The real preventive service a dental hygienist can



































 u. Scale")

 u. Scale")

: u. Scale")















































































- Slides: 156
“The real preventive service a dental hygienist can perform is to recognize early signs of periodontal involvement so that treatment can be initiated to arrest the disease and prevent more severe involvement…The difficult part is to watch carefully for incipient, often isolated indications of early periodontal disease. ” Ester Wilkins 6 th Edition, Clinical Practice of the Dental Hygienist
u. Periodontal disease is episodic in nature and site specific. u. Identifying small, incipient changes is our goal. u. Hygienists need to have assistance to be effective.
Why? ? ? u. Patient is brought into their treatment. u. Takes one third the amount of time. u. Keeps the infection control chain linked. u. Creates dialogue to help facilitate communication with patient
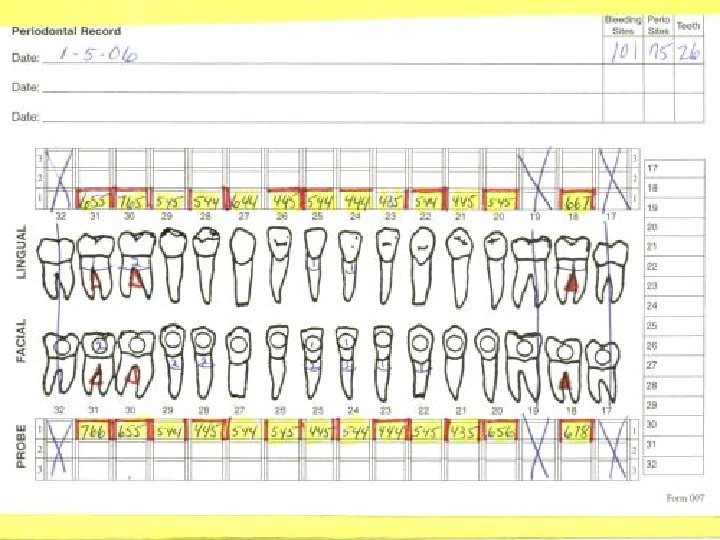
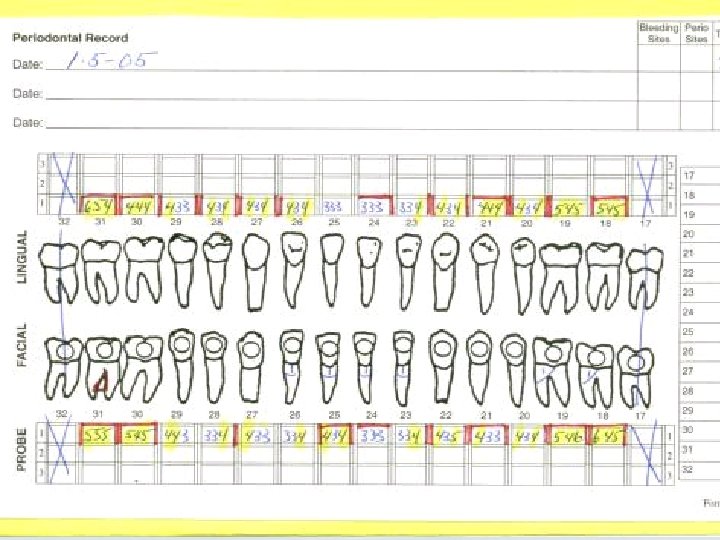
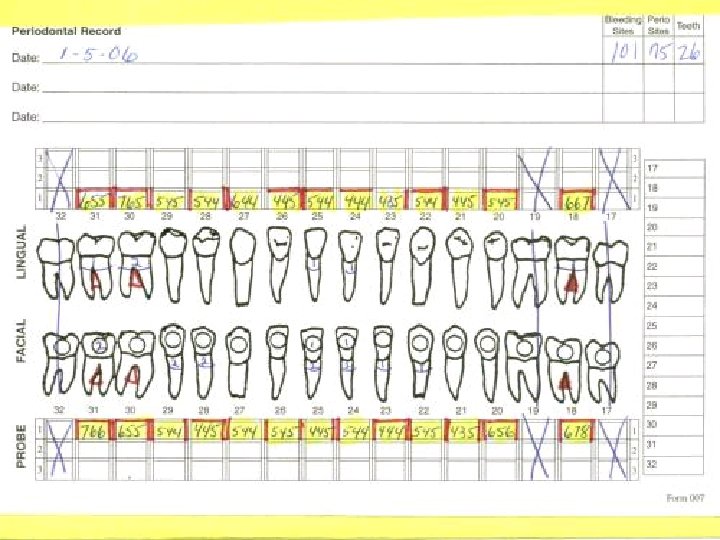
Effective Periodontal Charting In 5 -7 Minutes u. Five recordings necessary to develop treatment plan. v. Pocket depths v. Bleeding v. Recession v. Furcations v. Mobility
Class I Furcation Fig. III-10
Class II Furcation Fig. III-11
Class III Furcation Fig. III-12
Together Everyone Accomplishes More
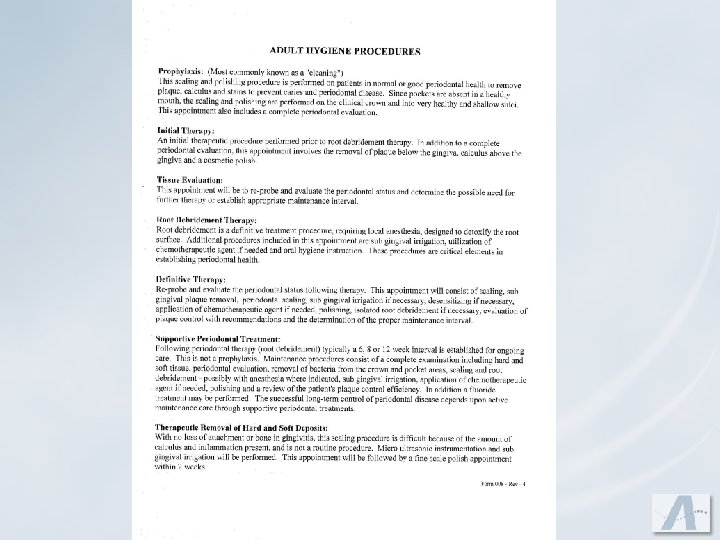
Hygiene Appointment Menu u. Prophy u. Therapeutic Removal of Hard & Soft Deposits u. Initial therapy u. Root Debridement/Detoxification therapy u. Definitive therapy u. Tissue evaluation u. Laser therapy u. Supportive periodontal treatment u. Full Mouth Debridement u. Child prophy and fluroide
Prophy u. CDT 2016 : Removal of plaque, calculus and stain from permanent and transitional dentition. It is intended to remove irritating factors. u. Workbook Definition: “this is a light supra and sub calculus removal and polish in the presence of a healthy mouth. Emphasis on instrumentation to remove coronal plaque, calculus, and stain. Evaluate personalized oral hygiene care. ” u. Key Words u. Never used to treat periodontal disease
Therapeutic Removal of Hard & Soft Deposits u. Workbook Definition: Scaling in presence of moderate or severe inflammation- full mouth u. Used to treat gingivitis u. Followed up with a prophy
Initial Therapy u. Workbook Definition: You have two choices for this treatment depending on your patient: v. Supra-gingival calculus removal, subgingival plaque removal and cosmetic polish. Or: v. Scale and polish only the healthy teeth u. Used as a transitional appointment for existing patients
Root Debridement Therapy u. Workbook Definition: Periodontal scaling, root debridement and detoxifying of the roots using anesthesia, ultrasonics, laser if available, and antimicrobial irrigation. Customize individual plaque control program. u 1993 standard of care in the treatment of periodontal disease changed from “root planning” to “root debridement” u. Root planning verses root debridement
Root Debridement Therapy Root Planing Root Debridement Aggressive Less-aggressive Treats Roots Treats Pathogens Removes Cementum Removes Toxins Technique uses heavy pressure Technique uses light pressure More operator fatigue Less operator fatigue Sensitivity usually results Little sensitivity results Goal is to remove the outer layer of cementum which holds the calculus which was believed to cause periodontal disease Goal is to stimulate the immune response by removing the loose plaque (which is the most destructive plaque). In turn this creates an environment conducive to healing.
Definitive Therapy u. Workbook Definition: Re-probing, light scale and polish or possible re-root debridement in an isolated area. Possible irrigation. Evaluating periodontal status and setting up on maintenance interval. u. This is the most important appointment in the entire series of periodontal appointments. u. Done 4 to 6 weeks after the last Root Debridement Therapy
Supportive Periodontal Treatment u CDT 2016 Definition: This procedure is instituted following periodontal therapy and continues at varying intervals, determined by the clinical evaluation of the dentist, for the life of the dentition or any implant replacements. It includes removal of the bacterial plaque and calculus from supragingival and subgingival regions, site specific scaling and root planning where indicated, and polishing the teeth. If new or recurring periodontal disease appears, additional diagnostic and treatment procedures must be considered. u Scheduled 8 to 12 weeks after the definitive therapy appointment. May be a shorter interval if the patient warrants a shorter interval. u Workbook Definition: To be used for patients who have completed periodontal therapy. Complete probing, periodontal scale, fine scale, subgingival plaque removal, and polish with possible isolated root debridement with anesthesia. (Laser practices will also incorporate lasers) u Scheduled 8 to 12 weeks after the definitive therapy appointment. May be a shorter interval if the patient warrants a shorter interval.
Supportive Periodontal Treatment u. Periodic maintenance treatment following periodontal therapy is not synonymous with a prophylaxis. u. Procedures: v. Complete periodontal probing – General fine scale v. Periodontal scale – Removal of subgingival plaque v. Treatment of 3 -4 isolated sites with root debridement incorporating anesthesia if necessary. (Laser practices will treat 2 -3 isolated sites and incorporate the utilization of the laser) v. Polish – Antimicrobial Irrigation – Desensitizing agent
Tissue Evaluation u. Workbook Definition: Re-probing and evaluation of need for further treatment. u. This is a 20 minute appointment u. No instrumentation besides periodontal charting u. Used predominately for gingivitis patients
Full Mouth Debridement u. Workbook Definition: General scale to enable periodontal evaluation u. The old “duck and cover” u. Key Components of this appointment: v. Remove gross calculus with ultrasonic v. Educate the patient of the need to return to have a full periodontal evaluation now that you can get the probe subgingivally
Child Prophy and Fluoride u. Workbook Definition: Light calculus and stain removal with polish/fluoride u. When do you charge for an adult prophy? u. How much time do you allot for a pedo prophy?
Case Typing u. Unified philosophy of treatment specific to your office u. Facilitates quick treatment planning u. Communication between hygienists u. Easy scheduling and financial presentations u. Subjective Information u. Objective Information u. Inflammation is Key
Root Causes of Disease
u…anything that elevates the inflammatory response may also speed the formation of amyloid plaques (cell-killing plaques that form in our brains). Steven Feske, M. D. Harvard Medical School Newsweek: October 3, 2005 u “In recent years, increasing evidence has supported the concept that the relationship between systemic and oral health is bi-directional. Much research has documented the association between periodontitis and its effects on preterm delivery and low birth weight newborns. Studies have also indicated that periodontal disease can increase the risk for cardiovascular disease, respiratory diseases, osteoporosis, and accelerate the progression of diabetes. The general mechanism behind the systemic effects of periodontitis is thought to involve, in part, a systemic inflammatory response through blood-borne oral lipopolysaccharides and oral bacteria. ”Ray C. Williams, DMD Chair, Department of Periodontology University of North Carolina School of Dentistry January, 2005
u It is evident that we can no longer view gingivitis simply as a precursor of periodontitis, but we should treat it as oral inflammation that needs to be controlled and eliminated for the overall well being of the individual. Ray C. Williams, DMD Chair, Department of Periodontology University of North Carolina School of Dentistry January, 2005 u “This is the most direct evidence yet that gum disease may lead to stroke or cardiovascular disease, ” said Dr. Moise Desvarieux at Columbia University Medical Center, who led the study. “And because gum infections are preventable and treatable, taking care of your oral health could very well have a significant impact on your cardiovascular health. ” AHA Circulation Magazine u There is growing evidence that chronic low-grade inflammation contributes to the development of many diseases, including Alzheimer's… Dr. Andrew Weil November 16, 2005
50% of your success with periodontal therapy is patient compliance!!
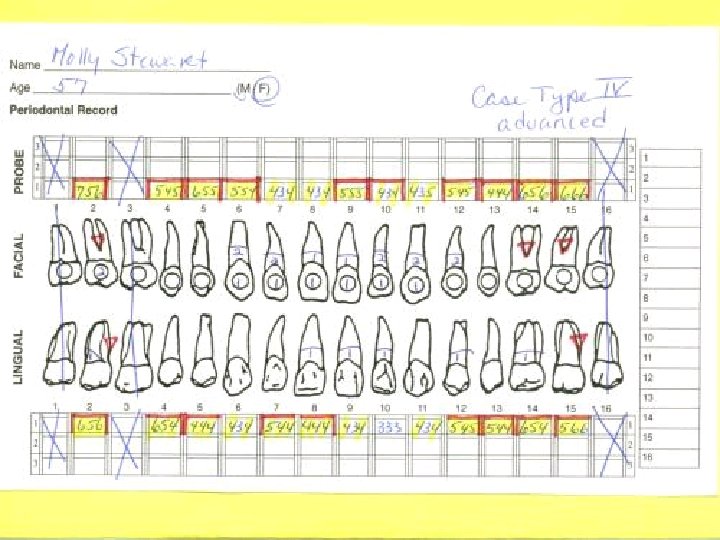
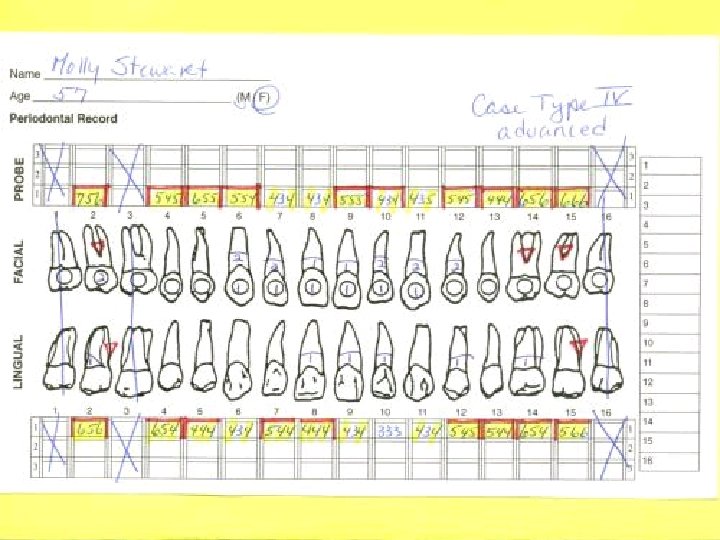
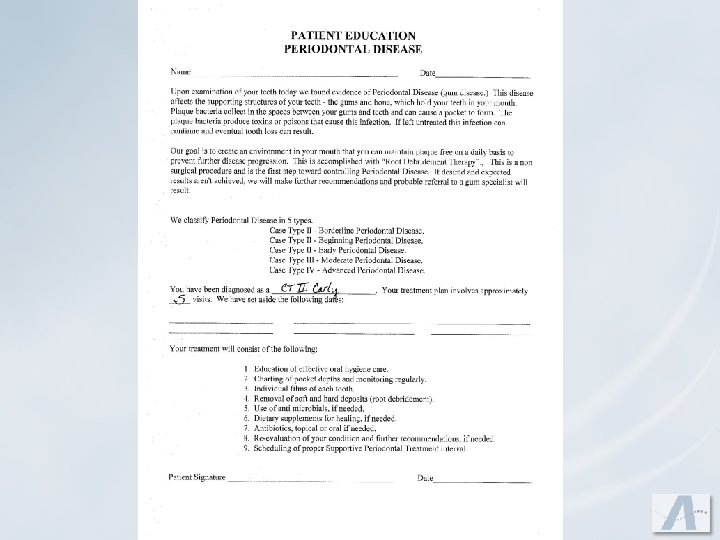
Current Case Types: Case Type I Gingivitis Case Type II Early Periodontitis (3 -4 mm) Case Type III Moderate Periodontitis (4 -6 mm) Case Type IV Advanced Periodontitis (6 mm and greater)
Our Case Types: Case Type I Gingivitis Case Type II Early Periodontitis (3 -4 mm) Case Type III Moderate Periodontitis (4 -5 mm) Case Type IV Advanced Periodontitis (6 mm and up) u. Mild u. Moderate u. Borderline u. Beginning u. Early
Healthy: u. Gingival tissue pink, firm stippled with minimal sulcus depth. u. Treatment Plan: v. Prophy v 3 or 6 month continuing care
Case Type I – Mild Gingivitis: u. Generalized bleeding points with light deposits. Isn’t really a healthy mouth, but doesn’t warrant a series of appointments.
Case Type I – Mild Gingivitis: Treatment Plan: u. Prophy – 60 minutes Followed up with either a: u. Tissue Evaluation – 20 minutes Or: u 3 month continuing care
Case Type I – Moderate Gingivitis: u. Clinical signs will either be red, inflamed, bulbous, rounded or blunted papilla that bleed easily, or firm, hard tissue with loss of stippling.
Case Type I – Moderate Gingivitis: Treatment Plan: u. Therapeutic Removal of Hard and Soft Deposits u. Fine Scale/polish u 3 month continuing care
Case Type II – Borderline Periodontitis u. Clinical healthy with one to three isolated 4 mm bleeding pockets. Treatment Plan: u. Prophy u 60 minute Root Debridement/Detoxification u 12 week Supportive periodontal treatment
Case Type II – Beginning Periodontitis u. Clinically you will see 3 -4 mm recordings with the 4 mm typically around the molars
Case Type II – Beginning Periodontitis Treatment Plan: Initial Therapy (Two Options) u. Scale and polish the healthy teeth or: u. Overall general debridement Root Debridement Therapy 4 to 6 weeks later: u. Definitive Therapy u 12 week Supportive Periodontal Treatment
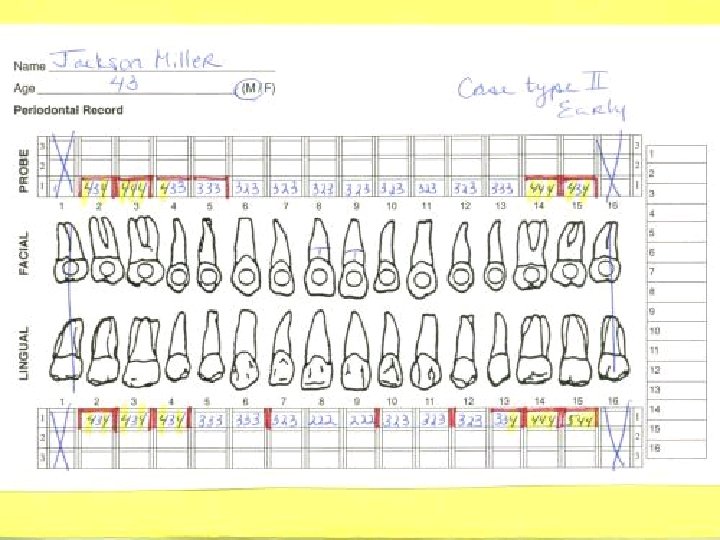
Case Type II – Early Periodontitis u. Clinically 3 to 4 mm pockets but the 4 mm pockets are more profuse and confined to the molars still but creeping into the bicuspids. You may have an isolated 5 mm pocket at this level.
Case Type II – Early Periodontitis Treatment Plan: Initial Therapy (Two Options) u. Scale and polish the healthy teeth or: u. Overall general debridement Root Debridement Therapy 4 to 6 weeks later: u. Definitive Therapy u 12 week Supportive Periodontal Treatment
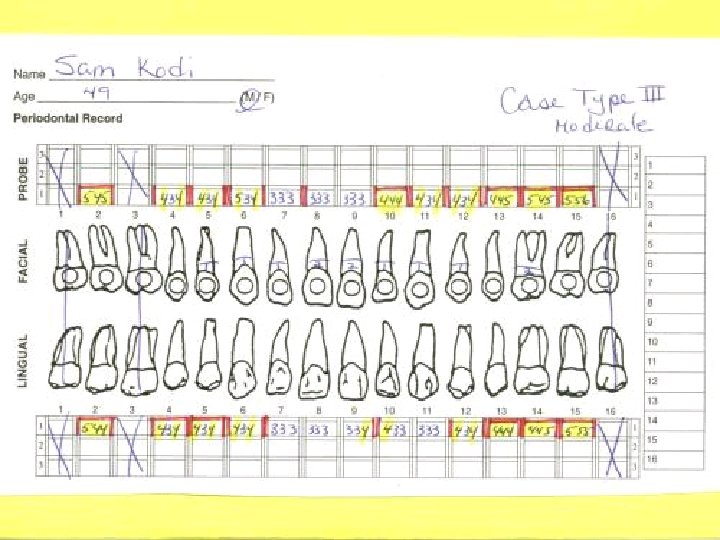
Case Type III – Moderate Periodontitis u. Clinically there will be generally 4 to 5 mm readings. There could be an isolated 6 mm pocket, too.
Case Type III – Moderate Periodontitis Treatment Plan: Initial Therapy (Two Options): u. Scale and polish the healthy teeth or: u. Overall general debridement Root Debridement Therapy Root Debridement Therapy 4 to 6 weeks later: u. Definitive Therapy u 8 to 12 week Supportive Periodontal Treatment
Case Type IV – Advanced Periodontitis u. Clinically you will see generally 5 to 6 mm and greater Treatment Plan: u. Initial Therapy v. Complete FMX u. REFER u. TRACK
Case Type IV – Advanced Periodontitis Treatment Plan: Initial Therapy u. Complete FMX REFER TRACK
“We are what we repeatedly do. Excellence, then, is not an act, but a habit. ” -Aristotle
“Put it on my Visa. ”
“Put it on my Visa. ”
“I forgot my checkbook. ”
What Will Do the Most Damage to a Patient/Doctor Relationship?
A Financial Misunderstanding
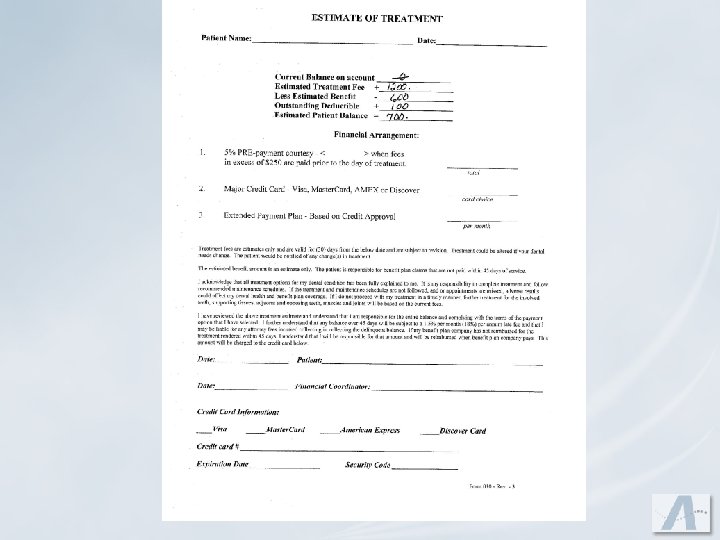
Financial Consultation and Written Financial Agreement
The Benefits of Having a Financial Policy! u. Increased patient satisfaction u. Diffuses patient confrontation u. Decreases phone time u. Increases cashflow by decreasing accounts receivable u. Decreasing A/R
Written Financial Agreement u. Don’t break down periodontal treatment – present total fee. u. Include previous balance u. How do you expect to be paid? u. Agreement between you and the patient u. If you accept benefit assignments, what happens if you are not paid in a timely manner by their benefit company?
Setting Fees Reflection of the Level of Care you Provide
Exam Codes u. D 0120 Periodic exam u. D 0140 Limited exam, problem focused u. D 0150 Comprehensive exam
X-ray Codes u. D 0210 u. D 0220 u. D 0230 u. D 0272 u. D 0274 Full mouth x-rays First periapical Additional periapical Two bite wing x-rays Four bite wing x-rays
Hygiene Codes u. D 1110 u. D 0120 u. D 1206 u. D 4346 deposits u. D 4341 u. D 4999 u. D 4910 Adult prophy Child prophy Fluoride varnish Theraupeutic removal hard & soft Root debridement Definitive therapy Supportive periodontal treatment
What is a Dental Expense Partial Reimbursement Plan?
What Were Annual Dental Maximums 40 Years Ago? ? u$1, 000 u$1, 500 u$2, 000
What Were Annual Dental Maximums 20 Years Ago? ? u$1, 000 u$1, 500 u$2, 000
What Are Annual Dental Maximums NOW? ? u$1, 000 u$1, 500 u$2, 000
Who Has the Largest Buildings in Big Cities? ?
Insurance Companies
Insurance Maximums 40 Years and 10 Years WHAT HAS CHANGED? Increased Premiums Managed Care Exclusions Waiting Periods Table of Allowances PPO
Partial Dental Benefit Reimbursement Philosophy u. Dental benefit program will “assist” patients. u. Administrative team “understands” dental insurance. u. The contract for dental benefits is between patient and employer u. Not all dental services are a covered benefit in all contracts. u. Doctor diagnoses and treats dental needs, not dental benefit plans.
“Secrets” for Submitting Effective Benefit Plan Claims u. Electronic claims get paid first u. Computer generated claims get paid second u. A motivated and informed patient u. Diagnosis Codes u. Narratives
A Motivated, Informed Patient u. Clear Communication v. Patient wants to have their disease treated u. Realistic Financial Consultation
Diagnostic Codes u. Case Type I – 4500 v. Gingivitis u. Case Type II – 4600 v. Borderline v. Beginning v. Early u. Case Type III – 4700 v. Moderate u. Case Type IV – 4800 v. Advanced
Narratives Initial Therapy – D 1110 Patient presented for a prophy, periodontal pockets present, performed an initial therapy as well as a scale and polish of the healthy teeth.
Narratives Tissue Evaluation – D 0140 Re-evaluation of chronic periodontitis to include full mouth probe and examination. Re-evaluation of periodontal condition.
Narratives Supportive Periodontal Treatment – D 4910 This patient has undergone active periodontal therapy (treatment completed xx/xx/xx) and is now receiving periodic ongoing treatment. Research has shown that periodic (12 week) ongoing treatment offers the patient the best chance for maintaining periodontal health.
Explosion Codes Explosion codes are a way to show a patient via statements all the services received for a specific hygiene appointment. Once entered when you enter a specific code the following lists will appear automatically on the patient’s statement:
Explosion Codes D 1110: Prophy u. Ultrasonic fine scale & polish u. Infection control u. Oral hygiene aids u. Complete periodontal evaluation u. Oral Cancer/Head & Neck Exam u. Oral hygiene instructions
Explosion Codes D 4341: Root Debridement u. Anesthesia as needed u. Ultrasonic periodontal scale u. Infection control u. Root debridement u. Antimicrobial irrigation u. Disclosing/oral hygiene instructions/aids
Explosion Codes D 4910: Supportive Periodontal Treatment u. Complete periodontal evaluation u. Isolated root debridement u. Ultrasonic periodontal scaling u. Oral cancer/head and neck exam u. Disclosing/oral hygiene instructions u. Fine scale and polish u. Anesthesia as needed u. Antimicrobial irrigation u. Infection control u. Oral hygiene aids
Explosion Codes D 4999: Definitive Therapy u. Complete periodontal evaluation u. Isolated root debridement u. Ultrasonic periodontal scaling u. Oral cancer/head and neck exam u. Disclosing/oral hygiene instructions u. Fine scale and polish u. Anesthesia as needed u. Antimicrobial irrigation u. Infection control u. Oral hygiene aids
Explosion Codes If your system allows less lines than you need you can adjust for that by adding a continuation of the code, and can add more descriptions. You would have a RDT with possibly 6 descriptions and then have an RDT 2 to fit in the remaining descriptions. You would need to enter two codes to fit in all your descriptions. You may need to decide what you feel are the most important procedures during each appointment and keep those while deleting the rest.
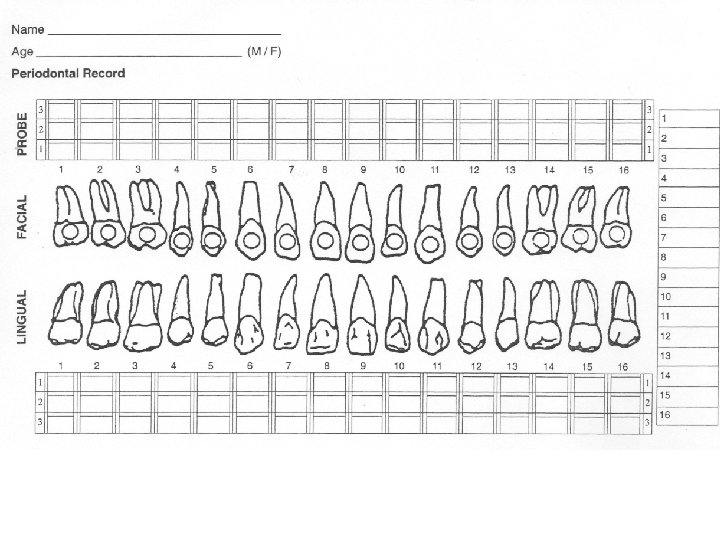
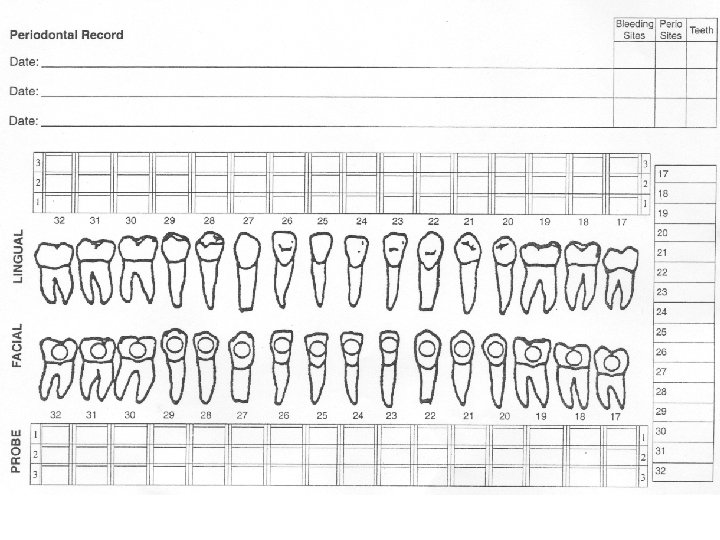
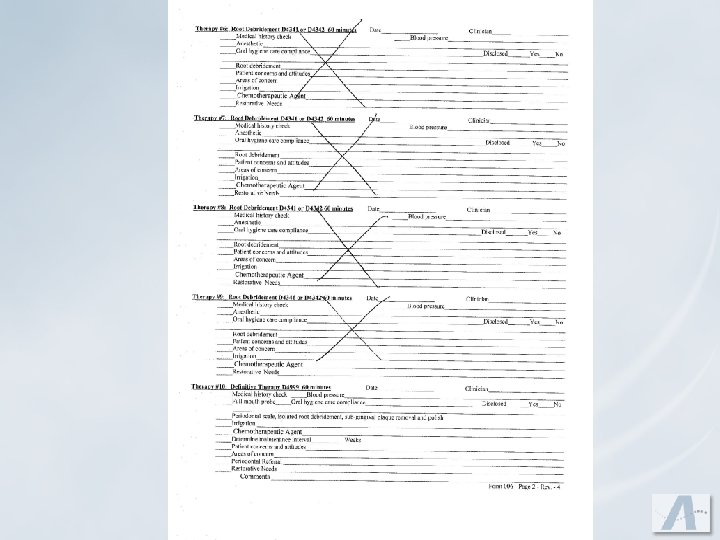
You Must Diagnose the Disease and Inform the Patient We feel a check list chart system is good and have samples for you to look over and use. A check list chart enables you to systematically go through your exams and leaves less room for error or oversights.
You Must Diagnose the Disease and Inform the Patient Entries should be: u Written in ink u Dated u Legible u Permanent u Signed u No alterations – If a mistake is made, draw a line through it. No liquid paper should be used. u Abbreviations are acceptable. There should be a master list of abbreviations for your office. u It is recommended to have a separate area where fees are recorded for the procedures.
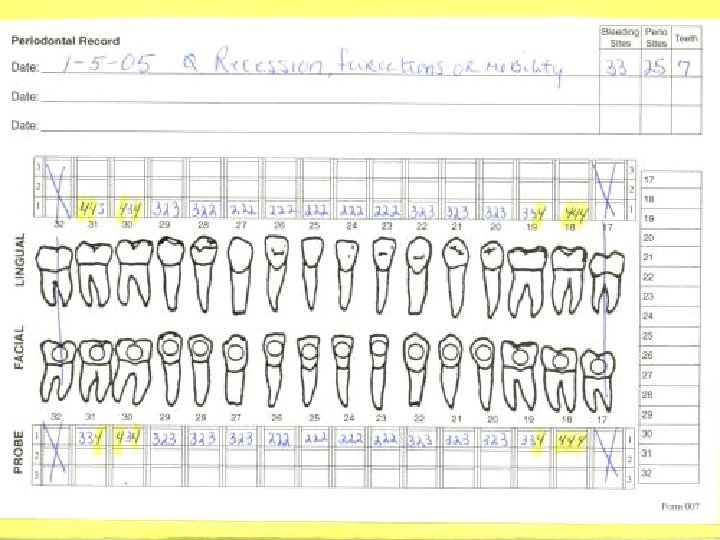
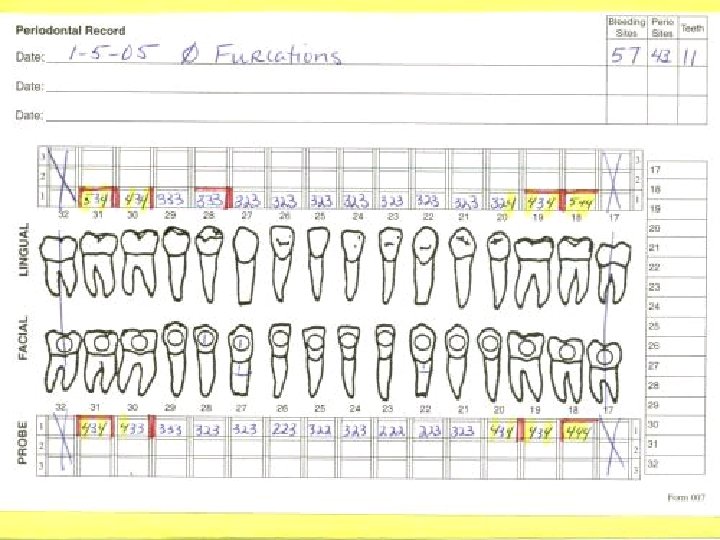
All Charts Should Include the Following 1. Current medical history and age of 7. Assessment of etiologic factors – patient i. e. , Dilantin 2. Blood pressure check 8. Assessment of accretions present 3. Oral cancer check 9. Assessment of gingival inflammation 4. Full periodontal pocket charting 10. Assessment of damage to periodontal structures 5. Recession, mobility and furcations noted as well as overhang fillings, rotated teeth, signs of occlusal trauma and sensitive teeth 11. Patient’s compliance and motivation 6. Appropriate x-rays 12. Treatment recommended; risks and alternatives
Sample of Chart Entries Example #1 u. Patient accepts treatment: Date + Case Type + Procedure + Provider (always after date) 2 -12 -17 - CT II – IT + 4 BW _____EAG 2 -14 -17 - CT II – 14 PA’s + RDT 1/3_____EAG 2 -21 -17 -CT II- RDT 2/3_______EAG 3 -31 -17 – CT II - DT 3/3_______EAG 6 -15 -17 - CT II - SPT_______ EAG
Sample of Chart Entries Example #2 u. Patient does NOT accept treatment: 4 -11 -17 - CT II-Pro + 4 BW. Pt. Did not accept treatment due to $. Pt. Understands the risks of non-treatment. _______EAG
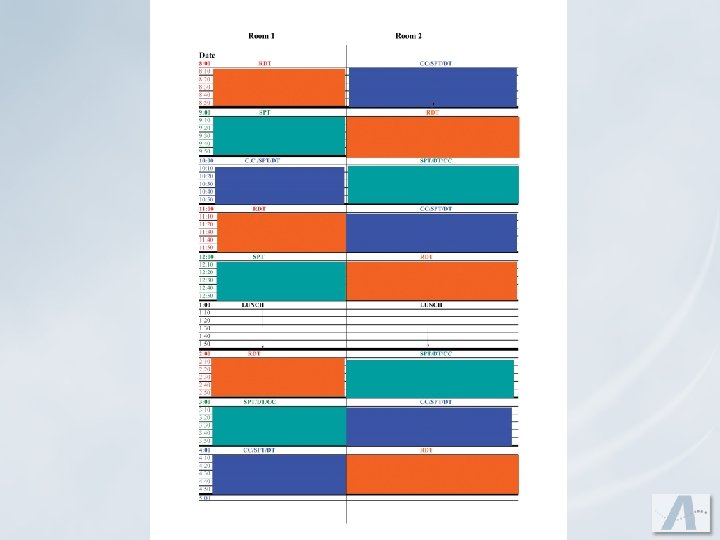
Effective Hygiene Scheduling It needs to be planned if you ever want to experience an effective productive schedule.
Effective Hygiene Scheduling u. Mix of procedures u. Daily Goal u. With multiple hygienists doctor exams need to be planned u. Appointments requiring periodontal chartings should not be planned at the same time u. Root debridements, Supportive periodontal treatment or Definitive therapies should be scheduled before lunch or at the end of the day.
Setting up the Day Requires: u 10 minute interval appointment u. A master “Ideal Day”
Phrases to Avoid! u“What time would you prefer? ” u“Would you like morning or afternoon? ” u“Is there a certain day or time that works better for you? ”
Cancellations!
Openings in Hygiene = Lost $ u. Cost of one opening in one hygiene schedule per day at the end of one year for your practice is: $_____
Types of Summaries u. Hygienist/Patient u. Hygienist/Doctor u. Doctor/Patient u. Hygienist/Financial Coordinator u. Hygienist/Scheduling Coordinator (SPT or Prophy) u. Financial Coordinator/Scheduling Coordinator u. Scheduling Coordinator/Patient
The Patient is on the Phone Wanting to Cancel u“Oh Dear” u. Pull Chart u. Find Ammunition u. W. I. I. F. T. (What’s In It For Them) u. Doctor and Hygienist Concerned u. Infection
Prevention u. What does your appointment card say? “We require two business days notice. ” u. Courtesy call 2 -3 days in advance u. Check-out Dialogue u. Answering Machine/Voice mail
When You Can’t Prevent the Cancellation u. Document
Two Types of Patients That Fail u. The patient who has never failed before and never will again, they are very apologetic u. The patient who would not get on a bus if you sent it for them, and could care less that they’ve missed an appointment
What To Do With Patients That Fail u. Don’t give the patient another block of reserved time unless they pre-pay! u. Place on a Priority Call List u. Invite them to call on a day that they feel that they can keep an appointment, if you have an opening they are welcome to it
What To Do With Patients That Fail Charge? You have to charge enough!!
Tomorrow, Day After Tomorrow Next Weeks Patients!!!! u. You never have a chance to recover that opening once it is gone u. Patients are always prepared for the possibility of change u. They are mentally ready for a dental appointment
Priority Call List u. Patients who require a particular time, are already scheduled, but interested in an earlier date u. Patients who have failed an appointment and are no longer offered a prescheduled appointment
Thoughts on Communication u 80% Listening +20% Talking 100% Effective Communicator u. Ask questions to facilitate communication u. Explain periodontal information clearly and in proper terms u. Patients are coming to you for guidance u. Communication is more than words u. Are you excited about the variety of services you can offer patients in your office?
Questions to Consider u. How would you feel if a doctor called you with the news that you had a “little problem”? u. What happens when people get overwhelmed? u. Do people change before they are ready to change?
Important Points for Explanation of Periodontal Disease u. Tell Patient what you are going to do and why: v. Introduce assistant v. Taking some measurements v. Looking for signs of periodontal disease v. Takes a few minutes v. Explain everything when done u. Case Type
Case Type u. Healthy – No readings over 3 MM and under ____ bleeding sites. u. Gingivitis – No readings over 3 MM and more than ____ bleeding sites v. Mild – No tissue change v. Moderate – Tissue change
Case Type u. Early Periodontal Disease – 4 MM pockets: v. Borderline – 1 to 3 isolated sites v. Beginning – in molars only v. Early – moving to anterior. Could also have a couple of isolated 5 MM
Case Type u. Moderate Periodontal Disease – 5 MM pockets with a possible couple of isolated 6 MM u. Advanced Periodontal Disease – 6 MM pockets and above
Important Points for Explanation of Periodontal Disease u. Treatment plan: v. Total the number of teeth with 4 MM pockets and greater then divide by 2 or 3 for laser practices or 3 or 4 for general practices u. Show Healthy: v. Show probe and show what it is v. Explain Health w Sulcus w 1, 2, and 3 MM readings w No bleeding
Important Points for Explanation of Periodontal Disease u. STOP and wait for a response u. Show Disease: v. Pockets measuring 4 MM or more v. Bleeding v. Tender to probe
Important Points for Explanation of Periodontal Disease u“We treat periodontal disease with a procedure called root debridement therapy. FOR YOU… v. Number of hours of therapy v. Each appointment approximately 1 hour long v. Not surgery v. Divide mouth into sections v. Numb for comfort v. Explain detoxification v. Expected results
Doctor’s Role u. Social graces with the patient u. Ask the hygienist what the findings were u. Diagnose disease u. Approval of patient’s decision u. Do restorative exam
Doctor’s Role u. Be certain to say your “line”: v. You will be scheduling a series of appointments before you leave today. It is very important that you keep these appointments as they are scheduled for the best success of your treatment
Hygienist’s Role u. Complete periodontal charting u. Bring patient into their own mouth by showing health versus disease u. Tell patient their level of disease and treatment recommendations u. Emphasize the importance of keeping appointments as scheduled for the success of their treatment
Hygienist’s Role u. Emphasize the importance of the most important appointment – the definitive therapy u. Make sure patient understands the nature of periodontal disease as chronic, site specific, and episodic u. Answer any questions the patient may have u. Summarize and hand-off to Doctor
Hygienist’s Role u. Summarize when you are done with today’s appointment v. I know we gave you a lot of information today… v. Pamphlets or handouts v. Business card u. Walk patient to the front and summarize and hand-off to the front office personnel
Supportive Periodontal Treatment Summary and Hand -offs u. Hygiene/Doctor Summary and Hand-off: v. How is interval working v. What you did today v. Recommendation for keeping or modifying supportive periodontal interval u. Doctor/Patient Summary: v. Confirm if interval is working (or not) v. Reinforce
Supportive Periodontal Treatment Summary and Hand -offs u. Hygienist/Patient Closing Summary: v. Let patient know that you or the scheduling coordinator will be reserving a 12 week interval appointment for their supportive periodontal treatment v. We were pleased with the results today v. Clarify and questions
Supportive Periodontal Treatment Summary and Hand -offs u. Hygienists/Scheduling Coordinator at Front: v. Sue will need to reserve time for her 12 -week supportive periodontal treatment. It was great seeing you today, Sue and I am really happy that this 12 -week interval is working well for you.
“Coming together is a beginning. Keeping together is progress. Working together is success. ” Henry Ford