APPROACH TO INFECTIONS IN IMMUNOCOMPROMISED HOST PRESENETED BY

APPROACH TO INFECTIONS IN IMMUNOCOMPROMISED HOST PRESENETED BY DR RAZZAQ

• CASE SCIENARIO • A 29 -year-old female patient, 2 years after kidney transplant, on mycophenolate, and prednisolone, presented with semiconsciousness, ulcerating lesions around right elbow, and oliguria for the past 6 h.

• Managing infection in an immunocompromised patient is a challenge to any ICU physician, as the presentation is varied and subtle and needs high index of suspicion for diagnosis and multiple possible etiologies. • A methodological approach to investigation and choice of empirical therapy is warranted in these patients.

• Step 1: Resuscitate • • If assisted respiration is required, initially non invasive ventillation should be tried. • • The patient should be closely monitored, and if no improvement or deterioration occurs in 2 h, invasive ventilation should be initiated. • Invasive catheters and lines should be avoided as these patients are coagulopathic and neutropenic and have a high risk of line sepsis. •

• Step 2: Take a focused history • • to determine the type and duration of the immunocompromised state Disease states such as hematological malignancy (leukemia and lymphoma), solid organ tumor, and conditions associated with neutropenic state should be looked for. • • History of any organ transplant and duration since transplant should be taken. • • HIV status should be determined, with proper consent. • • History of chemotherapy or radiotherapy should be taken. • • Detailed drug history should be elicited. • • Neurological, respiratory, gastrointestinal symptoms need to be elicited to narrow down differential diagnosis of opportunistic infection.

• Step 3: Perform physical examination • Any breach of skin or mucosal abrasion, skin ulcer, oral thrush, and perianal lesion should be searched for. • Look for skin rash. • All insertion sites of invasive lines should be inspected for tenderness or discharge. • All suture lines and drain sites should be inspected in postoperative patients after removing the dressing. • Look at the back for decubitus ulcer. • Do neurological, respiratory, and gastrointestinal system examination to determine organ system involvement

• Step 4: Send basic investigations • There is a broad differential diagnosis of opportunistic infection—bacterial, viral, or fungal— in immuno compromised patient These patients are also prone to infections which are common in non immuno compromised patients. • In these patients, infection mimics drug reaction, transfusion reaction, radiation induced complications, and disease-associated problems, which all need to be properly investigated. • Focused investigation, initially noninvasive and then invasive, should be performed to confirm the causative organism in order to narrow down anti-infective agents

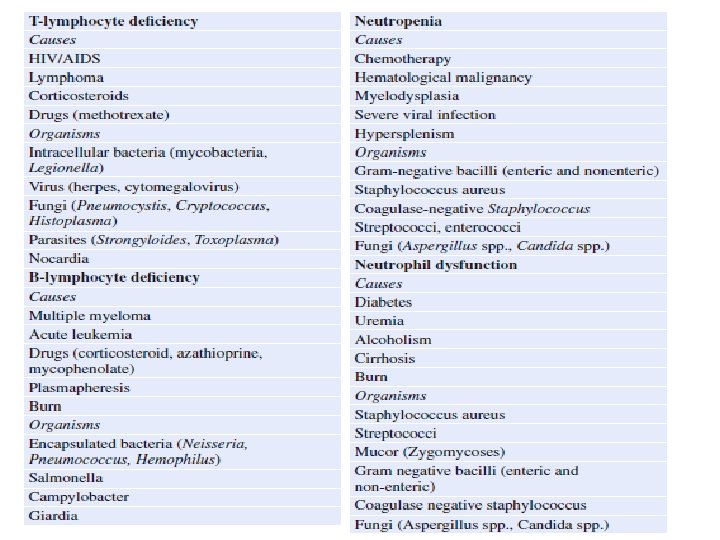
• Step 5: Identify underlying immune deficiency states and suspected pathogens • • Based on history, physical examination, and basic investigation, and immunodeficiency states needs to be recognized. • • Specific immunodeficiency states are associated with alteration of natural defense system (neutrophils, T cell, B cells). • • Patients with specific defense system alteration have propensity to be infected with certain groups of organisms, which need to be recognised

• Step 6: Initiate empirical anti-infective agents

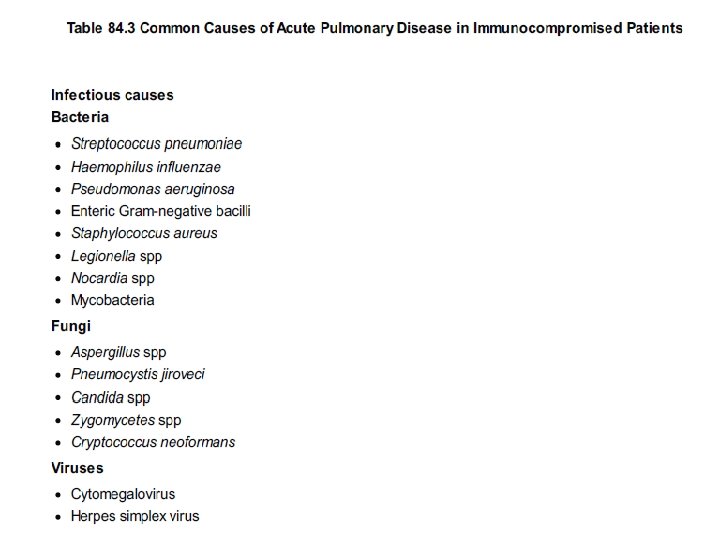
PNEUMONIA IN IMMUNO COMPRISED HOST • lung is one of the most common sites of infection in immunocompromised patients. • Pulmonary disease can be caused by a wide variety of agents, including bacteria, protozoa, helminths, viruses, fungi, and • mycobacteria • noninfectious pulmonary complications that can present abruptly with acute respiratory symptoms and fever. These • include underlying malignancy or vasculitis, drug toxicity, interstitial fibrosis, diffuse alveolar hemorrhage, radiation • pneumonitis, cardiogenic pulmonary edema, bronchiolitis obliterans organizing pneumonia (BOOP), diffuse alveolar • damage syndrome, acute fibrinous organizing pneumonia (AFOP), pulmonary alveolar proteinosis, and pulmonary • embolism

• Pneumonia in the immunocompromised patient often presents without the symptoms and signs seen in normal hosts. • Regardless of cause, fever and progressive shortness of breath ( tachypnea and arterial hypoxemia) • Chest radiographs should be obtained promptly in the compromised patient with fever or dyspnea. High-resolution CT or MRIs will often reveal infiltrates or masses that cannot • be appreciated on conventional X-rays.

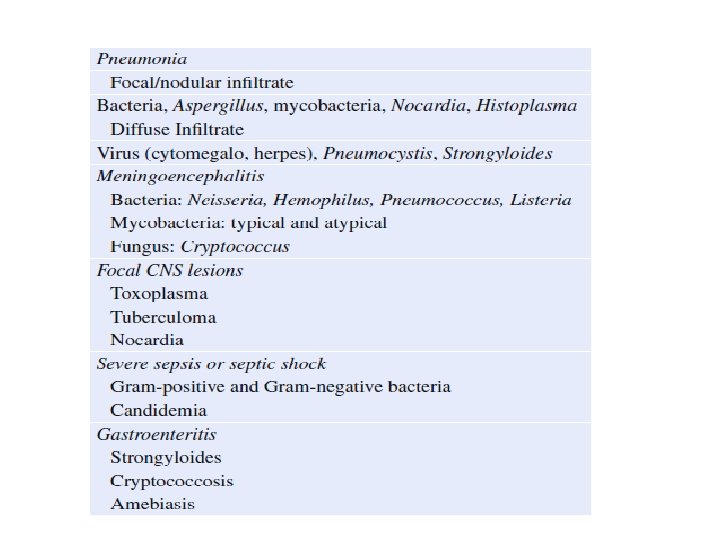
• Differential Diagnosis • Developing an appropriate differential diagnosis for the causative agents of pneumonia in the immunocompromised host • depends on the nature, severity, and duration of the immune suppression. In addition to being Susceptible. • respiratory tract pathogens (S. pneumoniae, H. influenzae), hospitalized • immunocompromised hosts are prone to Gram-negative bacillary pneumonia; those with prolonged (greater than 7 days) • or profound (less than 100 neutrophils per mm 3) neutropenia may become infected with Aspergillus or Zygomycetes spp. T cell-deficient hosts (e. g. , patients with HIV infection, transplant, or lymphoma) are more likely to acquire PCP or • infection with CMV, HSV , endemic fungi (Cryptococcus, Histoplasma) , Nocardia spp, or intracellular bacteria (mycobacteria, Legionella spp). • Patients who have resided in tropical countries may reactivate latent • infection by Strongyloides stercoralis.

• Chest radiographs - focal or multifocal infiltrates tend to suggest infections by bacteria or fungi, . Computerized tomographic scanning often provides more information, including the detection of lesions not seen on routine chest radiograph. Diffuse disease is more characteristic of viral causes (HSV, CMV), PCP, or noninfectious processes (drug toxicity, lymphangitic carcinomatosis, and radiation pneumonitis). • Cavitary disease can be seen with certain of the necrotizing Gramnegative bacilli such as P. aeruginosa S. aureus and anaerobes. • . Cavities also can be a late finding with pneumonia due to Aspergillus, Zygomycetes, and Nocardia spp. . Gram-negative bacilli or Legionella may progress to diffuse disease or incite the acute • respiratory distress syndrome. Patients with severe defects in cellmediated immunity manifest a miliary pattern • caused by disseminated tuberculosis or histoplasmosis. Conversely, radiation pneumonitis may present as focal, sharply • demarcated infiltrates confined to the irradiated portion of the lung

• Diagnostic Approach and Empiric Therapy • The diagnostic approach to pulmonary disease in the immunocompromised host also depends on the nature of the • immune deficit. As a general rule, all accessible sites (blood, urine, and sputum) should be cultured, although sputum of • high quality is obtained rarely in these circumstances. In neutropenic hosts, empiric antibacterial therapy is begun at the • outset regardless of radiographic pattern,

• Computed tomographic scans may show the classic “crescent” sign in patients with aspergillosis • The standard approach to therapy of confirmed pulmonary disease caused by Aspergillus is to treat with voriconazole as • this agent has been shown to be superior to treatment with amphotericin B preparations. • While the use of combinations of antifungal agents (including echinocandins and azoles as well as echinocandins and amphotericin

Pneumocystis carinii pneumonia • More commonin hiv patients • C/F dry cough , dysnoea , fever , fatigue , wt loss • Investigations - CXR shows B/L diffuse peri hilar interstitial shadowing • BAL , Induced Sputum • RX- Trimethoprim +sulfamethaoxazole + steroid • Ptwho are in tolerant to cotrimoxazole • Pentamidine 4 mg /kg/day • Primaquine with clindamycin • Trimetrexate +leucovorin + dapsone

ASPLENIA • PT who have under gone spleenectomy / functionally asplenic secondary to underlying disease like sickel cel disease , splenic artery thrombosis , malaria, have increased risk of encapsulated organisms , eg – strepto. Pneumonia , H. influenza , N. meningitiids • RX- vaccination to prevent

HIV • The CD 4 + Lymphocyte cell count remains an accurate guage of susceptability to opportunistic infections • A. pneumonia - if cd 4 <200 can suspect myco TB , pneumocystis jiroveci , toxoplasma • If < 50 cmv, vzv , and above can suspect • CNS infection • If cd 4 < 100 –listeria , hsv , toxoplasma • If< 50 – can suspect cryptococcus , cmv , ebv associated lymphoma

• Toxoplasma encephlalitis may manifest with fever , headache , altered mental status , seizure , neurological deficit • Ring enhancement lesion are seen in ct / mri • Meningo encephalitis sec to cryptoccus present with headache , photophobia , even coma due raised ICP • IRIS –immune reconstituition inflammatory syndrome is a life threatning emergency usually occurs within days to weeks after initiation of ART

NEUTROPENIC FEVER • Neutropenia is a common complication in pt receiving chemotherapy and hematological malignancy • DEF OF ANC - absolute neutrophil count < 500 cellmm 3 /< 1000 with an anticipated decline< 500 cell / mm 3 over next 48 hrs coupled with the presence of single temp >38 for more than 1 hr

• Mucositis sec to chemotherapy places the neutropenic pt at high risk for infection in sinuses oropharynx , GIT • Invasive fungal sinusitis ( mucormycosis) caused by zygomycetes can progress to severe rhino – orbital infections requiring extensive sx debridement • Neutropenic enterocolitis ( typhlitis) – necrotizinginfection of caecumextendimg to terminal ileum and ascending colon leading to bowel perforation , peritonitis , hemorrhage and sepsis

• Clostridium difficle may present as abd pain with diarrhoea • Translocation of intestinal bacteria acros damaged mucosal membrane can precipitate severe blood stream infections with entero coccus , gram – organisms • Cutaneous and mucosal infection caused by herpes and fungi increases risk of bacterial super infection • Pt with prior h/o Tb incrs risk of reactivation of the disease •

• Disseminated candidiasis with hepaticand aplenic abscess formation may present with abdominal pain and elevatd alkaline phosphatase • Pt with Acute lymphocytic leukaemia / other malignancies receiving high dose of corticosteroids without adequate antimicrobials prophylaxis amy develop PCP • Early emperic ANTIBiotic decrs mortality • Based on locl antimicrobial resistance pattern monoherapy with anti psudomonal , b lactam , carbapenam for broad for GM – coverage is initially recomended • If blood cultrs –ve & if still fever persist start emperic anti fungal therapy

• Management Based Upon Randomized Controlled Clinical Trials and Meta-Analyses of These Trials Acute fever without obvious source: neutropenia • Broad-spectrum antibiotic therapy should be started for all immunocompromised patients with fever greaterthan 38°C and absolute neutrophil counts less than 500/mm 3 (or less than 1, 000/mm 3 and falling) • There is no benefit to continuing vancomycin after 72 h unless a Gram-positive infection is documented. • There is no benefit to adding an aminoglycoside to a β-lactam agent in patients with fever and neutropenia

• Persistent fever or recurrent fever with obvious source: neutropenia • Empiric antifungal with an amphotericin B preparation, voriconazole, or an echinocandin should be started • for the immunocompromised patient with neutropenia and fever of 4– 7 d duration. • Treatment of aspergillosis • Voriconazole is the drug of choice for documented infections due to Aspergillus. • Prophylaxis of fungal infections • In patients undergoing chemotherapy for acute myelogenous leukemia or the myelodysplastic syndrome, posaconazole prevented invasive fungal infections more effectively than did either fluconazole or • itraconazole and improved overall survival. • Both fluconazole and itraconazole have shown benefit for prophylaxis in patients after allogeneic stem cell transplant
 administration has been studied")
• PREVENTION OF INFECTION • Oral fluoroquinolone (and trimethoprim-sulfamethoxazole) administration has been studied in patients with prolonged • neutropenia. These agents reduce levels of aerobic Gramnegative bacilli in the gut lumen, the major reservoir for • dissemination of infection in the neutropenic host, • Antifungal prophylaxis with oral fluconazole (400 mg orally daily or 200 mg IV every 12 hours) has proved effective in • reducing infection by Candida spp in bone marrow transplant recipients. • Recent studies suggest that posaconazole, which has a much broader spectrum than fluconazole (including Aspergillus), is efficacious in preventing fungal infections in severely neutropenic patients, hematopoietic stem cell transplant patients, and those with graft versus host disease
- Slides: 31