Single Complete Denture Niaz Ahammed A Contents Introduction













 The maxillary and mandibular cast are mounted on articulator using provisional")
 Method involves the use of a metal U-shaped occlusal template which")








 Suggested using compound maxillary rim for functionally generated chew-in technique. The compound")

 • Preliminary impressions and base – Upper and")




 Appointment I: Appointment II: • Impressions")


 Ø Mentions a simple technique of using maxillary rim of softened wax. Ø")







")













Porcelain teeth: 1. Wear slowly and vertical dimension of")
 Acrylic resin with amalgam stops: • Amalgam inserts reduce occlusal wear • Less")
 IPN Resin: 1. Consists of unfilled, highly cross-linked, interpenetrating polymer network. 2. Wear")



 loss of bone")
 papillary hyperplasia in the hard palate, (4) extrusion of the lower anterior teeth,")









- Slides: 75
Single Complete Denture Niaz Ahammed A
Contents • Introduction • Problems in single complete denture • Diagnosis and treatment planning -mouth preperations -occlusal adjustments • Modifying occlusal pattern – Swenson’s method – Yurkstas – Bruce method – Boucher’s method
• Achieving harmonious balance – Functional chew in – Articulator equilibriation • Mandibular denture opposing natural maxillary teeth • Maxillary denture opposing RPD • Maxillary denture opposing FPD • Maxillary denture opposing CD • Clinical procedures • Occlusal materials • Sequelae of single dentures • Combination syndrome
Introduction
A single complete denture can oppose any one of the following: 1. Natural teeth that are sufficient in number not to necessitate a fixed or removable partial denture. 2. A partially edentulous arch in which the missing teeth have been or will be replaced by a fixed partial denture. 3. A partially edentulous arch in which the missing teeth have been or will be replaced by a removable partial 4. An existing complete denture.
Problems in single complete denture • High magnitude of forces that natural teeth can exert on denture base • Occlusal form of denture base-over eruption or tilting and high or sharp cusps
Diagnosis and treatment planning • Primary objective is to preserve the remaining structures • Factors to be considered are: -Acceptable interocclusal records -Stable jaw relationship with bilateral posterior teeth contacts -Forces directed along the long axis of the teeth -Avoidance of adverse tooth contacts Prosthetic treatment for edentulous patients; Zarb , 13 thedition
Mouth preperation: • Arch form in dentate jaw may not co ordinate with the arrangement of denture teeth • The remaining teeth may be tilted or supra erupted • The natural teeth can be ground or restored to give a more suitable occluding surface and grossly malpositioned teeth can be extracted or orthodontically repositioned
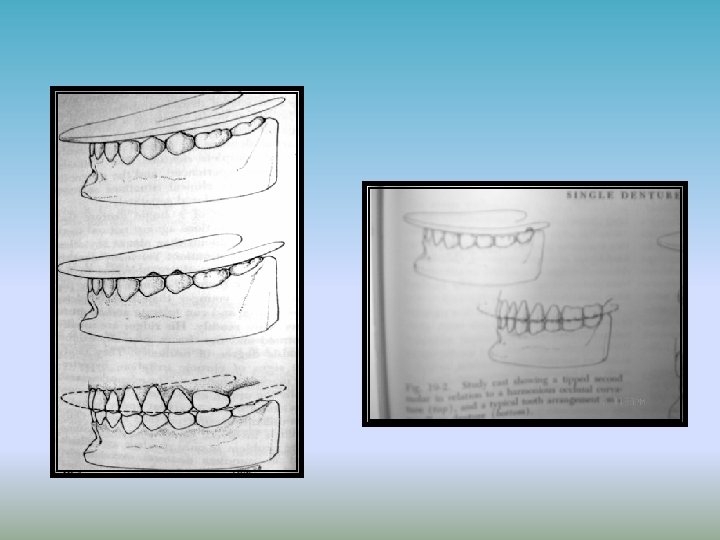
Occlusal adjustments • Natural lower cuspids and incisors are long and often has to be ground • Severely tilted and overerupted molars should be considered for extraction • If tilt is not extreme, distal half of occlusal surface is ground flat and denture made to contact with that area only
• Ideal treatment is to restore the tooth with cast gold crown or onlay • If there is a large edentulous space mesial to the molar, a bridge or removable denture should be inserted
Carl F. Driscoll and Radi M. Masri* proposed a classification system that could simplify the identification and treatment of single denture patients Class I - Patient for whom minor or no tooth reduction is all that is needed to obtain balance. Class II – Patient for whom minor additions to the height of the teeth are needed to obtain balance. Class III – Patient for whom both reduction and additions to the teeth are required to obtain balance. The treatment of these patient involves change in the vertical dimension of occlusion. Class IV – Patient who presents with occlusal discrepancies that require addition to the width of the occluding surface. Class V – Patient who presents with combination syndrome. *DCNA, July 2004: Vol 48; No. 3
Modifying Occlusal Pattern
• Several techniques to modify the existing occlusal pattern prior to denture construction have been suggested: q Swenson’s technique q Yurkstas method q Bruce method q Boucher method q Han Kuang Tan’s technique
Swenson’s method (1964) The maxillary and mandibular cast are mounted on articulator using provisional centric record. A maxillary denture teeth are set. Lower interfering teeth are adjusted on the cast and area is marked with a pencil. The natural teeth are modified using marked diagnostic cast as a guide. After the occlusal modifications new impressions are made of the lower arch and mounted on the articulator. The artificial teeth are then checked and modifications done for the final try in. Complete denture prosthodontics: Sharry, 315
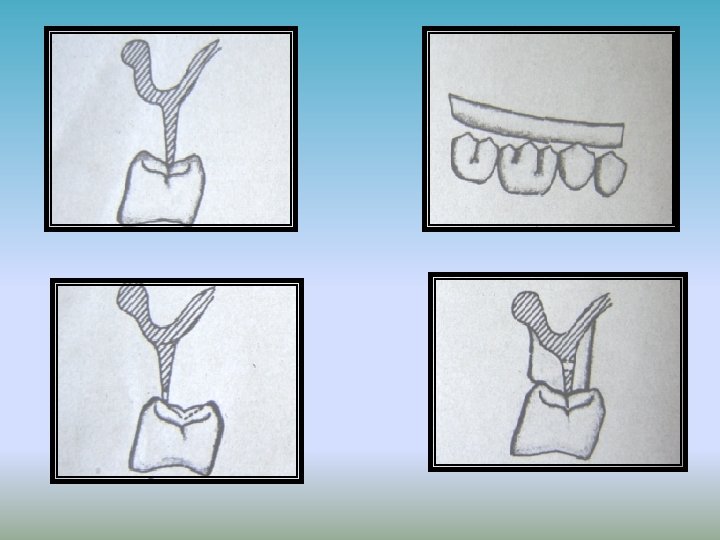
Yurkstas method (1968) Method involves the use of a metal U-shaped occlusal template which is slightly convex on the lower side. The template is placed on the lower cast and the cusps to be adjusted are identified. *DCNA, July 2004: Vol 48; No. 3 The stone cast is modified to an acceptable occlusal relationship and the areas are marked with a pencil. This cast is then used as a guide to modify natural teeth
Bruce method ØThe casts are mounted and the necessary modifications are made on the stone cast. ØA clear acrylic resin template is fabricated on the modified stone cast. ØThe inner surface of template is coated with pressure indicating paste and the interferences are noted through template. ØThe desired modifications are done till the template seats properly. Complete dentures opposing natural teeth: Bruce etal: JPD, November 1971
Boucher’s method His technique involves making the natural teeth fit to the established plane and inclines of the maxillary porcelain teeth. First, the cast are mounted and the artificial teeth are arranged to the best possible balancing contacts. If the natural teeth prevent balancing, the interferences are removed by movement of maxillary porcelain teeth over the mandibular stone teeth. The denture is processed and area to be reshaped are noted on the cast. The natural teeth are ground at the areas marked on the cast. The occlusion is refined in the right and left lateral excursive movements until a harmonious balance is achieved.
Han-Kuang Tan Make a vacuum formed clear template over the cast with Sta -Vac sheet 0. 02 inch thick The casts are mounted on the articulator and the maxillary teeth are arranged. Judicious grinding of the denture teeth and the natural stone teeth on the cast should be carried out. The modified cusps are marked and the template is re-seated. Voids are seen at the prepared areas. The template is cut over the prepared areas which will create openings in the prepared areas when it is seated in the patients mouth. The natural teeth are reduced using this a guide. A preparation guide for modifying the mandibular teeth before making a maxillary single complete denture Han- Kuang- Tang, JPD, 1997
Achieving Harmonious Occlusal Balance
The various techniques fall in two categories Those which dynamically equilibrate occlusion using a Functionally Generated Path Those which statistically equilibrate occlusion using a Articulator programmed to simulate patients jaw movements.
Functionally Generated Chew-in Technique These techniques to provide the most accurate method of recording occlusal pattern. However, Contraindications: – The desired jaw movements and necessary record base stability are not possible – The denture space is inadequate. – Physical and mental condition of the patient seriously compromise effective cooperation.
Stansbury (1951) Suggested using compound maxillary rim for functionally generated chew-in technique. The compound maxillary rim trimmed buccally and lingually Carding wax is added to the rim. The patient is asked to do eccentric chewing movements. Single denture construction against non-modified natural dentition: JPD, November, 1951 The carding wax gets molded to the functional movements and while compound in the central fossa prevents the loss in vertical dimension.
The stone is vibrated into the wax path of the cusps to make a stone cusp path record and chewing cast The denture teeth are first arranged according to the lower cast. After try-in is approved lower cast is removed and the lower chewing cast is secured to the articulator. All interfering spots are carefully grounded. Thus maximum bilateral balanced occlusion will be achieved.
Vig’s technique (Robert G. Vig 1961) • Preliminary impressions and base – Upper and lower impressions are made, casts poured and denture base fabricated with cold cure resin. • Registration and mounting – Centric relation at acceptable vertical dimension recorded – Anterior teeth are arranged • Preparing the chewing apparatus: – The wax occlusion rim posterior to cuspid is removed. – Resin in dough stage is placed on denture base and the articulator is closed to press the resin against the occlusal surface. – When set, the resin is trimmed so as to leave only a fin of resin in contact with the central grooves of lower posterior teeth. Modified chew in tech- RG Vigg, JPD, April 1964
• Cusp and Sulcus analysis: Ø The patient is directed to make a lateral excursions to bring tips of the mandibular cusps in contact with the fin Ø If most of the teeth do not contact the fin on lateral excursions then the teeth in contact must be ground until an equal contacts occurs between the teeth and plastic. Ø If most of the buccal cusps contacts the maxillary fin, but few do not, the fin must be lengthened by deepening the central fossae of teeth and building the fin with cold cure resin. Ø Even contacts are achieved on both sides of arch. Ø Holes about 1/4 th inch apart are drilled and filled with sticky wax. Ø The fin is then built up with wax according to the width of the opposing tooth.
• Functional impression and Chew-in q Tissue conditioning resin is added to the impression side and base is seated in the mouth. q After ½ hour patient is given thin slice of fruits like banana and asked to chew normal pattern followed by vigorous chewing. q The chewing pattern and impression surface are examined. ü If few areas expose : the resin is trimmed and relined ü If borders are exposed : resin is trimmed and relined ü If border unsupported : build with resin and reline q The wax on the occlusal surface is rebuilt and the base is inserted in patients mouth with instructions not to consume solid or hot foods and to wear base all night.
• Forming the stone chew-in record – Master cast poured without boxing – Record is obtained for the waxed chew in – The cast, record base, chew-in record and counter cast are mounted on the articulator • Arranging the posterior teeth – The teeth are arranged according to the occlusal scheme of the mandibular teeth and all the interferences in the lateral excursive movements are removed with the help of the chewin record.
• Rationale of the technique – Creates cuspal harmony in the non-functional glides – Patients with limited motion, unusual patterns of masticatory movements, persistent bruxism and other atypical situations can be accommodated Contraindicated if the mucosa is so resilient that it can allow shifting of the record base during the chew-in phase.
Kenneth D. Rudd and Robert M. Morrow (1973) Appointment I: Appointment II: • Impressions are made • Two resin base plates are constructed on the maxillary cast • A tentative jaw relation record. • Denture teeth are selected and positioned with the patient present, the setup is completed for try-in. • The duplicate denture base plate is placed on the cast and the modelling plastic is warmed and the articulator is closed. The posterior quadrant of the occlusal rim are trimmed. • With the modelling plastic in occlusion position, a divider is used to make vertical dimension reference measurement Occlusion and single denture; Rudd , Morrow; JPD July, 1973
Appointmen t III • The waxed denture is inserted and subjected to the usual check. • Recording wax for the functionally generated path procedure is added to the occlusion rim. • The patient is asked to do mandibular movements.
Stone core: • The generated wax path is carefully boxed and stone is poured. • The upper denture teeth are set or ground to fit the generated path as recorded in the stone core.
Sharry(1968) Ø Mentions a simple technique of using maxillary rim of softened wax. Ø Lateral protrusive chewing movements are made so that the wax is abraded. Ø Generating functional path of the lower cusps. Ø This is continued until the correct vertical dimension has been established. Complete Denture Prosthodontics; Sharry 317
Articulator Equilibration Technique Indications: v The denture base lacks stability. v If the patient is physically unable to form a chew-in record. Essentials of complete denture prosthodontics 2 nd ed, Sheldon Winkler, 421 -24
Upper cast is mounted on articulator using face bow. Lower cast is related using interocclusal record. Buccal lingual position of lower teeth and their relation to the upper arch is studied and decision is taken whether to articulate the denture teeth with lower buccal cusps or the lingual cusps. Once the holding cusp have been selected the inclines of remaining cusps are reduced.
The selection of the holding cusps depends according to the lower occlusal scheme
At the time of wax try-in eccentric records are made and set on the articulator. The upper posterior teeth are arranged as close to being balanced as possible at this time. The denture is processed and again related to the articulator. Eccentric balance is achieved by grinding the interfering buccal and lingual inclines of upper teeth. If any lower cusp make contacts other than holding cusp the interferences are removed.
• Mandibular Denture to Oppose Natural Maxillary Teeth: ü Seldom this condition does occur. ü It usually happens as a result of surgical or accidental trauma. ü An example of surgical trauma is the removal of the mandibular teeth for persons who have to undergo irradiation therapy for a tumor.
Complicating factors for the single mandibular complete denture opposing natural teeth 1. The denture supporting tissues for the mandibular complete denture is relatively small compared to the maxillary supporting tissue. 2. The mucosa with tightly attached submucosa overlying the periostium and bone of the lower residual ridge is thin. 3. For the above two reasons, the underlying bone is extremely prone to resorption from occlusal forces of the natural teeth. 4. Impact of occlusal forces from moving mandible Heartwell; syllabus of complete dentures, 488 -89; Zarb; 12 th edition
There are two situations When a mandibular complete denture, opposing upper natural teeth are accepted: 1. When the patient has a class III jaw relationship. This occur when the mandible is larger than normal or the maxilla is smaller than normal. 2. When the patient has a cleft palate,
Eugene tilman; removable partial upper and lower complete dentures ( jpd, nov- dec, 1961) • A posterior occlusion employing nonanatomic teeth aids in the stability and reduces the displacing forces encountered in mandibular movements during mastication. • The lower anterior teeth must be arranged for esthetic appearance • A plane of occlusion is constructed on the lower base beginning at the height of the cusp of the lower cuspid and extending distally parallel with the crest of the lower ridge
Single Complete Maxillary Denture to Oppose Natural Mandibular Teeth The diagnostic procedures should determine that; i. there are sufficient teeth in the mandibular arch, ii. periodontal health is acceptable, and iii. there are no missing teeth to be replaced. Syllabus of complete Dentures; Heartwell, pg- 490 -92
Some times the positions of the mandibular anterior teeth will not allow the maxillary anterior teeth to be positioned in an esthetically acceptable manner or for balanced occlusion. This problem may be resolved as follows: 1. Reposition the natural teeth with orthodontic procedures. 2. Alter the clinical crowns of the teeth by grinding or with restorations. 3. Accept balanced occlusion with the jaws in centric relation and not in the eccentric positions.
• The occlusal forms of the natural teeth usually act as the guide in selecting the occlusal form for the maxillary posterior teeth. • In most situations this would be a cusp tooth • But if the natural teeth are abraded and are not restored prior to treatment, the monoplane form may be the choice for the occlusal surfaces of posterior teeth. • When the mandibular teeth are malposed or missing, selective grinding procedures can be employed • When occlusal surfaces have large food tables , they can be altered by removing some enamel from buccal and lingual surfaces
Single Complete Maxillary Denture to Opposing Natural Mandibular Teeth with fixed prosthesis • Once a fixed restoration is placed in a dental arch, the restored arch can be thought of as natural teeth opposing a complete denture. • The construction and placement of fixed restorations can correct many occlusal disharmonies that existed previously • The occlusion between the denture teeth and the fixed restorations is harmonized on an articulator Single complete dentures; Ellinger. JPD; Nov, 1951
Complete maxillary denture to oppose a partially edentulous arch and a removable partial denture ü The most frequently encountered situation for a single complete denture ü Replacement of missing posterior teeth in lower arch will improve the prognosis of upper denture ü But in class II jaw relation, lower anterior teeth and premolars is enough Single complete dentures; Ellinger. JPD; Nov, 1951
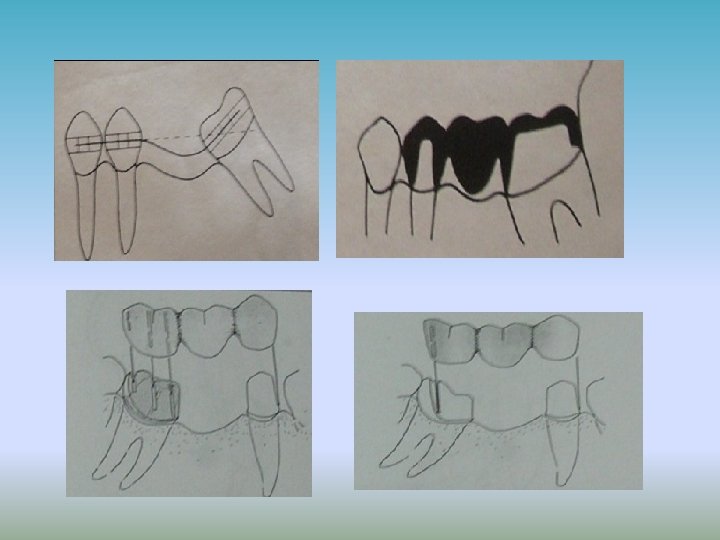
• A complete upper denture should not be constructed to oppose only 6 -8 lower natural anteriors, unless replaced by RPD • If not loss of bone and formation of hyperplastic tissue can form in anterior maxilla • Lower RPD is usually indicated when all molars are missing • If all teeth through the first molars are present RPD may not be indicated • If all teeth through premolars on one side and molars on other side are present, RPD may not be necessary • In some cases missing molars may be restored with cantilever type of FPD
Clinical procedures for making complete upper denture opposing natural or fixed restoration- Ellinger etal- JPD, July, 1971 • Make Impression of lower arch of irreversible hydrocolloid and pour artificial stone • Make Preliminary upper impression and final impressions of upper arch made and pour the cast • Construct occlusion rim and contour it for adequate lip support • Use face bow and mount maxillary cast on articulator • Establish the VDO
• Make preliminary centric relation record • Select artificial teeth and arrange them in centric occlusion • Make eccentric records and transfer it on to the articulator • Rearrange posterior teeth to obtain balanced occlusion
• Alter occlusal surfaces of teeth on stone cast to provide balanced occlusion and outlined • After the teeth are recontoured, make preperations for restorations that are planned for fixed or removable prosthesis • An impression is made and mount cast on articulator , and carve the wax patterns to the existing occlusion of denture teeth
• Place restoration in mouth and make final impression • Make a new centric relation record and remount the lower cast • Teeth are arranged in the most nearly ideal balanced occlusion • Perfectly balanced occlusion in all eccentric positions may not be possible for every patient when working with natural teeth
Single Complete Denture to Oppose an Existing Complete Denture • The existing denture should be satisfactory if it is used for fabrication of single complete dentures ü ü The teeth should be Aligned with respect to residual alveolar ridge for mechanical stability and masticatory efficiency Have good appearance Exhibit proper tissue support Have cusp height suitable for the teeth of planned denture Single complete dentures; Ellinger. JPD; Nov, 1951
The denture base should q Have esthetic contour and thickness to support peri oral structures q Be extended to utilize all available supporting tissues q Be stable and retentive Unfortunately, few dentures fulfill all these criteria and in such cases the prognosis is poor
OCCLUSAL MATERIALS FOR SINGLE DENTURES • Artificial Tooth Material ü Plastic ü Porcelain ü Metal Ø Amalgam Ø Cast gold occlusals
OCCLUSAL MATERIALS FOR SINGLE DENTURES 1)Porcelain teeth: 1. Wear slowly and vertical dimension of occlusion is maintained. 2. Cause fracture and chipping when opposed to natural teeth and are difficult to equilibrate. 3. Cause wear of natural teeth 2) Acrylic resin teeth : 1. Easy to equilibrate and cause no wear of natural teeth 2. Disadvantages: These teeth wear after a period of time and cause loss in vertical dimension.
3) Acrylic resin with amalgam stops: • Amalgam inserts reduce occlusal wear • Less expensive and time consuming Technique: After the acrylic teeth have been balanced, occlusal preparations are made in the acrylic teeth, extending to include as much of the articulating paper tracing as possible. Amalgam is condensed into these preparations and articulator is gently closed, going side to side, back and forth until the incisal guide plane is again flush with the guide pin. Articulator generated amalgam stops for cd, Lauciello, JPD, 1979
4) IPN Resin: 1. Consists of unfilled, highly cross-linked, interpenetrating polymer network. 2. Wear is significantly less as compared to acrylic resin. 5) Gold occlusals: 1. These are considered one of the best materials to oppose natural teeth though it is an expensive and a time consuming process. 2. When one or more gold occlusal surfaces are provided on either side of the single complete denture, they will stop the abrasion between unlike materials and protect the other teeth from wear.
Use of gold occlusal surfaces in complete and partial dentures-Wallace DH; JPD, 1964 • The denture is processed with acrylic resin teeth and all occlusal adjustments are made • Occlusal index or counter die is made of the denture teeth • The occlusal surface of the posterior denture teeth is reduced by 1 mm • Occlusal index is used to make a wax pattern with inlay wax • The wax patterns are cast and then cemented with selfcure acrylic resin
Two most common adverse sequelae include Natural tooth wear Use of porcelain teeth can lead to rapid wear of opposing natural dentition. Best is to use acrylic resin denture teeth in conjunction with periodic examination Denture fracture Heavy anterior occlusal contact, deep labial freni notches and high occlusal forces due to strong mandibular elevator musculature Carefully planned occlusion, adequate denture base thickness are necessary to prevent fracture Still if the fracture potential is high, cast metal base is the best option Prosthodontic ttm for edentulous patients; Zarb, 12 th ed pg-432
Combination Syndrome According to GPT 8 • “the characteristic features that occur when an edentulous maxilla is opposed by natural mandibular anterior teeth, ü including loss of bone from the anterior portion of the maxillary ridge, ü overgrowth of the tuberosities, ü papillary hyperplasia of the hard palatal mucosa, ü extrusion of mandibular anterior teeth, and ü loss of alveolar bone and ridge height beneath the mandibular removable partial denture bases, Also called anterior” hyperfunction syndrome. ”
Five changes constitute a Combination syndrome These are quite characteristic. (1) loss of bone from the anterior part of the maxillary ridge, (2) overgrowth of the tuberosities, Changes caused by mandibular rpd opposing maxillary cd, Kelly E, JPD february,
(3) papillary hyperplasia in the hard palate, (4) extrusion of the lower anterior teeth, and (5) the loss of bone under the partial denture bases.
Saunders et al; stated that six other changes are commonly associated with this clinical scenario: ü Loss of vertical dimension of occlusion ü Occlusal plane discrepancy ü Anterior spatial repositioning of the mandible ü Poor adaptation of the prostheses ü Epulis fissuratum ü Adverse periodontal changes
Kelly's Hypothesis Bone resorption in the maxillary anterior region initiates the changes. bony resorption also occurs under the mandibular partial denture bases. The maxillary denture then moves up in the anterior region and down in the posterior region in function. Changes caused by mandibular rpd opposing maxillary cd, Kelly E, JPD february,
With the posterior palatal seal, a negative pressure is produced posterior to the fulcrum line. This negative pressure may account for the enlarged tuberosities and the papillary hyperplasia.
Changes caused by mandibular rpd opposing maxillary cd, Kelly E, JPD february,
PREVENTION OF THE COMBINATION SYNDROME ü Treatment planning should avoid the necessity for such a combination. ü Eliminate the combination of complete upper dentures opposing Class I lower partial dentures by retaining weak posterior teeth as abutments by means of endodontic and periodontic techniques. Combination syndrome, a treatment report : Schmitt, JPD, Nov, 1985
ü Endosseous endodontic implants ü Amputation of one lower molar root to preserve the other as an abutment ü An overlay denture on the lower ü Overlay dentures utilizing the lower tooth roots for stabilization provide a complete denture occlusion.
Saunders et al; recommended that the essential objective of treatment planning in these cases was “ To provide an occlusal scheme that could best discourage excessive occlusal pressures in the maxillary anterior region in both centric and eccentric occlusal contacts”.
Summary