Introduction to Pediatric Nephrology Dr Fahad Gadi MD













 l l l Glomerular filtration begins between the 9 th")





: Obstructive nephropathy- 47% Reflux nephropathy- 18, 5% Hypo/dysplasia 8,")













 refluxes part-way up")





- Slides: 43
Introduction to Pediatric Nephrology Dr. Fahad Gadi, MD Pediatrics Demonstrator King Abdulaziz University Rabigh Medical School
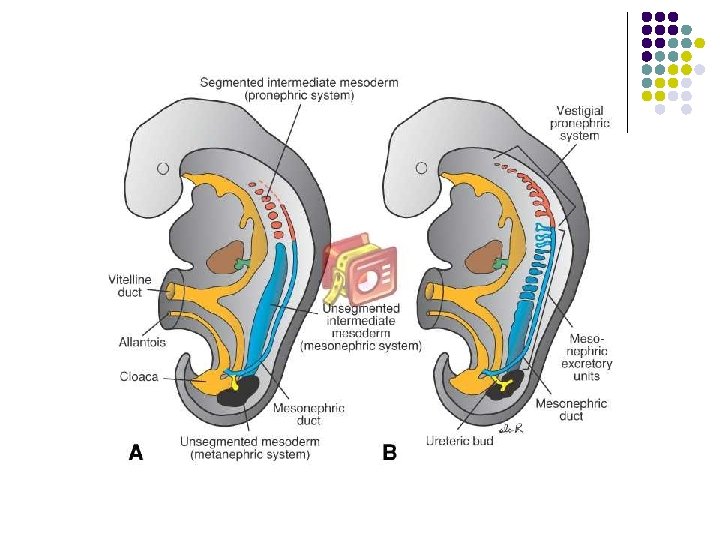
Kidney ontogenesis l l The embryological development of the kidney is a long and continuous process which begins in the 3 rd week and is completed by about 34 -35 weeks of fetal life. Kidney organogenesis is characterised by 3 distinct and linked stages: pronephros, mesonephros and metanephros.
Kidney ontogenesis l In humans, the first two are transient structures with little excretory capacity but they are important for the appropriate development of the metanephros, which is the direct precursor of the adult kidney.
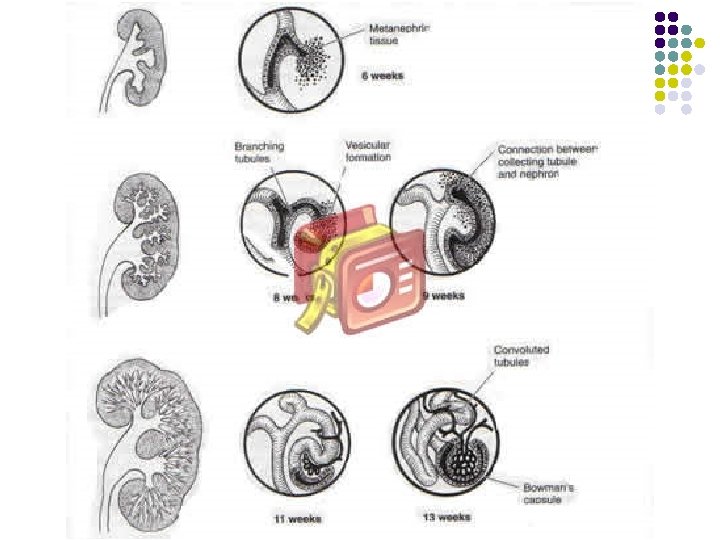
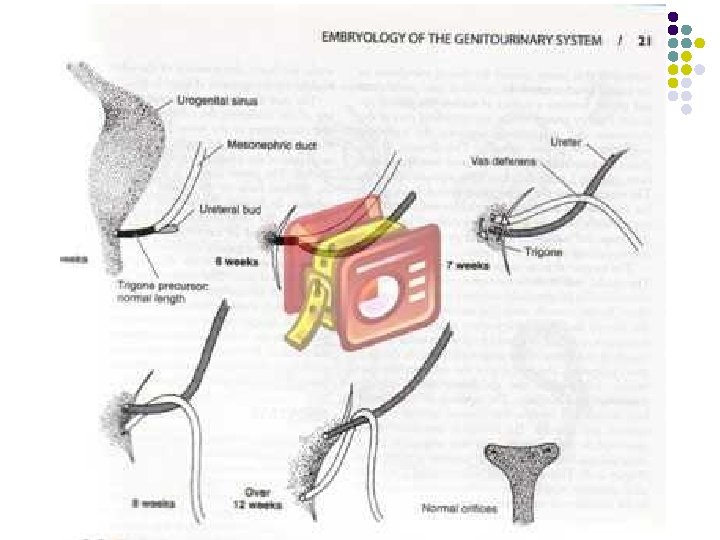
METANEPHROS l l l The final stage of the kidney is the differentation of the metanephros and arise from the ureteric bud and the metanephric blastema (mesenchyme). The renal pelvis, major and minor calyces and terminal collecting duct are formed by the 10 -13 th wks of ges. After morphogenesis each kidney contains approx a million nephrons.
Renal development Pronephros aorta nefrotomy Przednercze 3 t. ż. 4 -8 t. ż. Mesonephros przewód Wolffa Śródnercze 5 t. ż. Metanephros stek pączek moczowodowy blastema nerki ostatecznej Nerka ostateczna
Antenatal Period l l l The most common cause is physiologic dilation. Metanephric urine production begins at 8 weeks, even before ureteral canalization is complete. Transient obstruction with hydronephrosis occurs.
Embryology
MOLECULAR ASPECT l l The development of the metanephric kidney depends on inductive interaction between the ureteric bud (UB) and the metanephric mesenchyme (MM). A large number of genes have been found to be crucial during kidney development.
Nephrons l l In the fetus at 36 weeks’ gestation there is an adult complement of nephrons- approx. one million All further growth of the kidney is via hyperplasia mainly in the tubules.
Fetal kidney l l Nephrogenesis is completed between the 28 and 36 th gestational week in the human, the renal tissue and particularly the tubular cells continue to develop postnatally. Several of the major transporters in the tubular epithelial cells undergo postnatal maturation
Fetal kidney l l Outer cortical glomeruli are relatively underperfused compared with inner cortical glomeruli. Following birth, renal perfusion to superficial cortical nephrons rises compared with deeper glomeruli
Fetal kidney l Angiotensin-converting enzyme inhibitors and angiotensin-receptor antagonists impair nephrogenesis and so are contraindicated in pregnancy
Production of urine l l l Production of urine starts at the age of 10 -12 weeks of gestation: 1. very dilute urine 2. small amount of urine Fetal urine is a major constituent of amniotic fluid and urinary flow rate increases from 12 ml/hr at 32 weeks’gestation to 28 ml/hr at 40 weeks’gestation. Similar increases are described during the maturation of premature newborns.
Glomerular Filtration Rate (GFR) l l l Glomerular filtration begins between the 9 th and 12 th week of gestation in humans. The GFR is relatively low at birth especially in the premature infant. The values of GFR nearly double between 3 and 7 days and thereafter GFR continues to increase, by 1 to 2 yrs of age the GFR is the same as in an older child- 80% of mature kidney.
GFR
Kidney of newborn l l The kidney of the newborn infant has a limited capacity to regulate the excretion of fluid and electolytes. The high sodium excretion during the first 2 to 3 weeks often results in a negative sodium balance and predisposes to hyponatremia.
Creatinine Clearance l l Newborn: 40 -65 ml/min/1. 73 m 2 <40 yrs: 97 -137 ml/min/1. 73 m 2
Renal failure in the newborn l l l Renal failure in the newborn: severe asphyxia, the majority suffered from nonoliguric renal failure
CAKUT l l l Congenital Anomalies of Kidney and Urogenital Tract
CAKUT Chronic renal failure (children): Obstructive nephropathy- 47% Reflux nephropathy- 18, 5% Hypo/dysplasia 8, 7% l
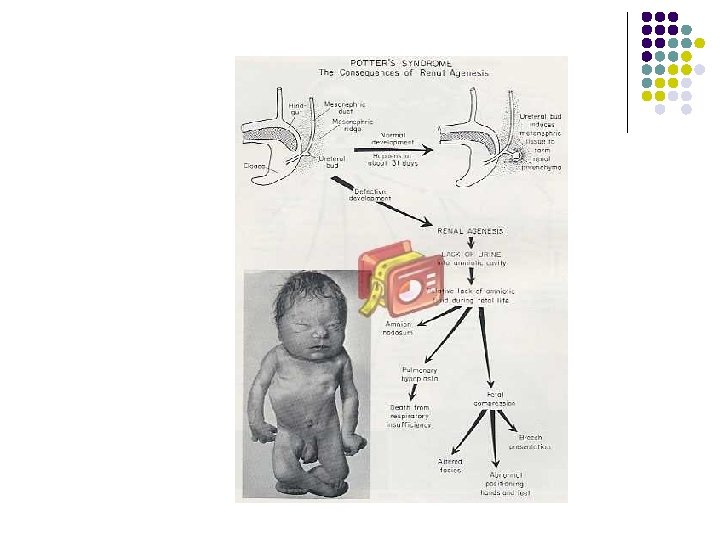
RENAL ABNORMALITIES l Renal agenesis: bilateral fetal death- Potter syndrome 1: 4000 pregnancies unilateral other organ- 1: 2900 pregnancies abnormalites
Renal abnormalities Agenesis Aplasia Hypoplasia
RENAL ABNORMALITIES l Hydronephrosis
RENAL ABNORMALITIES l Obstractive uropathy: A. ureteropelvic junction obstruction- dilated renal pelvis with/ without caliectasis and no dilation of the ureter B. ureterovesical junction obstruction (megaureter)pelviectasis and caliectasis with significant ureter dilation
RENAL ABNORMALITIES l l C. posterior urethral valve D. ureterocele- cystic dilatation of the distal ureter that protrudes into the urinary bladder, may extend past the bladder into urethra E. ectopic ureters F. constriction (stenosis)of urethra
Posterior urethral valve Type I – Type III
Duplication of urinary tract Ureter duplex Ureter fissus Ureter
Vesico-ureteral reflux Frequency of VUR • Isolated • UTI in the past • Siblings with VUR • Mothers with VUR in the past 1% (0. 4 -4%) 29 -50% 32 -45% 60%
RENAL ABNORMALITIES l Polycystic kidney: autosomal dominant p. k. disease autosomal recessive p. k. disease
Kidney ontogenesis
PRONEPHROS l l l Pronephros is a transitory nonfunctional kidney, the first tubules appear the middle of the 3 rd week and arise from intermediate mesodermal cells. The pronephric tubules persist for only a short time and undergo degeneration by the 5 th week. At the time the pronephros is degenerating the mesonephric tubules and duct are developing.
Pronephros
Vesico- ureteral reflux Normal kidney, ureter, and bladder
Vesico- ureteral reflux Grade I Vesicoureteral Reflux: urine (shown in blue) refluxes part-way up the ureter
Vesico- ureteral reflux l Grade II Vesicoureteral Reflux: urine refluxes all the way up the ureter
Vesico- ureteral reflux l Grade III Vesicoureteral Reflux: urine refluxes all the way up the ureter with dilatation of the ureter and calyces (part of the kidney where urine collects)
Vesico- ureteral reflux l Grade IV Vesicoureteral Reflux: urine refluxes all the way up the ureter with marked dilatation of the ureter and calyces
Vesico- ureteral reflux l Grade V Vesicoureteral Reflux: massive reflux of urine up the ureter with marked tortuosity and dilatation of the ureter and calyces
International Classification of VUR Io IIIo IVo Vo