Development of the heart Mark Kozsurek M D
























 orifice. Formation of the interatrial septum. Formation of")




















 from the right ventricle ascends and from")






")





 / persisting foramen ovale (PFO): septum primum and secundum")

")



- Slides: 68
Development of the heart Mark Kozsurek, M. D. , Ph. D. mark@kozsurek. hu ED I. , 20/02/2018
Development of the heart includes: n n formation of the heart tube, twisting and further differentiation of the heart tube, partitioning of the heart – complete isolation of the left and right halves, formation of the valves.
I. Early development of the heart: appearance of the heart tube
oropharyngeal membrane septum transversum cloacal membrane amniotic cavity connecting stalk cardiogenic area yolk sac extraembryonic celom
Note that heart starts to develop anterior to the brain! brain spinal cord
Heart primordium appears on the 18 th-19 th days (the end of the third week). At this stage the embryo is a flat, trilaminar disc and the differentiation of the three germ layers has just begun. Heart develops from the cardiogenic area, a part of the intraembryonic mesoderm anterior to the oropharyngeal membrane and posterior to the septum transversum.
cardiogenic area amniotic cavity lateral plate mesoderm yolk sac somatic layer splanchnic layer intraembryonic celom
somatic layer splanchnic layer angioblastic cords A group of cells leaves the splanchnic mesoderm, moves medially and forms the angioblastic cords.
somatic layer splanchnic layer endocardial tubes myoepicardial mantle On the dorsal side of the endocardial tube, the splanchnic mesoderm thickens and forms the myoepicardial mantles.
Further development of the heart is mainly determined by the folding of the embryo (4 th week). The folding includes: 1) „flexion” around transverse axes – this will explain, how the heart primordium moves from „above the head” into the chest occupying its final position. 2) „rolling” around the longitudinal axis – this will mainly explain the fusion of the structures originally developing on the two sides of the embryo.
The „flexion”
The „rolling” foregut intraembryonic celom pericardial cavity dorsal mesocardium
Folding of the embryo, especially the „rolling”, results in the fusion of the two endocardial tubes in the midline. Somewhat later the myoepicardial mantles also unite and surround the endocardial tube. The intraembryonic celoms fuse ventrally, and finally, the dorsal mesocardium disappears.
The heart tube, branching both rostrally and caudally, is surrounded by the pericardial cavity.
Summary Cells emigrating from the splanchnic mesoderm form the endocardial tubes, this gives later the ENDOCARDIUM. Thickening of the splanchnic mesoderm gives the myoepicardial mantles from which the MYOCARDIUM, and the VISCERAL LAYER OF THE PERICARDIUM (EPICARDIUM) develop. Intraembryonic celom, originally bounded by the lateral plates, transforms into the PERICARDIAL CAVITY. Somatic layer of the mesoderm differenciates into the PARIETAL LAYER OF THE PERICARDIUM.
II. Twisting and further differentiation of the heart tube
As the two ends of the heart tube are fixed, its intense longitudinal growth necessarily results in the formation of several loops and curvatures. Furthermore some parts of the tube remain narrower, while others dilate. The venous end moves backward and ascends and gets behind the slightly descending arterious end. cardiogenic plate endocardial tubes and their fusion 6 5 4 3 1 -2 6 5 4 3 2 1 6 4 5 3 2 1 RV Common ventricle gives the later LV and the inflow part of the RV, while the bulbus cordis differentiates into the outflow part of the RV! LV 1. 2. 3. 4. 5. 6. sinus venosus common atrium atrioventricular canal common ventricle bulbus cordis truncus arteriosus
TRANSVERSE SINUS su s ve no us sin common atrium truncus arteriosus bulbus cordis atrioventricular canal sup. post. ant. common ventricle inf. OBLIQUE SINUS
os us sinus venosus sin u s v en truncus arteriosus right sinus horn sinu-atrial opening common atrium atrioventricular canal bulbus cordis common atrium common ventricle lateral view atrioventricular canal Note the right and left sinus horns draining into the sinus venosus and the right and left veinous valves (green) at the sinu-atrial opening! common ventricle frontal view left sinus horn
os us sinus venosus sin u s v en truncus arteriosus common atrium atrioventricular canal right sinus horn left sinus horn → coronary sinus sinu-atrial opening bulbus cordis common atrium common ventricle The sinu-atrial opening moves to the right, the left sinus horn (or duct of Cuviér) involutes and persists as the coronary sinus. atrioventricular canal common ventricle
os us SVC sin u s v en truncus arteriosus left sinus horn → coronary sinus venarum common atrium atrioventricular canal sinu-atrial opening bulbus cordis IVC common atrium common ventricle Note three veins opening into the sinus venarum (derivative of the sinus venosus): the superior and inferior vena cava and the coronary sinus! atrioventricular canal common ventricle
os us SVC sin u s v en truncus arteriosus coronary sinus venarum common atrium atrioventricular canal sinu-atrial opening bulbus cordis IVC common atrium common ventricle Pulmonary veins arise from (or enter) the left portion of the common atrium. atrioventricular canal common ventricle pulmonary veins
os us SVC sin u s v en truncus arteriosus coronary sinus venarum common atrium atrioventricular canal pulmonary veins sinu-atrial opening bulbus cordis IVC common atrium common ventricle Sinus venarum and pulmonary vein segments getting incorporated into the atrial wall will give the smooth-walled parts of the atria (blue), while the original regions of the common atrium will persist as the rough parts of the atria. atrioventricular canal common ventricle SMOOTH ROUGH
III. Partitioning of the heart
Septation of the common atrioventricular (AV) orifice. Formation of the interatrial septum. Formation of the muscular interventricular septum. Appearance of the membranous interventricular septum and the spiral aorticopulmonary septum.
right left
septum primum
septum primum
septum primum foramen primum
septum primum foramen primum
septum primum foramen secundum foramen primum
septum primum foramen secundum foramen primum
septum primum foramen secundum
septum secundum foramen ovale septum primum
septum secundum foramen ovale septum primum
septum secundum foramen ovale septum primum
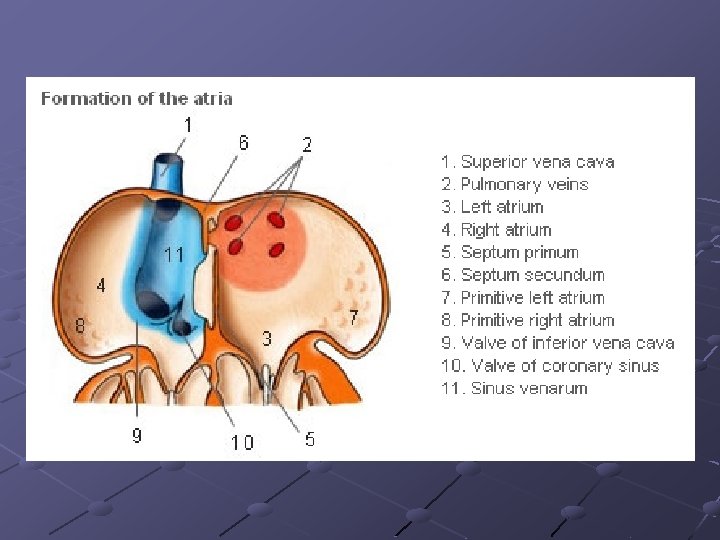
Summary The septation of the common atrium starts with the appearance of the crescent-shaped septum primum. The opening of this septum, the foramen primum, becomes progressively smaller. Before the foramen primum completly closes, postero-superiorly several small openings appear on the septum primum. These perforations coalesce later and form the foramen secundum. On the right side of the septum primum a new septum, the septum secundum, starts to grow. The orifice of the septum secundum is the foramen ovale. Finally two crescent-like, incomplete, partially overlapping septa exist with one hole on each. Septum secundum is more rigid and the septum primum on its left side acts as a valve letting the blood flow exclusively from the right to the left. Its importance will become obvious when the fetal circulation is discussed.
septum secundum foramen ovale septum primum
septum secundum foramen ovale septum primum
septum secundum foramen ovale septum primum interventricular foramen
Summary Nothing is simplier then the development of the muscular part of the interventricular septum. Similarly to the processes observeble at the level of atria, a crescent-like septum appears on the floor of the common ventricle. This septum grows upward until it reaches the bulbus cordis. Here the interventricular foramen persists for a while and will be closed by an other septum.
dorsal aortae septum secundum foramen ovale interventricular foramen 6 th aortic arches * truncus arteriosus septum primum bulbus cordis *: differentiate into pulmonary arteries!!!
dorsal aortae 6 th aortic arches In the bulbus cordis and the truncus arteriosus two endocardial thickenings, bulbar and truncal ridges appear and exhibit a spiral course twisting 270 degrees* (90 degrees in each third of the full length). * Different values between 180 and 270 degrees can be found in different textbooks.
dorsal aortae 6 th aortic arches The two bulbar and truncal ridges (= conotruncal ridges as used by others) approach each other.
dorsal aortae „hook” 6 th aortic arches Finally, a complete spiral septum is formed. An additional hook-shaped septum arises from the superior edge of this septum and isolates the posterior portion of the truncus arteriosus.
dorsal aortae pulmonary arteries Venous blood (blue) from the right ventricle ascends and from the posterior portion of the truncus arteriosus may only flow toward the pulmonary arteries developing from the 6 th aortic arches. Blood from the left ventricle (red) exits through the two dorsal aortae.
dorsal aortae septum secundum pulmonary arteries foramen ovale septum primum interventricular foramen
dorsal aortae septum secundum pulmonary arteries foramen ovale septum primum
conotruncal = bulbar/truncal ridges Closure of the interventricular foramen and formation of the membranous part of the interventricular septum result from the fusion of tissues from three sources: the right bulbar ridge, the left bulbar ridge, and the endocardial cushion growing on the top of the muscular septum.
Why is the formation of the aorticopulmonary septum so complicated? straight tube bent tube discrepancy between the length of the red and blue patways bent tube crossing of the two patways eliminates the former discrepancy
Summary Finally a spiral septum twisting 270 degrees develops within the bulbus cordis and truncus arteriosus. The inferior portion of the spiral septum (also called bulbar septum) unites with the muscular interventricular septum. The superior part of the spiral septum (truncal septum or more commonly the aorticopulmonary septum) isolates the aorta and the pulmonary trunk. With this step, the septation of the common ventricle into a left and right half is completed. Must be noted, that the uncomplete union of the membraneous aorticopulmonary and the muscular interventricular septum is the most frequent reason of the ventricular septal defect, one of the most common heart malformations. (Roughly occurs in 1 out of 100 newborns. ) Spiral orientation of the aorticopulmonary septum can be explained by the spiral blood flow due to the bending of the heart. Walls develop where they are let to develop: where the blood streams are relatively quiet.
IV. A few words about the valves. . .
(sinu-atrial junction)
Eustach Thebesius
Right and left venous valves: two semilunar structures at the sinu-atrial junction. Postero-superiorly they unite and form the septum spurium. The left one later completly disappears by fusing with the interatrial septum. The right one divides into two: the upper part persists as a part of the crista terminalis, while the lower gives the mass of the Thebesian and the Eustachian valves.
bulbar ridges A PT posterior anterior secondary endocardial cushions
Semilunar valves: right and left semilunar valvulae of the aorta and the pulmonary trunk develop from the bulbar ridges (primary endocardial cushions) also beeing responsible for the formation of the aorticopulmonary septum; anterior semilunar valvula of the pulmonary valve and the posterior valvula of the aorta arise from secondary endocardial cushions. Atrioventricular valves: endocardial proliferation around the AV orifices.
Malformations 1. situs inversus totalis: all the viscera are mirrored. Prevalance is less than 1/10 000.
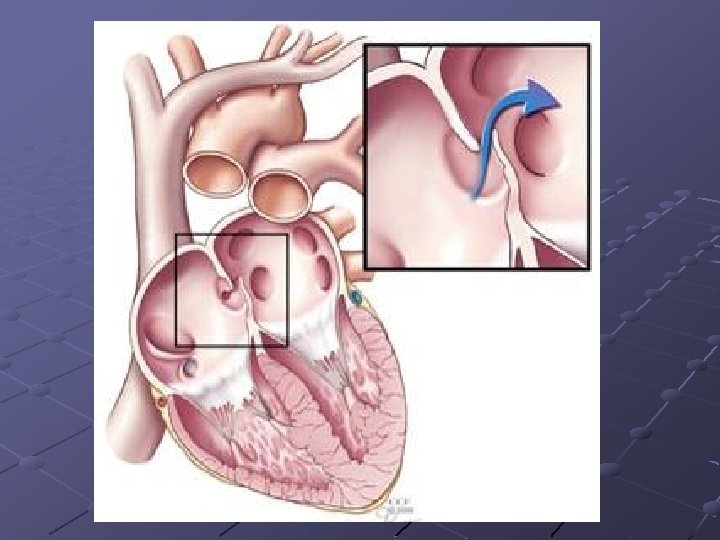
3. atrial septal defect (ASD) / persisting foramen ovale (PFO): septum primum and secundum do not overlap completly.
2. dextrocardia: only the heart is swapped to the right side of the thorax (first seen and drawn by Leonardo da Vinci in 1452– 1519)
4. ventricular septal defect (VSD)
5. transposition of the great vessels: aorticopulmonary septum twists only 90 degrees.
6. Tetralogy of Fallot: a complex malformation
Thank you for your attention!