed (eg, respiratory failure).

Venous blood gases and other alternatives to arterial blood gases An arterial blood gas (ABG) is the traditional method of estimating the systemic carbon dioxide tension and p. H, usually for the purpose of assessing ventilation and/or acid-base status. However, the necessary sample of arterial blood can be difficult to obtain due to diminished pulses or patient movement. Diminished pulses may reflect poor peripheral circulation or low blood pressure, while patient movement is frequently caused by the pain associated with arterial puncture.
 is an alternative method of estimating systemic carbon dioxide")
A venous blood gas (VBG) is an alternative method of estimating systemic carbon dioxide and p. H that does not require arterial blood sampling. Performing a VBG rather than an ABG is particularly convenient in the intensive care unit, since most patients have a central venous catheter from which venous blood can be quickly and easily obtained.

Sampling sites A VBG can be performed using a peripheral venous sample (obtained by venipuncture), a central venous sample (obtained from a central venous catheter), or a mixed venous sample (obtained from the distal port of a pulmonary artery catheter). Central venous blood gases are preferred because their correlation with arterial blood gases is the most well-established by research and clinical experience.

Peripheral venous blood gases are an alternative for patients who do not have central venous access. If a tourniquet is used to facilitate venipuncture, it should be released about one minute before the sample is drawn to avoid changes induced by local ischemia.

Mixed venous blood gases are a reasonable alternative for patients whose venous access is a pulmonary artery catheter; however, a pulmonary artery catheter should not be inserted for the sole purpose of venous blood sampling
, carbon dioxide tension")
Measurements A VBG measures the venous oxygen tension (Pv. O 2), carbon dioxide tension (Pv. CO 2), acidity (p. H), oxyhemoglobin saturation (Sv. O 2), and serum bicarbonate (HCO 3) concentration: • Pv. CO 2, venous p. H, and venous serum HCO 3 concentration are used to assess ventilation and/or acid-base status • Sv. O 2 is used to guide resuscitation during severe sepsis or septic shock, a process called early goal-directed therapy • Pv. O 2 has no practical value at this time. It is not useful in assessing oxygenation because oxygen has already been extracted by the tissues by the time the blood reaches the venous circulation. The inability of a VBG to measure oxygenation is the major drawback compared with an ABG. To overcome this limitation, VBGs are often considered in combination with pulse oximetry.

Correlation with arterial blood gases Central venous *The central venous p. H is usually 0. 03 to 0. 05 p. H units lower than the arterial p. H *the PCO 2 is usually 4 to 5 mm. Hg higher *little or no increase in serum HCO 3. Mixed venous blood gives results similar to central venous blood. peripheral venous *The p. H is approximately 0. 02 to 0. 04 p. H units lower than the arterial p. H *the venous serum HCO 3 concentration is approximately 1 to 2 meq/L higher *the venous PCO 2 is approximately 3 to 8 mm. Hg higher. There are no venous to arterial conversions for the central venous, mixed venous, or peripheral venous Pv. O 2 or Sv. O 2.

Misleading results The correlation between arterial and venous blood gas measurements varies with the hemodynamic stability of the patient. This observation has two practical consequences: First, clinicians should be wary of VBG results and preferentially obtain an ABG in hypotensive patients. Second, periodic correlation of the venous measurements with arterial measurements should be performed whenever venous measurements are used for serial monitoring.
 is another")
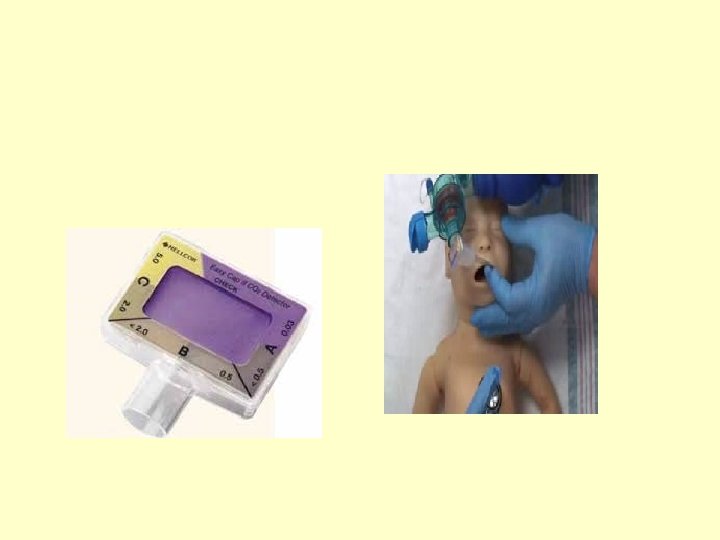
END-TIDAL CARBON DIOXIDE Measurement of end tidal carbon dioxide (Pet. CO 2) is another method of non-invasively estimating the arterial carbon dioxide tension (Pa. CO 2). This technique, called capnography, requires a closed system of gas collection, either with a tight fitting mask or a ventilator circuit. A sample of expired gas is analyzed by infrared or mass spectrometry, and then displayed as a numerical value or a graph. The Pet. CO 2 is usually within 1 mm of the Pa. CO 2 in healthy adults, but it is far less accurate in critically ill adults because of the dependence of CO 2 production on cardiac output. Thus, routine use of Pet. CO 2 exists primarily in newborn ICUs, operating rooms, and emergency departments, to provide early warning of endotracheal tube complications. Pet. CO 2 is reviewed in detail separately.
 and")
TRANSCUTANEOUS CARBON DIOXIDE Systems that measure both transcutaneous carbon dioxide (ptc. CO 2) and pulse oximetry are an attractive option because they overcome the major limitations of both ABGs (invasive arterial sampling) and VBGs (lack of information about oxygenation). Such combination systems generally have a heating element that raises the skin temperature to 42 to 45ºC to increase local perfusion, an electrode to measure ptc. CO 2, and a light emitter and sensor to measure arterial oxyhemoglobin saturation.

Older studies suggested that ptc. CO 2 measurements are accurate in neonates, but not critically ill adults because of poor peripheral perfusion (peripheral artery disease, hypotension, vasopressors). Devices have since improved and more recent observational studies suggest that the newer systems may be more accurate in critically ill patients, although their accuracy diminishes when the arterial carbon dioxide tension (Pa. CO 2) is greater than 56 mm. Hg.

Such combination systems have limitations: 1. They may be difficult to keep calibrated 2. may be difficult to mount in a way that prevents air trapping 3. may take up to an hour to sufficiently warm the skin. 4. the devices must be attached to an ear, which may be difficult in agitated patients or in those who had neurosurgery Given the limitations of noninvasive monitoring, any persistent or unexpected change in the ptc. CO 2 or oxyhemoglobin saturation should be confirmed with an ABG. Clinical trials are necessary before combined pulse oximetry and ptc. CO 2 monitoring become routine care.


Comparison of Blood Gas Analysis at different sites Arterial Capillary Venous • PH Same ----- Lower • PO 2 Higher ----- Lower • PCO 2 Lower Higher • HCO-3 Same ----- Same • Recommendation Good Fair Bad

SPECIMEN CARE Regardless of the method used to withdraw the arterial blood, several issues should be considered prior to sending the specimen to the laboratory: 1. Gas diffusion through the plastic syringe is a potential source of error. However, it appears that the clinical significance of the error is minimal if the sample is placed on ice and analyzed within 15 minutes. Using a glass syringe will also prevent this error. 2. The heparin that is added to the syringe as an anticoagulant can decrease in the p. H if acidic heparin is used. It can also dilute the Pa. CO 2, resulting in a falsely low value. Thus, the amount of heparin solution should be minimized and at least 2 m. L of blood should be obtained.

3. Air bubbles that exceed 1 to 2 percent of the blood volume can cause a falsely high Pa. O 2 and a falsely low Pa. CO 2. The magnitude of this error depends upon the difference in gas tensions between blood and air, the exposure surface area (which is increased by agitation), and the time from specimen collection to analysis. The clinical significance of this error can be decreased by gently removing the bubbles without agitation and analyzing the sample as soon as possible.
, which can cause a")
4. This reduces oxygen consumption by leukocytes (ie, leukocyte larceny), which can cause a factitiously low Pa. O 2. This effect is most pronounced in patients whose leukocytosis is profound. In addition, it reduces the likelihood that error due to gas diffusion through the plastic syringe or air bubbles will be clinically significant.

TRANSPORT The arterial blood should be placed on ice during transport to the lab and then analyzed as quickly as possible.

ANALYSIS Analysis of arterial blood is usually performed by automated blood gas analyzers, which automatically transport the specimen to electrochemical sensors to measure p. H, Pa. CO 2, and Pa. O 2: • The Pa. CO 2 is measured using a chemical reaction that consumes CO 2 and produces a hydrogen ion, which is sensed as a change in p. H • The Pa. O 2 is measured using oxidation-reduction reactions that generate measurable electric currents • Automated blood gas analyzers rinse the system, calibrate the sensors, and report the results. Rigorous quality control by the laboratory is essential for accurate results.

• Arterial blood gas measurements are effected by temperature. Specifically, p. H increases and both Pa. O 2 and Pa. CO 2 decrease as temperature declines. The effect of temperature on blood gas measurements

Modern automated blood gas analyzers can report the p. H, Pa. O 2, and Pa. CO 2 at either 37ºC (the temperature at which the values are measured by the blood gas analyzer) or at the patient's body temperature. Most centers report the values of p. H, PCO 2, and PO 2 at 37ºC, even if the patient's body temperature is different. However, this practice is controversial

Terminology of ABG • Acidemia — An arterial p. H below the normal range (less than 7. 36). • Alkalemia — An arterial p. H above the normal range (greater than 7. 44). • Acidosis — A process that tends to lower the extracellular fluid p. H (hydrogen ion concentration increases). This can be caused by a fall in the serum bicarbonate (HCO 3) concentration and/or an elevation in PCO 2. • Alkalosis — A process that tends to raise the extracellular fluid p. H (hydrogen ion concentration decreases). This can be caused by an elevation in the serum HCO 3 concentration and/or a fall in PCO 2.

• Metabolic acidosis — A disorder that causes reductions in the serum HCO 3 concentration and p. H. • Metabolic alkalosis — A disorder that causes elevations in the serum HCO 3 concentration and p. H. • Respiratory acidosis — A disorder that causes an elevation in arterial PCO 2 and a reduction in p. H. • Respiratory alkalosis — A disorder that causes a reduction in arterial PCO 2 and an increase in p. H.

• Simple acid-base disorder — The presence of one of the above four disorders with the appropriate respiratory or renal compensation for that disorder. • Mixed acid-base disorder — The simultaneous presence of more than one acid-base disorder. Mixed acid-base disorders can be suspected from the patient's history, from a lesser- or greater-than-expected compensatory respiratory or renal response, and from analysis of the serum electrolytes and anion gap. As an example, a patient with severe vomiting would be expected to develop a metabolic alkalosis due to the loss of acidic gastric fluid. If, however, the patient developed hypovolemic shock from the fluid loss, the ensuing lactic acidosis would lower the elevated serum HCO 3 possibly to below normal values, resulting in acidemia

INTERPRETATION ABGs provide information about oxygenation, ventilation, and acidbase balance • Acid-Base & ventilation Information • p. H • PCO 2 • HCO 3 [calculated vs measured] • Oxygenation Information • PO 2 [oxygen tension] • SO 2 [oxygen saturation]
 of carbon dioxide (CO")
Each day approximately 15, 000 mmol (considerably more with exercise) of carbon dioxide (CO 2, which can generate carbonic acid as it combines with water) and 50 to 100 meq of nonvolatile acid (mostly sulfuric acid derived from the metabolism of sulfur-containing amino acids) are produced. Acid-base balance is maintained by normal pulmonary and renal excretion of carbon dioxide and nonvolatile acid, respectively.

General principles in ABG interpretation The Henderson-Hasselbalch equation shows that the p. H is determined by the ratio of the serum bicarbonate (HCO 3) concentration and the PCO 2, not by the value of either one alone. Each of the simple acidbase disorders is associated with a compensatory respiratory or renal response that limits the change in ratio and therefore in PH. p. H = 6. 10 + log ([HCO 3 -] ÷ [0. 03 x PCO 2])
![Hydrogen Ions H+ is produced as a by-product of metabolism. [H+] is maintained in](http://slidetodoc.com/presentation_image_h/752c6c42951fa87d391a6a28d524ca1a/image-50.jpg "Hydrogen Ions H+ is produced as a by-product of metabolism. [H+] is maintained in")
Hydrogen Ions H+ is produced as a by-product of metabolism. [H+] is maintained in a narrow range. Normal arterial p. H is around 7. 4. A p. H under 7. 0 or over 7. 8 is compatible with life for only short periods.
![PH and [H+] (9 -p. H) + [ H ] in n. Eq/L =](http://slidetodoc.com/presentation_image_h/752c6c42951fa87d391a6a28d524ca1a/image-51.jpg "PH and [H+] (9 -p. H) + [ H ] in n. Eq/L =")
PH and [H+] (9 -p. H) + [ H ] in n. Eq/L = 10
![A normal [H+] of 40 n. Eq/L corresponds to a p. H of 7.](http://slidetodoc.com/presentation_image_h/752c6c42951fa87d391a6a28d524ca1a/image-52.jpg "A normal [H+] of 40 n. Eq/L corresponds to a p. H of 7.")
A normal [H+] of 40 n. Eq/L corresponds to a p. H of 7. 40. Because the p. H is a negative logarithm of the [H+], changes in p. H are inversely related to changes in [H+] (e. g. , a decrease in p. H is associated with an increase in [H+]). p. H [H+] 7. 7 7. 5 7. 4 7. 3 7. 1 7. 0 6. 8 20 31 40 50 80 100 160

Hydrogen Ion Regulation The body maintains a narrow p. H range by 3 mechanisms: 1. Chemical buffers (extracellular and intracellular) react instantly to compensate for the addition or subtraction of H+ ions. 2. CO 2 elimination is controlled by the lungs (respiratory system). Decreases (increases) in p. H result in decreases (increases) in PCO 2 within minutes. 3. HCO 3 - elimination is controlled by the kidneys. Decreases (increases) in p. H result in increases (decreases) in HCO 3 -. It takes hours to days for the renal system to compensate for changes in p. H.
![CENTRAL EQUATION OF ACID -BASE PHYSIOLOGY The hydrogen ion concentration [H+] in extracellular fluid](http://slidetodoc.com/presentation_image_h/752c6c42951fa87d391a6a28d524ca1a/image-54.jpg "CENTRAL EQUATION OF ACID -BASE PHYSIOLOGY The hydrogen ion concentration [H+] in extracellular fluid")
CENTRAL EQUATION OF ACID -BASE PHYSIOLOGY The hydrogen ion concentration [H+] in extracellular fluid is determined by the balance between the partial pressure of carbon dioxide (PCO 2) and the concentration of bicarbonate [HCO 3 -] in the fluid. This relationship is expressed as follows: [H+] in n. Eq/L = 24 x (PCO 2 / [HCO 3 -] ) where [ H+] is related to p. H by [ H+] in n. Eq/L = 10 (9 -p. H)

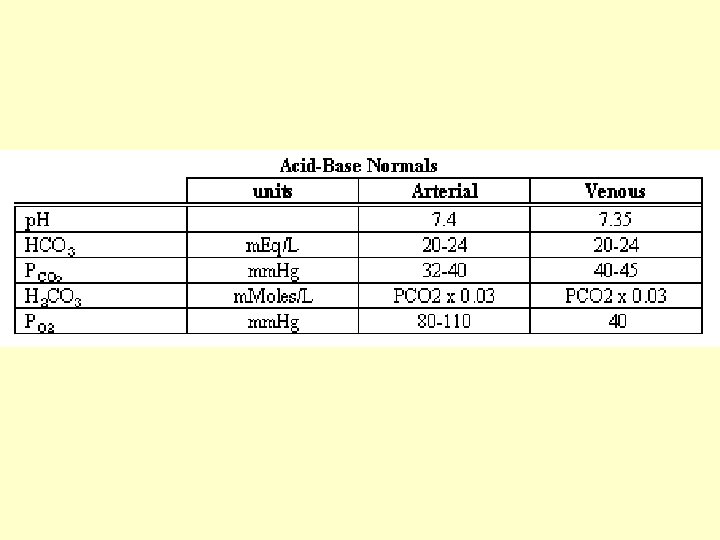
NORMAL VALUES Using a normal arterial PCO 2 of 40 mm Hg and a normal serum [HCO 3 - ] concentration of 24 m. Eq/L, the normal [H+] in arterial blood is 24 × (40/24) = 40 n. Eq / L When a primary acid-base disturbance alters one component of the PCO 2/[HCO 3 - ]ratio, the compensatory response alters the other component in the same direction to keep the PCO 2/[HCO 3 - ] ratio constant.
![PCO 2/[HCO 3 - ] Ratio Since [H+] = 24 x (PCO 2](http://slidetodoc.com/presentation_image_h/752c6c42951fa87d391a6a28d524ca1a/image-56.jpg "PCO 2/[HCO 3 - ] Ratio Since [H+] = 24 x (PCO 2")
PCO 2/[HCO 3 - ] Ratio Since [H+] = 24 x (PCO 2 / [HCO 3 -]), the stability of the extracellular p. H is determined by the stability of the PCO 2/HCO 3 - ratio. Maintaining a constant PCO 2/HCO 3 - ratio will maintain a constant extracellular p. H.

The respiratory compensation: When a metabolic acid-base disorder causes the serum HCO 3 to decrease (metabolic acidosis) or increase (metabolic alkalosis), there is usually an appropriate respiratory compensation that causes the PCO 2 to change in the same direction as the serum HCO 3 (falling in metabolic acidosis and rising in metabolic alkalosis). The respiratory compensation mitigates the change in the ratio of the serum HCO 3 to PCO 2 and therefore in the p. H. The respiratory compensation in metabolic acidosis or alkalosis is a rapid response that, in metabolic acidosis, begins within 30 minutes and is complete within 12 to 24 hours

The ventilatory control system provides the compensation for metabolic acid-base disturbances, and the response is prompt. The changes in ventilation are mediated by H+ sensitive chemoreceptors located in the carotid body (at the carotid bifurcation in the neck) and in the lower brainstem. *A metabolic acidosis excites the chemoreceptors and initiates a prompt increase in ventilation and a decrease in arterial PCO 2. *A metabolic alkalosis silences the chemoreceptors and produces a prompt decrease in ventilation and increase in arterial PCO 2.

Control System for Respiratory Regulation of Acid-base Balance Control Element Physiological or Anatomical Correlate Comment Controlled variable Arterial p. CO 2 A change in arterial p. CO 2 alters arterial p. H (as calculated by use of the Henderson. Hasselbalch Equation). Sensors Central and peripheral chemoreceptors Both respond to changes in arterial p. CO 2 (as well as some other factors) Central integrator The respiratory center in the medulla Effectors The respiratory muscles An increase in minute ventilation increases alveolar ventilation and thus decreases arterial p. CO 2 (the controlled variable).

The renal compensation: When a respiratory acid-base disorder causes the PCO 2 to increase (respiratory acidosis) or decrease (respiratory alkalosis), there is usually a renal compensation that causes the HCO 3 to change in the same direction as the PCO 2, thereby mitigating the change in p. H. These compensations are mediated by increased hydrogen ion secretion (which raises the serum HCO 3 concentration) in respiratory acidosis and decreased hydrogen ion secretion and urinary HCO 3 loss in respiratory alkalosis. The renal compensation takes three to five days for completion. As a result, the expected findings are different in acute (little or no renal compensation) and chronic (full renal compensation) respiratory acidbase disorders.

Renal excretion of acid is achieved by combining hydrogen ions with either urinary buffers to form titratable acid, mainly phosphate (HPO 42 - + H+ → H 2 PO 4 -), or with ammonia to form ammonium (NH 3 + H+ → NH 4+) When increased quantities of acid must be excreted by the kidney, the major adaptive response consists of increases in ammonia production (derived from the metabolism of glutamine) with a resultant increase in ammonium excretion into the urine.

The compensatory renal and respiratory responses are thought to be mediated, at least in part, by parallel p. H changes within sensory and regulatory cells including renal tubule cells and cells in the respiratory center. The magnitude of the compensatory response is proportional to the severity of the primary acid-base disturbance. An important clinical consequence of these compensations is that the diagnosis of an acid-base disorder requires measurement of the extracellular (usually arterial) p. H. The diagnosis cannot be made from the serum HCO 3 alone. A low value could represent either metabolic acidosis or the renal compensation to respiratory alkalosis, while a high value could represent either metabolic alkalosis or the renal compensation to respiratory acidosis. In addition, mixed acid-base disorders may be present.

The expected compensation for any given acid-base disorder has been determined empirically by observations in humans with either spontaneous or experimentally induced simple acid-base disorders The degree of compensation is usually calculated from the decrease or increase in arterial PCO 2 from its normal range (in metabolic acid-base disorders) or the decrease or increase in serum HCO 3 from its normal range (in respiratory acid-base disorders). This approach presumes that the patient had normal values prior to the onset of the acid-base disorder. Thus, in the absence of known baseline values, there is the potential for error if the patient had abnormal baseline values.

Metabolic acid-base disorders 1. Metabolic acidosis *The respiratory compensation to metabolic acidosis results in an approximately 1. 2 mm. Hg fall in arterial PCO 2 for every 1 meq/L reduction in the serum HCO 3 concentration. *The respiratory response to metabolic acidosis begins within 30 minutes and is complete within 12 to 24 hours. *The lag in respiratory compensation is not seen when the metabolic acidosis develops slowly (eg, 4 meq/L fall in serum HCO 3 over 15 hours).

*An inability to generate the expected respiratory response is usually indicative of significant underlying respiratory or neurologic disease, but can also be seen in patients with acute metabolic acidosis in whom there has not been adequate time for respiratory compensation to achieve completion. *Several other relationships have been used to determine the appropriate respiratory compensation to metabolic acidosis. These include: • Arterial PCO 2 = 1. 5 x serum HCO 3 + 8 ± 2 (Winters' equation) • Arterial PCO 2 = Serum HCO 3 + 15 • Arterial PCO 2 should be similar to the decimal digits of the arterial p. H (eg, 25 mm. Hg when the arterial p. H is 7. 25, a setting in which the serum HCO 3 concentration would be approximately 11 meq/L)

These formulas generally give similar results and there are no data on comparative efficacy A reasonable approach is to use the relationship rule that is easiest to remember and implement. *There is a limit to the maximum respiratory compensation that can be attained. In severe metabolic acidosis (eg, serum HCO 3 concentration less than 6 meq/L), the PCO 2 can be reduced to a minimum of 8 to 12 mm. Hg in individuals with normal neuro-respiratory function.

*In addition to assessing the respiratory compensation, another component in the evaluation of patients with metabolic acidosis is calculation of the serum anion gap to determine if it is normal or elevated. *Metabolic acidosis may be of the -high anion gap type -normal anion gap type (hyperchloremic) -combined normal and elevated anion gap acidosis. The latter often occurs with severe diarrhea, which generates a normal anion gap metabolic acidosis but can also lead to hypovolemia-induced lactic acidosis With high anion gap metabolic acidosis, comparing the change in anion gap (or the Δ anion gap) with the change in bicarbonate (or the Δ bicarbonate) may be helpful.

2. Metabolic alkalosis The respiratory compensation to metabolic alkalosis should raise the PCO 2 by 0. 7 mm. Hg for every 1 meq/L elevation in the serum HCO 3 concentration In severe metabolic alkalosis, the arterial PCO 2 can be as high as 55 mm. Hg, suggesting that hypoxia in individuals without underlying lung disease does not usually limit the respiratory compensation

• Limitations of the respiratory compensation It has been shown in dog studies that respiratory compensation for metabolic acidosis or alkalosis most effectively blunts changes in p. H acutely. If the metabolic disorder persists, on the other hand, respiratory compensation becomes less effective and can even have a detrimental effect on p. H The acute hyperventilatory response to metabolic acidosis causes a fall in PCO 2 and this will initially raise the arterial p. H toward normal. However, over time, the reduction in PCO 2 causes a further decrease in the serum HCO 3 concentration due to both reduced renal acid secretion and urinary HCO 3 loss; these changes are similar to those induced by primary respiratory alkalosis

The net effect of these two processes is that they tend to cancel one another out so that the arterial p. H with chronic metabolic acidosis is often the same whether or not respiratory compensation occurs. Furthermore, in studies in dogs, the respiratory response was occasionally maladaptive, and the secondary fall in serum HCO 3 actually caused the arterial p. H to fall below the level that would have existed in the absence of respiratory compensation.

Analogous findings have been demonstrated in chronic metabolic alkalosis in which the respiratory compensation (hypoventilation leading to a rise in PCO 2) causes increased renal acid secretion and a rise in the serum HCO 3 concentration similar to that induced by primary respiratory acidosis. The renal response to a high PCO 2 mitigates the p. H benefit of hypoventilation. As with chronic metabolic acidosis, studies in dogs showed that this effect could become maladaptive and raise the arterial p. H to a value higher than that which would have occurred in the absence of respiratory compensation

Respiratory acid-base disorders The compensatory response to respiratory acid-base disorders occurs in two stages: • The initial acute response is generated by blood, extracellular fluid, and cell buffering that causes the serum HCO 3 to increase (in respiratory acidosis) or decrease (in respiratory alkalosis) within minutes. The acute response is relatively modest. • A larger response generated by the kidney is called chronic compensation. This response begins soon after the onset of the primary respiratory disorder but requires 3 to 5 days to become complete. Because of this variation with time, different compensatory responses are expected with acute and chronic respiratory disorders

• With chronic respiratory acidosis, the kidney increases acid excretion in the form of titratable acid and ammonium, and also increases HCO 3 reabsorption to maintain the higher HCO 3 concentration • With chronic respiratory alkalosis, the kidney reduces acid excretion, and also excretes some HCO 3 to reduce the HCO 3 concentration. Renal tubular reabsorption of HCO 3 is also reduced. • These renal responses are carefully regulated. As an example, administering exogenous HCO 3 in the setting of chronic respiratory acidosis and relatively normal renal function results in the urinary excretion of the excess alkali without a further elevation in the serum HCO 3 concentration.

1. Respiratory acidosis The compensatory response to acute respiratory acidosis causes the serum HCO 3 concentration to increase by about 1 meq/L for every 10 mm. Hg elevation in the PCO 2 If the elevated PCO 2 persists, the serum HCO 3 will continue to gradually increase and, after three to five days, the disorder is considered chronic. Studies mostly performed in hospitalized patients found that the serum HCO 3 increases by 3. 5 to 4. 0 meq/L for every 10 mm. Hg elevation in PCO 2 in patients with chronic respiratory acidosis However, a later study in stable outpatients with chronic respiratory acidosis found a greater compensatory rise in serum HCO 3 of about 5. 0 meq/L per 10 mm. Hg elevation in PCO 2.

The compensatory response to mild to moderate chronic respiratory acidosis (PCO 2 less than 70 mm. Hg) results in an arterial p. H that is usually modestly reduced or in the low-normal range. Thus, moderate to severe acidemia in a patient with mild to moderate chronic respiratory acidosis is usually indicative of concurrent metabolic acidosis or superimposed acute respiratory acidosis. An arterial p. H of 7. 40 or higher suggests a concurrent metabolic alkalosis or acute respiratory alkalosis.

2. Respiratory alkalosis The compensatory response to acute respiratory alkalosis causes the serum HCO 3 concentration to fall by 2 meq/L for every 10 mm. Hg decline in the PCO 2. If the reduced PCO 2 persists for more than 3 to 5 days, then the disorder is considered chronic and the serum HCO 3 concentration should fall by about 4 to 5 meq/L for every 10 mm. Hg reduction in the PCO 2.

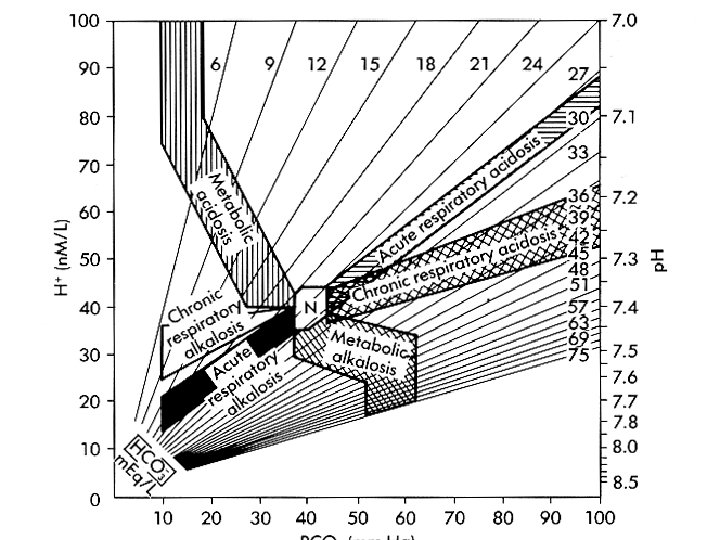
DIAGNOSIS There are four primary acid-base disorders: metabolic acidosis, metabolic alkalosis, respiratory acidosis, and respiratory alkalosis. Because the renal compensation to respiratory disorders takes 3 to 5 days to complete, the primary respiratory disorders can be further divided into acute and chronic respiratory acidosis and respiratory alkalosis. An important clinical consequence of the respiratory and renal compensations to acid-base disorders is that the diagnosis cannot be made with certainty from the serum HCO 3 alone. As an example, a low value could represent either metabolic acidosis or the renal compensation to respiratory alkalosis, while a high value could represent either metabolic alkalosis or the renal compensation to respiratory acidosis.
![PRIMARY AND SECONDARY ACID-BASE DERANGEMENTS End-Point: A Constant PCO 2/[HCO 3 - ]](http://slidetodoc.com/presentation_image_h/752c6c42951fa87d391a6a28d524ca1a/image-78.jpg "PRIMARY AND SECONDARY ACID-BASE DERANGEMENTS End-Point: A Constant PCO 2/[HCO 3 - ]")
PRIMARY AND SECONDARY ACID-BASE DERANGEMENTS End-Point: A Constant PCO 2/[HCO 3 - ] Ratio Acid-Base Disorder Primary Change Compensatory Change Respiratory acidosis PCO 2 up(10) HCO 3 up(1), (5) Respiratory alkalosis PCO 2 down(10) HCO 3 down(2), (4 -5) Metabolic acidosis HCO 3 down(1) PCO 2 down(1. 2) Metabolic alkalosis HCO 3 up(1) PCO 2 up(0. 7)

Expected Compensation in Acid-Base Disorders

EXPECTED CHANGES IN ACID-BASE DISORDERS Primary Disorder Expected Changes Metabolic acidosis PCO 2 = 1. 5 × HCO 3 + (8 ± 2) Metabolic alkalosis PCO 2 = 0. 7 × HCO 3 + (21 ± 2) Acute respiratory acidosis delta p. H = 0. 008 × (PCO 2 - 40) Chronic respiratory acidosis delta p. H = 0. 003 × (PCO 2 - 40) Acute respiratory alkalosis delta p. H = 0. 008 × (40 - PCO 2) Chronic respiratory alkalosis delta p. H = 0. 003 × (40 - PCO 2)

Normal Neonatal ABG values • PH: 7. 35 – 7. 45 • p. CO 2: 35 – 45 mm Hg • p. O 2: 50 – 70 mm Hg • HCO 3: 20 – 24 m. Eq/L • BE: +/- 5

NORMAL VALUES ACCORDING TO SITE OF SAMPLING — The range of normal values for acid-base parameters is different for arterial and venous samples and also varies among laboratories. • Arterial sample — For an arterial sample, the normal range for p. H is 7. 36 to 7. 44; for bicarbonate (HCO 3) concentration, 21 to 27 meq/L; and for PCO 2, 36 to 44 mm. Hg. • Peripheral venous sample — Normal values for peripheral venous blood differ from those of arterial blood due to the uptake and buffering of metabolically produced CO 2 in the capillary circulation. If a tourniquet is used to facilitate phlebotomy, it should be released about one minute before the sample is drawn to avoid changes induced by ischemia

In different studies, the peripheral venous range for p. H is approximately 0. 02 to 0. 04 p. H units lower than in arterial blood, the HCO 3 concentration is approximately 1 to 2 meq/L higher, and the PCO 2 is approximately 3 to 8 mm. Hg higher If venous measurements are used for serial monitoring, periodic correlation with arterial measurements should be performed. • Central venous sample — Central venous samples may be used in patients with central venous catheters. The central venous p. H is usually 0. 03 to 0. 05 p. H units lower than in arterial blood and the PCO 2 is 4 to 5 mm. Hg higher, with little or no increase in serum HCO 3.

ABG values vary with age of neonate:

ABG values vary with gestational age:

The Steps Approach to Solving Acid-Base Disorders

Accurate diagnosis of an acid-base disorder requires measurement of serum electrolytes to determine the serum HCO 3 concentration, the serum potassium (looking for hypokalemia or hyperkalemia which can accompany metabolic acid-base disorders), and the serum sodium and chloride concentrations to detect possible hyponatremia or hypernatremia and calculation of the serum anion gap. In addition, in patients with a high anion gap metabolic acidosis, analysis of the increase of the anion gap from its baseline divided by the reduction in bicarbonate from normal (ie, the Δ anion gap divided by the Δ bicarbonate, or "Δ/Δ") may be helpful.

A definitive diagnosis of acid-base disorders requires measurement of the arterial p. H and PCO 2 to identify the underlying disorder and to determine whether a mixed acid-base disorder exists. However, measurement of arterial p. H may not be required when the history and serum electrolytes clearly point toward a particular diagnosis. As an example, arterial blood gas analysis might not be required in a previously healthy patient with a recent history of severe diarrhea who has a low serum bicarbonate, hypokalemia, a normal anion gap, and no apparent cause of chronic respiratory alkalosis in which a low serum bicarbonate would represent the compensatory response.

Measurement of peripheral venous p. H and PCO 2 is an alternative, less invasive and more convenient approach than arterial measurements. However, venous measurements have some important limitations. As a result, arterial measurements are preferred. If venous measurements are used for serial monitoring, periodic correlation with arterial measurements should be performed. These issues are discussed in detail elsewhere.

• We suggest the following three-step approach in most patients: Step 1: Establish the primary diagnosis: *Metabolic acidosis is characterized by a low serum HCO 3 and a low arterial p. H; the serum anion gap may be increased or normal *Metabolic alkalosis is characterized by an elevated serum HCO 3 and an elevated arterial p. H *Respiratory acidosis is characterized by an elevated arterial PCO 2 and a low arterial p. H *Respiratory alkalosis is characterized by low arterial PCO 2 and an elevated arterial p. H

• Compensatory responses do not usually return the arterial p. H to normal. Thus, a normal arterial p. H in the presence of substantial changes in both serum HCO 3 and arterial PCO 2 is usually indicative of a mixed acid-base disorder (which could include an acute respiratory alkalosis produced by hyperventilation due to the discomfort of obtaining the blood sample). • However, there are two exceptions in which a simple acid-base disorder may be accompanied by a normal arterial p. H. Specifically, compensatory responses may return the arterial p. H to the highnormal range with mild to moderate chronic respiratory alkalosis, and to the low-normal range with mild to moderate chronic respiratory acidosis.

Step 2: Assess the degree of compensation A substantially reduced or excessive compensation is indicative of a mixed acid-base disorder. The degree of compensation is usually calculated from the change in arterial PCO 2 (in metabolic acid-base disorders) or serum HCO 3 (in respiratory acid-base disorders) from their presumed baseline normal values. The assumption that the patient had normal values prior to the onset of the acid-base disorder may be incorrect and introduces potential error.

The compensatory response must be correlated with the history. This is particularly true in respiratory acid-base disorders since the renal compensation occurs over 3 to 5 days. Thus, the expected compensation is smaller with acute compared with chronic disorders. As noted above, the normal compensatory response to respiratory acidosis is an increase in the serum HCO 3 concentration by about 1 meq/L for every 10 mm. Hg elevation in the PCO 2 acutely and about 3. 5 to 5. 0 meq/L for every 10 mm. Hg elevation in the PCO 2 if the underlying respiratory problem persists for three to five days or more.

Step 3: In patients with metabolic acidosis, determine if the anion gap is elevated If it is, then analyze the ratio of the increase in anion gap to the decrease in the HCO 3 concentration. This is the Δanion gap/ΔHCO 3 ratio. Interpretation of the anion gap and the Δanion gap/ΔHCO 3 ratio are discussed elsewhere. Step 4: Establish the clinical diagnosis Once the acid-base disorder is identified, the underlying cause or causes of the disorder should be determined and corrected.

• Case 1 — A patient with respiratory distress and an uncertain past history presents with an arterial p. H of 7. 32, an arterial PCO 2 of 70 mm. Hg, and a serum HCO 3 concentration of 35 meq/L, which is approximately 11 meq/L above the value seen in normal individuals. • These values are compatible with the expected renal compensation to chronic respiratory acidosis, although they are also compatible with a mixed acid-base disorder. • As an example, an acute respiratory acidosis causing a rise in PCO 2 to 70 mm. Hg should increase the serum HCO 3 by 3 meq/L to about 27 meq/L. If, however, this respiratory disturbance is superimposed on a metabolic alkalosis that raises the serum HCO 3 by an additional 8 meq/L to 35 meq/L, the resulting findings would be the same as those seen with a simple chronic respiratory acidosis. The history usually helps to distinguish among these possibilities.

• Case 2 — A patient with diarrhea has an arterial p. H of 7. 24, HCO 3 concentration of 10 meq/L, and arterial PCO 2 of 24 mm. Hg. • The low p. H indicates acidemia, and the low serum HCO 3 concentration indicates metabolic acidosis. The serum HCO 3 concentration of 10 meq/L is approximately 14 meq/L below normal. This should generate a 17 mm. Hg fall in the PCO 2 (14 x 1. 2 = 17) from 40 to 23 mm. Hg. Thus, this patient has a simple metabolic acidosis. • The other estimation equations for the degree of compensation cited above give similar results. Winters' equation predicts a PCO 2 of 23 mm. Hg (1. 5 x 10 +8 ± 2), the "HCO 3 + 15" rule predicts a PCO 2 of 25 mm. Hg, and the p. CO 2 is the same as the decimal digits of the arterial p. H.

• A PCO 2 significantly higher than the expected value would indicate a concurrent respiratory acidosis, as might occur if the patient were obtunded and had respiratory center depression. If, on the other hand, the PCO 2 were lower than 20 mm. Hg, then a concurrent respiratory alkalosis would be present. The combination of metabolic acidosis and respiratory alkalosis is often seen with salicylate intoxication or septic shock.

• Mixed acid-base disorders — Some patients have two, three, or more relatively independent acid-base disorders. • These mixed disorders include combinations of metabolic disorders (eg, vomiting-induced metabolic alkalosis plus hypovolemiainduced lactic acidosis), mixed metabolic and respiratory disorders (eg, metabolic acidosis and respiratory alkalosis in salicylate intoxication), and more complex combinations. • As discussed in the preceding section, the evaluation of patients with acid-base disorders initially requires identification of the major disorder, and then determination if the degree of compensation is appropriate. If the compensation is not appropriate, then this is indicative of a second acid-base disorder (ie, a mixed acid-base disorder is present).

The following examples are illustrative: • If metabolic acidosis is the primary disorder, an arterial PCO 2 substantially higher than the expected compensatory response defines the mixed disorder of metabolic acidosis and respiratory acidosis, while an arterial PCO 2 substantially lower than expected defines the mixed disorder of metabolic acidosis and respiratory alkalosis (which could be produced by acute hyperventilation due to the discomfort of obtaining the blood sample). • If respiratory acidosis is the major disorder, then the serum HCO 3 should be appropriately increased. If the serum HCO 3 is not as high as expected, then metabolic acidosis also exists and the arterial p. H may be substantially reduced. In contrast, if the serum HCO 3 is higher than expected, then metabolic alkalosis complicates the respiratory acidosis and the arterial p. H may be inappropriately "normal. "

• In patients with a high anion gap metabolic acidosis, a diagnosis of a mixed metabolic acidosis and a metabolic alkalosis generally requires calculation and interpretation of the Δ anion gap and the Δ HCO 3.

• Case 3 — Establishing the correct diagnosis may be more difficult with respiratory acid-base disorders, because of the difference between the acute and chronic compensatory responses. Consider the following arterial blood values: arterial p. H 7. 27, arterial PCO 2 70 mm. Hg, and serum HCO 3 31 meq/L. The low p. H and hypercapnia indicate that the patient has respiratory acidosis. If this is acute hypercapnia, then the 30 mm. Hg rise in PCO 2 should increase the serum HCO 3 concentration by 3 meq/L (to about 27 meq/L). If this is chronic hypercapnia, the serum HCO 3 should increase by 11 meq/L (to about 35 meq/L).

The observed value of 31 meq/L is between these expected levels and could have multiple explanations, including: 1. Chronic respiratory acidosis with a superimposed metabolic acidosis that has reduced the serum HCO 3 from 35 to 31 meq/L. This might occur in a patient with chronic obstructive pulmonary disease who developed diarrhea due to viral gastroenteritis or lactic acidosis from sepsis. 2. Acute respiratory acidosis with a superimposed metabolic alkalosis that has increased the HCO 3 from 27 to 31 meq/L. This could occur in a patient with respiratory depression due to a sedating drug who also developed vomiting or was taking diuretics.

3. Acute respiratory acidosis superimposed on mild chronic respiratory acidosis. Suppose, for example, that a patient has chronic respiratory acidosis with a PCO 2 of 55 mm. Hg and an appropriate serum HCO 3 of 30 meq/L. The patient then develops pneumonia, which acutely increases the p. CO 2 to 70 mm. Hg. The serum HCO 3 would rise further to about 31 meq/L. 4. Acute respiratory acidosis that is evolving into a chronic disorder (between 1 and 3 days).

• Thus, the correct diagnosis in a primary respiratory acid-base disorder can be established only when correlated with the clinical history and physical examination. • This is true even when the arterial blood values appear to represent a simple disorder. If the serum HCO 3 concentration had been 35 meq/L in this example, the findings would have been compatible with an uncomplicated chronic respiratory acidosis. However, similar findings could have been induced by acute respiratory acidosis plus metabolic alkalosis. • The history usually helps to distinguish among the possibilities and serial blood gas measurements and serum chemistries should be performed.

Some Aids to Interpretation of Acid-Base Disorders "Clue" Significance High anion gap Always strongly suggests a metabolic acidosis. Hyperglycaemia If ketones present also diabetic ketoacidosis Hypokalemia and/or hypochloremia Suggests metabolic alkalosis Hyperchloremia Common with normal anion gap acidosis Elevated creatinine and urea Suggests uremic acidosis or hypovolemia (prerenal failure) Elevated creatinine Consider ketoacidosis: ketones interfere in the laboratory method (Jaffe reaction) used for creatinine measurement & give a falsely elevated result; typically urea will be normal. Elevated glucose Consider ketoacidosis or hyperosmolar nonketotic syndrome Urine dipstick tests for glucose and ketones Glucose detected if hyperglycaemia; ketones detected if ketoacidosis http: //www. anaesthesiamcq. com/Acid. Base. Book/ab 9_2. php

The End
- Slides: 108