Infections in the immunocompromised patient Inger Karin Lgreid



, important with numbers and")


 • Clinically")








")














:")






 in urine or biopsi")




 • Forekomst – alder og kjønn.")
 • Status pr. 21. 12. 2009 in")

 – capsules, recommended to all age groups. Reduced")
 des-10/jan-11: • Alv. utbrudd i England høst 2010 –")





 -- acyclovir (Zovirax) -- valacyclovir (Valtrex) •")

- Slides: 56
Infections in the immunocompromised patient. Inger Karin Lægreid Avd for nyresykdommer St. Olavs Hospital Desember 2011
Immunocompromised patients: • Organtransplanted – immunosuppressive medications • Cancerpatients – cytotoxic drugs + xray • Systemic illnesses – ex. Vasculitis, Lupus, RA - immunosuppressive medications + cytotoxic drugs • HIV pos / AIDS
Risk factors for infections • 1. High dosis of immunosuppressive medications - Because of treatment failure or rejection - Repeating treatments - Cumulative dosis • 2. Leucopenia - Induced by a. medications: - Most often cytotoxic drugs and - azathioprine(Imurel), mycophenalate (Cell Cept or Myfortic) - or b. virus: CMV
Mecanisme of defense • Granulocytes – ability to granulocytosis (BM), important with numbers and function • Cellulær immunity – remove intracellulære patogens and virusinfected cells – Cytotoxic effector cells and spes. T cells • Humoral immunity – remove extra-cellulare bacteria, B cells and Ag and plasmacells – Ab • Skin-barriere broken: wound, venflone, catheter – entry for bacteria og virus • Mucous membranes (mouth, GI tractus, urinary tract)
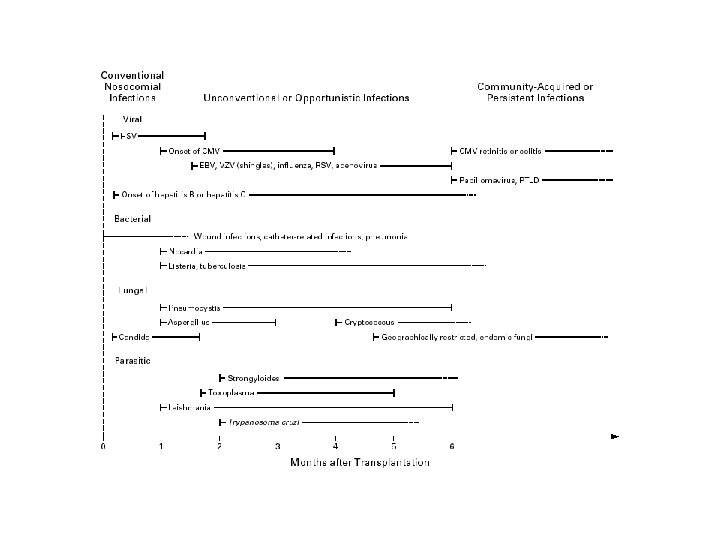
Types of agens • - Virus: Cytomegalo CMV Epstein Barr EBV Varicella zoster VZV Hepatitis. B HBV Hepatitis C HCV Herpesvirus HHV 6 -7 Polyomavirus Influenza A, pandemic • Bacteria: • Gram neg – Pseudomonas, E. coli, Klebsiella, enterobacti • Gram pos cocci – staf. cocci, streptococci - Legionella sp. - Listeria sp - Tbc
Cont. types of agens • • - Fungi: Candida Cryptococcus Mucor Aspergillus • Protozoer: • Pneumocystis jirovecii • Toxoplasmose sp. A
Causes of infection, fever and neutropenia • Fever without known cause (drugfever) • Clinically def. infection (- pos. culture) • Bacteremia (pos. blodkultur) • - Gram neg 10% – Gram pos cocci – Mixed – Polymicrobial 19% 1% 6% • Non bacteremia – – Gram neg Gram pos cocci Mixed Polymikrobial 39% 17% 35% 9% 2% 3% 1% 3% Am. cancerpopulasjon
Kasuistikk • • • Mann f. 1944 Ulcerøs colitt Nyretransplantert 2002 Sarkoidose Står på trippel immunsuppresjon: – Sandimmun, Cellsept og Prednisolon • Inntil det aktuelle: god almentilstand, kreatinin 160.
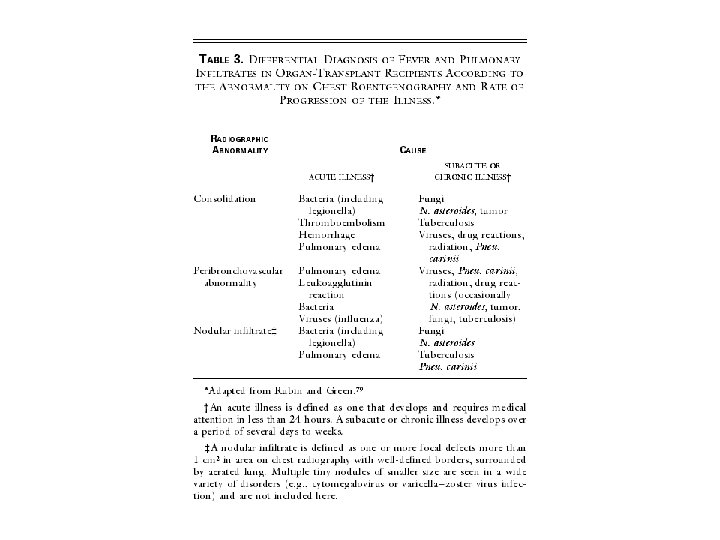
Kasuistikk • Feber, tørrhoste, slapphet frå 3. 12 • Opps fastlege , får Ciproxin • Ny kontakt pga ingen effekt/ forverring av symptomer → innlegges. • Ved innk 10. 12: feber, hoste, tungpust, CRP: 130, kreatinin 204 (e. GFR 28 ml/min) • Rtg. thoraks: småflekka infiltrat bilat, mest utbredt perihilært. Atypisk pneumoni? ? • Starter Rocephalin (cephalosporin)
Kasuistikk • Trass i Rocephalin – tilstanden forverres, økende dyspnoe, stigende CRP • Utifrå klinikk, CT thoraks og rtg. thorax funn – atypisk pneumoni: ? ? Pneumocystis Jirovecii • Planlagt bronkoskopi med BAL – pas for dårlig. • Starter Trim Sulfa (TMS) på mistanke, red dose pga nyresvikt • Forverring → Respirator • Bronkoskopi med BAL: Pneumoc J → høg dose TMS
Pneumocystis jirovecii pneumonia • Typisk røntgenfunn • Bilat hilusnære småflekka fortetninger
Kasuistikk • • • Uendra resp. status over fleire dager Terapisvikt pga initial låg TMS dose? Høg dose → økende nyresvikt + rhabdomyolyse Red TMS, må seponeres. 04. 01. 11: fortsatt på respirator, betring i nyrefunksjon (kreat 125), CRP 102, svært usikker prognose. • Får spontan pneumothorax – vanskelig å ventilere • Har ARDS, lungefibrose. • Avslutter respiratorbehandling 5. 1 –pas sovner inn samme dag
Pneumocystis jirovecii • Incidens hos organ tranplanterte: 5 – 15% • Reservoir: barn, symp og asympt immunkomprimerte pasienter • Luftsmitte via mennesker – opptrer ofte i ”cluster” • Riskofaktorer: alder, CMV infeksjoner, rejeksjoner, ↓ lymfocytter • Obs. coinfection (Herpesvirus)
Listeria monocytogenes • Listeria sepsis in adults nonpregnant: – Most are immunocompromised or elderly – Symptoms: fever and chills – Septic shock – Seeding of the brain and/or meninges – Meningoencephalitis or cerebritis – Diagnosis: culture of blood and cerebrospinal fluid (CSF) – Cerebral MRI
Listeria M • Listeria RH autum 2007: – Kantine serverte upasteurisert gårdsost – 15 persons got the disease – 5 died, 3 immunocompromised and 2 unborn childs(twins) • Eng. studie 10 års materiale (1999 – 2009): – Cancerpas har 5 X større risiko for Listeria M – Hematologisk cancer mest utsatt (17 x) – I tillegg til cancer: lever, nyresykdommer, bindevevssykdommer(Lupus) og inflammatoriske sykdommer (Crohns sykdom) Piers Mook et al; Em Inf Dis 2011 Jan
Listeria M • Treatment: – Ampicillin – Gentamycin ( in combination the first days) • Prognosis: – Total mortality: 25% – Higher by menigitis and sepsis
Legionella • Pneumonia – predominantly clinical manifestation • Cough – initially mild • Chest pain • High fever > 39 • Gastrointestinal symptoms • Headache
Legionella • Diagnosis: – Xray of lungs: patchy infiltrates – Culture of blood ( specific medium) – BAL – Direct immunfluorescens – Antigen- test in urine
Legionella • Treatment: –Erythromycin –In combination with ciprofloxacin or rifampicin • Prognosis: • Mortality: 5 – 30%
Cryptococcus • Disseminated fungi infection in liver transplanted patient • Six cutane lesions like this one • Biopsi and serum antigen test – cryptococcus • ”fleshy” border with centrale umbilication.
Invasive candidaisis • Tender, erythematøse nodulare lesions in neutropen pasient with leucemia after induction chemotherapy.
Aspergillus • Neutropen patient stamcelle treatment • Multiple necrotic lesions • Biopsi showed infarctions caused by Aspergillus
Herpes Zoster • 1. primær infeksjon: vannkopper • 2. Herpes Zoster – reaktivering av endogent latente varizella zoster virus i sensoriske ganglier – Følger dermatomer • 75% har prodromale smerter før utslettet • Starter ofte med små røde flekker → blemmer • Varizella zoster pneumonitt – alvorlig prognose
Herpes Zoster • Important with early diagnosis and treatment • Zovirax/ Valtrex early shortens the duration of the disease and reduces postherpetic pain • ”common” by organtransplanted (35% av BM tx)
Herpes Zoster • HIV pos. • Hemorrhagic vesicles • Pustles • = seint stadium • Obs. sekundær infeksjon
Herpes Zoster • Male b. 1960. Refugee from Vietnam • Cystic kidney disease, - renal transplanted april 98 • Rejection – Solumedrole + Thymoglobuline • Creatinine at discharge from RH july 98 : 320 • Aug -98: pain at left eye and ear. Opthalmoscopy: Shows vesicles, diagnosed as HZ optalmicus, gets general eyedrops.
Herpes Zoster II • 1 week later- hospitalizes with widespread Herpes Zoster Oftalmicus with affection of left part of the face incl. left ear • Zovirax (in reduced dosis because of reduced renal function) • Discharged from hospital after 2 weeks.
Herpes Zoster III • • 1 week later – new hosp : fever, dyspnoe og cough Blood tests: High CRP og leucopenia Xray lungs: diffuse infiltrate – agents? Broncoskopi with BAL: stafylococcus aureus + CMV Sepsis- multiorgan failure – respirator – dialysis Sep 2 of 3 immunosuppressive medications Survives with a rel. good outcome • status nov 2007: -- creat 130, chronic pain in left part of face, got perforation of tympanic membrane in -98, relapsing otitis later, planned operative treatment (myringoplastic surgery)
Herpes Zoster ophtalmicus • Rammer Trigeminus dermatom • Kan føre til corneal affeksjon og føre til synstap
Cytomegalovirus CMV • Member of B-herpes family • big ds DNA virus. Transmitted by : -contact (sexually, nursing) - blood / organ (CMV pos til CMV neg) - mother to child (in utero, perinatal, lactation) • Asymptomatic primary infection, followed by lifelong latency, can be reactivated • Age related increase in seroprevalence: - by age 20: - 40% -by age 30: - 50% -by age 50: - 65% -by age 80: - 90%
CMV • The most common viral infection in organ-transplanted • Lungs>heart>liver>pancreas>kidney ”CMV- syndrome” (viremi): - fever, malaise, ( ”influenza-symptoms”), leucopenia, trombocytopenia, hepatic aminotransferase elevations Tissue – invasive CMV: - GI – duodenitis, gastritis, colitis, ulcus - Lungs – pneumonitis - Transplantat – nephritis, hepatitis, pneumonitis - Eye - retinitis
CMV retinitis • CMV infenction in patient with AIDS • Retinitis with hemorhagies og papille-oedema • In the periphery– can be difficult to localise with ophtalmoscopi
Epstein Barr virus EBV • 20 -30% of organtransplanted has active replication of EBV • 80% of these have got antilymfocytt- antibodies (because of serious rejection). • Cyclosporine A (Sandimmun), tacrolimus (Prograf) + Antilymfocytt-antibodies reactivate latent EBV infection • EBV can give mononucleosis • Important: the role of EBV in the pathogenesis of development of post-tx lymfoproliferative disease.
EBV II • B celle lymfoproliferativ process – can change from benign polyclonale process to a highly malignant monoclonal lymphoma which is resistante to treatment. • Post-tx disease – extranodale – brain, bonemarrow, organtransplant, GI-tractus and liver • Important to reduce or take away immunsuppressive medications • Most important that the patient survives, on the behalf of the transplanted organ.
Epstein Barr virus Primary infection to chronic infection • EBV infect resting Bcells or epitelial cells • EBV-infected cells are kept in check by killercells and cytotoxic T-cells • Latente infected memory B cells (EBNA) can be reactivated and give chronic EBV infection
EBV lymfoproliferativ sjukdom • A. Cerebral MRImultiple tumornodules • B. Biopsi from perirenal tissue: immunoblastic lymfoma • C. EBV nuclear antigen - EBNA
Polyoma virus PV • Ds DNA virus, two types ass. with humane disease: • BK virus • JK virus • 60 -80% av immuncompetente adults are seropos for PV • Renal transplanted: --PV-BK can give acute tubulo-intestitiell nephritis, ureter stenosis, hemorragic cystitis, serious transplantat dysfunction --PV-JK reactivation can give progressive multifokal leukoencephalopati
Polyomavirus • Diagnosis: ---cells who contains virale inclutionsbodies (”decoy cells”) in urine or biopsi of the transplant • Treatment: ---- reduction in immunsuppression --- cidofovir – seldom in use, highly nephrotoksic
Polyoma-virus • Infecting many types of cells, including kidney, brain, liver, retina, lungs, blood, lymfatic, heart, muskulature og vasculare endoteliale cells • Virale particles binds to a spesific celle-surface reseptor and prod T antigen early in the infection cykel.
Genetic relationship among Human and Swine influenza viruses 1918 2009
The Two Mechanisms whereby Pandemic Influenza Originates. 1918 – H 1 N 1 virus closely related to avian virus adapted to replicate in humans 1957 and 1968, reassortment events led to new viruses that resulted in pandemic influenza. 1957 – Asian influenza 1968 – Hong Kong influenza Future pandemic strains could arise through either mechanism.
Influenza- virus
Infl. A H 1 N 1 (svineinfluensa) • Forekomst – alder og kjønn.
Influenza A (H 1 N 1= svineflu) • Status pr. 21. 12. 2009 in Norway: – 900 000 deceased persons – 1310 hospitalized – 170 intensive care • 71% < 30 years – 29 dead • 23 had other chronic diseases.
Vaccination – immunocomprimised patients • The use of immunosuppresive medication gives reduced effect of vaccination. • These patients is recommanded 2 vaccination with 4 weeks interval. • In periods with very high dosis of immunosuppresive medication (i. e just after renal tx, vaccination not recommanded, wait till 3 -6 months after tx) • Family members are recommanded vaccination
Treatment Influenza A • Oseltamivir (Tamiflu) – capsules, recommended to all age groups. Reduced dosis at e. GFR < 30, Not to dialysis patients (e. GFR< 10). • Zanavimir (Relenza) –aerosol, recommended to age groups > 5 years. No reduction in dosis with renal failure. Not recommended with serious lung disease.
Status A(H 1 N 1) des-10/jan-11: • Alv. utbrudd i England høst 2010 – Medio sept – medio des: 10 døde – Unge personer, fleste i risikogruppe – Medio des: 16 innl, fleste i intensivavd. • Sverige: gutt 7 år døde, risikogr. • Norge: 2 innl. ; lite barn + mann i 60 åra – Høg vaksinasjonsfrekvens i 2009/2010 – Mange hadde mild sjukdom, gir immunitet – Antar få m alv sjukdom i Norge denne vinter.
Diagnosis – infection in immunocomprimised patients? : • Anamnese: progress of the disease? fever? medication? Spesific symptoms? Pain? Cough? Abdominalia? Rash? • Clinical examination: all organs, spec. skin – wounds? incl. mouth, • Blood tests: Hb, trombocytes, leukocytes with cellcounting or only granulocytes, CRP, or SR renal function, liver function,
Cont. diagnosis • Urine stix + culture • Larynx • • Virus-serologi Bloodculture CBF - cerebrospinal fluid microscopy and culture Bronkoskopi – med lavage (BAL) Secrete from wounds Biopsi of affected organ. OBS! catheter – • Radiologic – chest, sinus, US, CT , MR • OBS: sikre diagnostiske prøver før start av antibiotika!!
Principles for antimicrobielle therapy • Treatment of established clinically disease • Prophylaxis – treat the entire patient-population prophylactic, fex all renal-transplant pat. get TMS as prophylaxis against Pneumocystis carini in 6 months post-tx • Preemptive therapy – treat subpopulations fex renaltx with pos CMV test, before clinically symptoms. • Obs. Studier må vise stor gevinst for å vege opp for risiko for resistensutvikling.
Anti-microbielle treatment Fever and neutropenia ( neutrophile < 0. 5 x 10 9 cells /L): (ex: nadirperiode etter tøffe cytostatika-kurer) • Big risk for lifethreathening infections, spec. gram. neg bacteria • Start with: benzylpenicillin + gentamicin • With clear abdominal symptoms: piperacillin/ tazobactam (Tazocin) • Dont hesitate – important with early start!!
Antifungal treatment • After 3 -5 days with neutropenia and fever –the risk for invasive mycosis is 25 -30% • The most common: candidasis • Treatment: fluconazol (Diflucan) • Suspicious for aspergillus and notflucanozol- sensitive candidasis: voriconazol (VFEND)
Antiviral treatment • Herpes simplex – valgancyclovir(Valcyte) -- acyclovir (Zovirax) -- valacyclovir (Valtrex) • CMV –gancyclovir ( Cymvene) – valgancyclovir • Herpes Zoster – acyclovir (Zovirax) • Diagnostikk: PCR- test in blood IF (immunofluorescens) Biopsi = gold standard
Conclusions • Immunocompromised pasients: – More vulnerable for infections – More often atypical infections, remember: virus, fungi, tbc – Can reacte different upon infections: • Less fever • Later signs on x-ray – Obs neutropenia – Obs medications • EARLY DIAGNOSIS and SPESIFIC TREATMENT is important for a good outcome!