Greenstick fracture Transverse fracture Fracture Epiphyseal Fracture Torus






















 Definitive diagnostic test Rules out other conditions")



















































")

























 Osteoarthritis is very common Anyone over 35 YOA Progressive loss of cartilage (wear")




















 Ice Compression Elevation Analgesia")



























 Boot Unstable (tibia or both) Splint and refer")














- Slides: 173
Greenstick fracture
Transverse fracture Fracture
Epiphyseal Fracture
Torus or Buckle fracture Occurs after a minor fall on the hand. Fractures are very stable and are not as painful as unstable fractures. Heal uneventfully in 3 -4 weeks. 4 3/5/2021
Torus or Buckle Fracture
Colle’s Fracture wrist Mechanism: Fall on an outstretched hand Most Common fracture of distal radius Signs and Symptoms: “Silver Fork” deformity seen, with dorsal angulation of distal radius Tests: X-ray Treatment: Analgesics, close reduction, volar splint, surgery
Colle’s Fracture
Colle’s Fracture
Smith’s Fracture Opposite of Colle’s Fracture, “Smith Fracture” or “Reverse Colles” has volar angulation of distal radius Swelling, tenderness, deformity Volar wrist splint
DON’T CAST UNTIL SWELLING HAS SUBSIDED!! Putting on a cast while the injury is acute risks causing compromise of circulation. Leave finger tips exposed to check color, sensation, movement and cap refill! Have patient remove elastic bandages (splint) and re-apply more loosely as required
Scaphoid bone
Scaphoid Fracture
Scaphoid Fractures Fall on outstretched hand Most common carpal fracture Tenderness & swelling in anatomical “snuffbox” Fractures are often “occult”. (2 -5 % not seen on initial x-ray but patient has persistent point tenderness over anatomic snuffbox 3/5/2021 13
Scaphoid Fracture Mechanism: Fall on an outstretched hand Most Common carpal fracture Signs and Symptoms: Tenderness and swelling in the anatomical “snuffbox” Tests: X-ray, Treatment: Thumb-spica splint, analgesics and surgery when displaced Complication is avascular necrosis because radial artery provides blood supply form distal to proximal poles Burroughs KE. Scaphoid fractures. Uptodate Topic 197 Version 11. 0. 2012
Scaphoid arterial supply
Anatomical Snuffbox The anatomical snuffbox is formed by the tendons of the extensor pollicis longus, and brevis and abductor pollicis longus.
Anatomical snuffbox
Carpal Tunnel Syndrome Mechanism: Inflammation of the carpal canal, resulting in compression of median nerve More common in women (smaller canal? ) pregnancy diabetes, hypothyroid Assembly workers 3 X more common than data entry Signs and Symptoms: Paresthesias in median nerve distribution
Clinical Tests for CTS Positive Phalen’s and Tinel’s sign Positive Flick signal= patient flicks hand as if shaking down a thermometer to relieve symptoms Thumb abduction test=the abductor pollicis brevis is innervated by the median nerve only. Weakness is associated with CTS
Phalen’s and Tinel’s signs Phalen’s 25% false positives Tinel’s 6 -45% false positives
CTS - Median Nerve Distribution
Manual compression testing Apply pressure over transverse carpal ligament for 30 seconds. + if pain/paresthsias 64% sensitivity 83% specificity
Electromyography, Nerve Conduction Study (EMG/NCS) Definitive diagnostic test Rules out other conditions
Carpal Tunnel Syndrome Treatment Conservative at first: wrist splinting at night or all day, rest from repetitive movements OT therapy has been shown to be beneficial NSAIDs have not been shown to be better than placebo corticosteroid injections combined with splinting and limited to once every 6 months have been shown to be helpful but if the problem persists surgery is more effective for long term relief Surgical: “Release” has 15 -20% failure rate
Aim for the ring finger Injection over the hook of the hammate
Ganglion Cyst May wax and wane spontaneously If asymptomatic, watchful waiting is appropriate Aspiration and injection of glucocorticoid Surgical removal
Boxer’s Fracture Mechanism: Closed-fist injury Fracture of the distal 5 th metacarpal Watch for knuckle lacerations! open fractures, tooth lac Signs and Symptoms: Pain, swelling, tenderness, and loss of prominence of knuckle at the little finger Tests: X-ray
Metacarpal Neck Fracture Treatment 2 nd & 3 rd metacarpal neck fractures cannot tolerate significant angulation due to the lack of motion at the CMC joint. Angulation >10 degrees at the 2 nd and >20 degrees at the 3 rd warrant reduction or referral 4 th & 5 th metacarpal neck fractures tolerate greater angulation (up to 30 degrees) due to increased mobility at the CMC joint. Most of these fractures result in good functional results even with significant degrees of angulation No approach has been shown to be superior to rigid splint immobilization
Open Fractures Any fracture that breaks skin causes an increased risk of bacterial contamination of the wound. Osteomyelitis, gas gangrene or tetanus may occur. Treatment: IV antibiotics immediately. Admission and surgical debridement may be nesessary Ask about whether it was a punch to someone's face/teeth for HIV and Hepatitis exposure screen. 32 3/5/2021
De Quervain’s Tenosynovitis Covered by Dr. Cleveland Stenosing Tenosynovitis in which the synovial lining of the tunnel becomes inflamed and hurts with movement. Mechanism: Excessive use of the thumb Involves the tendons of 2 muscles—extensor pollicis brevis and abductor pollicis longus
Extensor pollicus brevis
Abductor pollicus longus
De Quervain’s Tenosynovitis Covered by Dr. Cleveland Signs and Symtoms: Pain, tenderness, redness, swelling at side of wrist beneath base of thumb Positive Finkelstein test—pain when thumb is folded across palm and fingers are flexed over thumb as hand is pulled away from wrist Tests: Excellent history and physical exam Treatment: Thumb spica splint NSAIDs and ice may help in the acute phase Steroid injections Up to 90% will benefit if treated within 6 months of onset of sx Surgical referral if sx recur after 2 nd injection
Finkelstein’s test
More proximal wrist pain
Intersection syndrome Is inflammation of the crossover point of the abductor pollicis longus and extensor pollicis brevis with the extensor carpi radialis longus and brevis. Patients have a history of overuse. Pain is worse with wrist motion. Pain, edema and crepitus 4 to 8 cm proximal to radial styloid is pathopneumonic Splint wrist in 15 degrees extension (position of function), rest, Rx NSAIDs for 2 to 3 weeks. PT extensor strengthening
Intersection syndrome
Activity modification
Activity modification
Phalangeal Fractures/Sprains ½ of all hand injuries Nail bed injuries are common Open fractures or extensive soft tissue or boney injury, i. e. crush injury, require consultation with a hand specialist Nondisplaced fractures can be treated with immobilization splint
Mallet deformity Swan Neck Deformity Boutonniere Deformity
Mallet finger
Notice the padding!
If you work where I do, you might have to make one
This one is available at most pharmacies
Pelvic Trauma Pelvic fractures represent approximately 3 percent of skeletal injuries. Overall mortality from pelvic fractures ranges from 5 to 16 percent, with the rate for unstable pelvic fractures approximately 8 percent. The mortality rate associated with acetabular fractures is 3 percent, while open pelvic fractures, which comprise 2 to 4 percent of all pelvic fractures, are associated with a mortality rate of up to 45 percent. Most fatalities stem from associated internal injuries; deaths attributed solely to pelvic fractures range from 0. 4 to 0. 8 percent of trauma fatalities. Patients aged greater than 65 with pelvic fractures have a mortality rate of approximately 20 percent. Overall, pelvic fractures are associated with an increased risk of death among trauma patients
Pelvic Injuries They include pelvic ring fractures, acetabular fractures, and avulsion injuries. The majority of pelvis injuries are due to high energy blunt trauma, although frail and elderly patients may sustain such injuries from a low energy mechanism, i. e. a fall.
Pelvic Injuries - Hx Mechanism of injury Ambulatory at the accident scene Location of pain Bowel or bladder incontinence Numbness or weakness Bleeding: hematuria, rectal or vaginal bleeding Last menstrual period
Pelvic Injuries - PE Inspection External bleeding Ecchymosis Position of LE and iliac crests Check lumbosacral spine and gluteal regions Palpation Iliac crests, pubic symphysis, sacrum, SI joints, greater trochanters Gentle compression (8% sensitivity) DRE U/A Plain X-ray if hemodynamically unstable Gold standard for diagnosis is multidetector computed tomography (MDCT)
Disorders of the Lower Extremity Hips Knees Ankles Feet
DDx of “kid a with funny walk” Infection- septic arthritis, myositis Inflammation- synovitis Trauma-Fx infancy and from fall of own height- suspect abuse Deformities- Slipped capital femoral epiphysis, hip dysplasia Aseptic necrosis- Legg-Calve-Perthes, osteochondritis Tumors
Congenital Hip Dislocation If a congenitally dislocated hip is flexed and abducted and externally rotated, the femoral head slips over the acetabular rim, reducing the dislocation and producing a palpable and/or audible click or jerk. This is called the Ortolani click.
Barlow maneuver Posterior pressure is applied to the greater trochanters to cause posterior subluxation/dislocation Determines if the hip is dislocatable
Ortolani Anterior pressure is applied to greater trochanters to reduce the posterior dislocation Determines if the hip is reducible
Congenital Hip Dislocation
Congenital Hip Dislocation
Congenital Hip Dislocation X-rays cannot diagnose this until 3 months of age Ortalani and Barlow maneuvers must be done on all infants and documented as + or If it is not diagnosed and corrected by conservative means before the child begins to walk it may result in permanent disability
Slipped Capital Femoral Epiphysis Mechanism: A Salter-Harris Type I epiphyseal fracture is seen and the epiphyseal growth plate is unusually widened Abnormal cartilage maturation occurs, leading to disruption of normal architecture and slippage occurs through this weakened area Most Common adolescent hip disorder Prevalence: 10 cases/100, 000 persons
SCFE Adolescent, ball of femur slips backwards, weakness of growth plate
Slipped Capital Femoral Epiphysis The child with SCFE usually presents with pain and a limp. Since the pain is often located only in the thigh or knee, the diagnosis is often missed. It is important to remember that knee pain in the child can be secondary to hip disease.
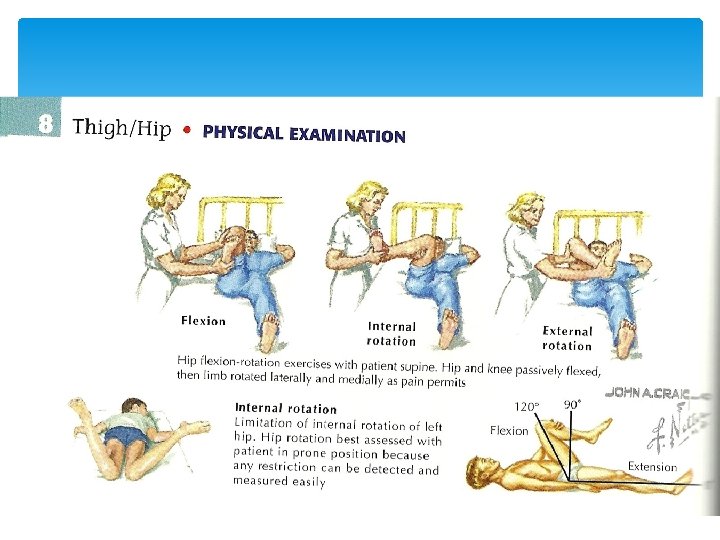
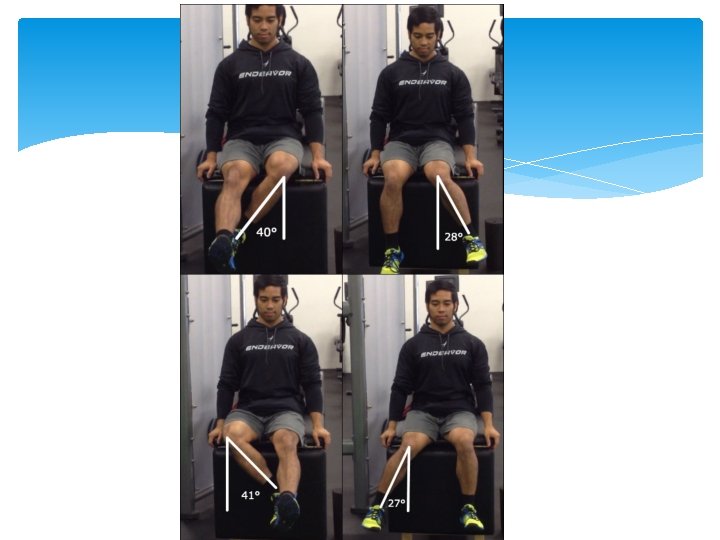
Slipped Capital Femoral Epiphysis On physical examination, there is frequently limitation of motion, especially internal rotation and abduction. As the examiner flexes the hip, it moves into external rotation and the patient often holds the leg externally rotated when standing.
Slipped Capital Femoral Epiphysis Tests: X-ray A/P and Lat views Femoral head is displaced posteriorly and inferiorly in relation to femoral neck Determine whether Klein Line is present—on A/P view, a line drawn along superior border of femoral neck should pass through a portion of the femoral head; if not, SCFE is diagnosed Treatment: Surgery with internal fixation Prognosis of osteoarthritis if it is not recognized and treated
Slipped Capital Femoral Epiphysis Klein Line
Salter Harris
Useful mnemonics for remembering the Salter-Harris classification system is: SALTR or SMACK Fortunately this is also the order of prognosis (from best to worse) SALTR • S: slipped (type I) • A: above (type II) • L: lower (type III) • T: through or transverse or together (type IV) • R: ruined or rammed (type V) SMACK • S: slipped (type I) • M: metaphyseal (type II) • A: articular-epiphyseal (type III) • C: complete-metaphysis and epiphysis (type IV) • K: krushed! (type V)
Avascular Necrosis Most commonly involves the femoral head. It is usually caused by trauma, typically occurring after a displaced femoral neck fracture and less frequently after a fracture-dislocation of the hip. Necrosis results when the vascular supply to the femoral head is disrupted at the time of injury. Non-traumatic AVN occurs in a younger population and is commonly bilateral. Corticosteroid use can result in AV Even one dose!!!
Femur circulation
Avascular Necrosis Signs and Symptoms Gradual onset pain that progresses and worsens to severe pain Decreased range of motion Arthritis May take months to a year for sx’s to progress
Avascular Necrosis Tests The Gold Standard is MRI, bone scan. The X-ray in early stage is normal, late stage may show changes.
Avascular Necrosis
Avascular Necrosis Treatment: Two approaches Conservative Medications NSAIDS Meds to reduce fatty substances (lipids) that increase with steroid use (statins) Meds to decrease coagulation in clotting disorders Vasodilators bisphonates Decrease weight bearing and exercises Nonoperative management has generally been ineffective at halting the progression of disease Surgical Bone graft Total hip arthroplasty (THA)
Hip fracture 310, 000 individuals were hospitalized with hip fractures in the United States alone in 2003 30 percent of all hospitalized patients Hip fractures substantially increase the risk of death and major morbidity in the elderly Femoral neck and intertrochanteric fractures occur with approximately the same frequency in patients between the ages of 65 and 99 years Isolated trochanteric fractures occur more often in young, active adults between the ages of 14 and 25
Hip Fractures Major risk factors for hip fractures among elderly patients include osteoporosis and falls Mechanism of injury: A fall directly onto the lateral hip A twisting mechanism in which the patient's foot is planted and the body rotates A sudden spontaneous completion of a fatigue (or insufficiency) fracture, which then causes a fall Did they fall and break their hip or did they break their hip and fall?
Hip fracture – Signs and Symptoms Sudden onset of hip pain before or after a fall and the inability to walk Assess for syncope as a cause of the fall Assess for other trauma associated with the fall Head? Arm? The leg may appear shortened and externally rotated
Hip Fracture - Treatment Depending on overall functional status Nonoperative management Nonambulatory Demented Unstable with major, uncorrectable comorbid disease Patients at the end stage of a terminal disease Surgical Open reduction with internal fixation (ORIF)
Hip Dislocation
Hip Dislocation High energy MVA most common cause Fall from a significant height One story – ankle fracture Two story - hip fracture Because of mechanism of injury always check for other injuries, i. e. lower leg, pelvis, back, abdomen, head, neck Always do a good distal neuro and circulatory exam
Hip dislocation closed reduction - Captain Morgan technique
DDx of “hip Pain” Lateral hip pain aggravated by pressure Trochanteric bursitis Rest, ice, NSAIDs Glucocorticoid + local anesthetic injection Lateral hip pain associated with paresthesias and hypesthesias Meralgia paresthetica Anterior hip or groin pain Primary involvement of the hip joint OA, osteonecrosis, occult fracture, acute synovitis, septic arthritis (uncommon)
DDx of “hip Pain” Posterior hip pain Least common SI joint dis Lumbar radiculopathy HZV Unusual hip joint Lower anterior thigh pain Clinically challenging Primary hip joint dis Lesions of the upper femur Stress fracture of femoral neck Upper lumbar radiculopathy
PE of the Hip Inspection Palpation Distal N/V exam Specific ROM Stabilize contralateral ASIS to test abduction Put patient in LL decubitus and stabilize ipsilateral ASIS to test extension
extension Abduction
Adduction
Flamingo test for SI joint pain
Knee Effusions Internal derangements: Meniscal tears Cruciate ligament tears Dislocations Infection Inflammation
Swollen knee Hx Trauma? Fever? STD? Diarrhea? PE: Effusion? Warm? Erythema? Special tests for internal derangement. Joint aspiration when? When Hx of infection but no trauma, fever, warm joint
Knee Effusion “Water on the knee” is increased synovial fluid in the joint. Several tests help evaluate this: Balloon Ballottement Bulge DDx of someone with knee effusion includes internal derangement, inflammation, infection
Knee Effusion
Bulge Sign
Balloon Sign
Ballottement
Septic arthritis Risk factors: Advanced age, DM, arthritis, prosthetic joint, recent trauma or surgery or corticosteroid injection or soft tissue infection to the region, IV drug use, alcoholism. Patients complain of acute joint pain, swelling usually in one joint, usually knee. The patient may report fever. There may be recent Hx of skin, urinary, or lung infection.
Septic arthritis PE: Patient may be febrile. Joint is warm, swollen, with restricted ROM. Diagnosis is by synovial fluid aspiration and analysis with gram stain, leukocyte count, and culture. Culture is considered definitive. Synovial fluid will have leukocytosis 50 -150, 000 cells/mm 3 Blood culture may be positive, ESR and CRP are usually elevated. Radiographs should also be taken to assess for osteomyelitis.
Septic arthritis If gram stain is positive, vancomycin should be initiated IV. If gram stain is negative, a third generation cephalosporin should be used. IV antibiotics are used for 14 days followed by 14 days of oral medication. Some orthos drain the joint. Osteoarthritis sometimes follows DDx includes reactive arthritis, rheumatoid arthritis, Lyme disease, gout and psuedogout
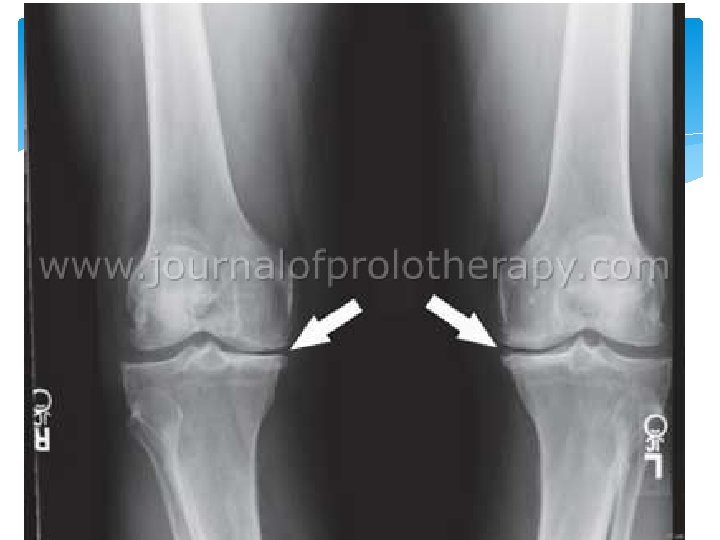
(Arthritis) Osteoarthritis is very common Anyone over 35 YOA Progressive loss of cartilage (wear and tear) Loose weight NSAIDS Activity Knee replacement
Patella Fracture Signs and Symptoms are swelling, tenderness, hemarthrosis Proximal displacement of patella Difficulty with weight bearing Inability to actively extend knee Sometimes a palpable gap
Patella Fracture
Anterior-posterior instability of the knee Tests for Anterior-posterior instability, or injury to the cruciate ligaments include the Lachman and Drawer tests. Anterior displacement of the tibia implies anterior cruciate ligament tear. Posterior displacement of the tibia implies posterior cruciate ligament tear.
Cruciate Ligament Tear Provides anterior/posterior stability May see partial or complete tear Mechanism: Twisting injury with usual contact (athletes) Signs and Symptoms include pain, swelling, hemarthrosis and instability Tests: MRI, Drawer test, Lachman test Treatment: RICE, knee immobilizer, analgesics, surgery
Anterior Cruciate Ligament
Joint line tenderness
Drawer Test
Lachman Test
Lachman Test
Valgus stress test for the medial collateral ligament. With the patient supine, press the lateral side of the knee in a medial direction, while pressing the medial ankle in a lateral direction.
Medial Collateral Ligament The unhappy Triad: Medial col. Lig. Medial men. ACL
Varus Stress Checks stability of Lateral Collateral Ligament With the patient supine, press the medial side of the knee in a lateral direction, while pressing the lateral ankle in a medial direction.
Meniscus Tear Mechanism: Trauma and twisting injury Medial meniscus most commonly torn Signs and symptoms: pain, “clicking”, “locking”, effusion, and joint line tenderness Pain and effusion are often delayed a day after injury Tests: MRI, positive Mc. Murray sign Treatment: analgesics, knee immobilization, conservative vs. surgical intervention
Meniscus Tear
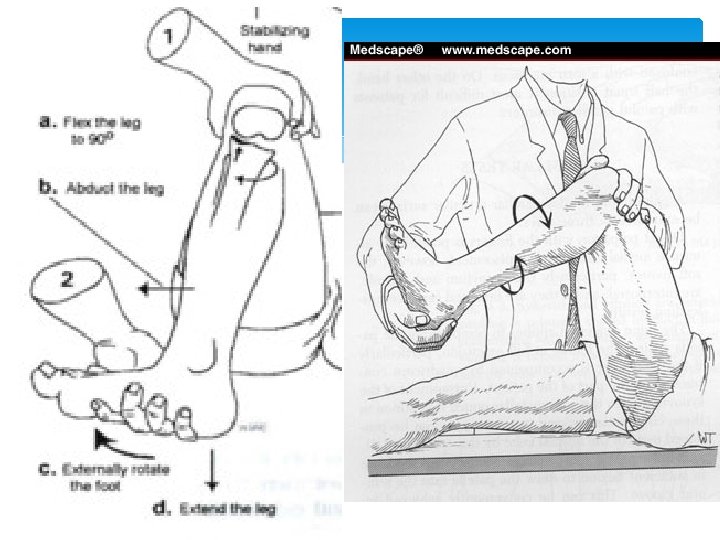
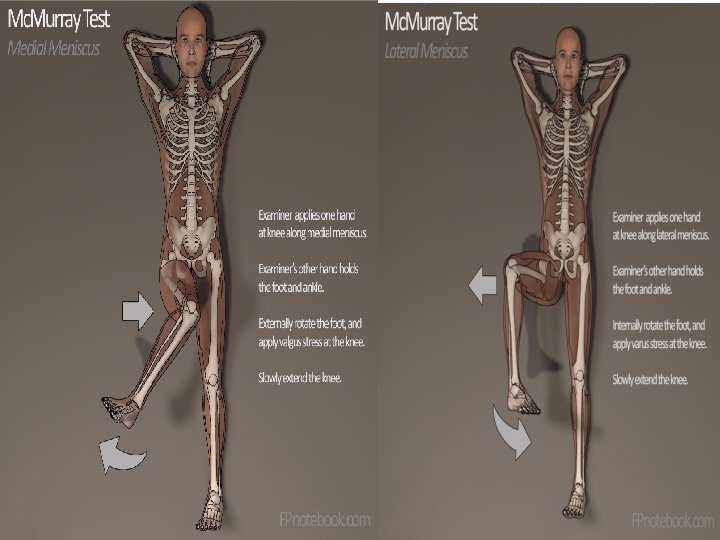
Meniscus exam Palpate joint line tenderness Mc. Murray’s One palm on distal femur with fingers and thumb on joint line, the other palm is on the calcaneus. The knee is flexed to 90°. Rotate the heel (first internal then external) while compressing the knee (push your palms together), then extend the knee keeping the rotation. Repeat with the opposite rotational component.
Mc. Murray Sign This test is performed with the patient in a supine position on the table, with the practitioner holding the proximal tibia in one hand, and the distal femur in the other. A figure eight motion is made, putting medial and lateral pressure against the two menisci. Clicking, locking, and pain indicate a tear.
Meniscal exam Appley’s compression test
Knee dislocation Popliteal artery is at risk for injury whenever a patient sustains a posterior dislocation of the knee and should be evaluated with an arteriogram despite the presence of pedal pulses. 128 3/5/2021
Knee Dislocation Signs and Symptoms: Gross deformity to leg, swelling and immobility Perform thorough vascular exam because: Popliteal artery injury occurs in 7 -45% of dislocations Peroneal nerve injury occurs in 25 -35% of dislocations Decreased sensation to first webspace with impaired dorsiflexion of foot
Knee Injury Treatment Rest (immobilization) Ice Compression Elevation Analgesia
Knee Aspiration
Osgood-Schlatter’s Disease= Osteochondritis of tibial tuberosity= Tibial tuberosity avulsion Due to a traction avulsion lesion of the tibial tubercle and represents an avulsion fracture - healing to a degree and then further being avulsed. Presents gradually in a Male> female child 914 adolescent athlete as a very painful mass on one or both tibial tuberosities. It is exacerbated by kneeling and activity.
Osgood-Schlatter’s Disease
Osgood-Schlatter’s Disease Dx On PE, the pain and tenderness is directly over the tibial tuberosity. Pain is exacerbated by knee extension and squatting. X-ray is not necessary to make the Dx, which is clinical. If done to differentiate, X-ray will show DDx includes slipped capfem epishesis and Legg-Calve-Perth’s, tumor
Osgood-Schlatter’s Disease Rx Continue sports activity Pain control with Acetaminophen, NSAIDs Wrapping Ice PT to strengthen quads, ROM quads and Hams Prognosis is great and resolves when epiphyseal plates close.
Bursa of the knee
Bursitis of the Knee
Bursitis of the Knee
Knee Bursitis Treatment Aspiration and drainage combined with padding and protection are the treatments of choice for acute prepatellar bursitis Glucocorticoid injection For recurrent, nonseptic bursitis Septic 80% pathogen is S. aureus For mild inflammation clincamycin, doxycycline or TMP/SMZ If patient is immunocompromised or inflammation is severe IV Vanco
Edema History Ask a patient if his legs are swollen, or if rings are tight. Be sure to determine onset, duration, aggravating factors.
Pitting edema If the pressing causes an indentation that persists for some time after the release of the pressure, the edema is referred to as pitting edema. It is measured, and therefore documented as 1+, 2+, 3+ and 4+.
Pitting Edema CHF, Kidney failure, and Liver failure all cause pitting edema. 1+ =2 mm 2+ =4 mm 3+ =6 mm 4+ =8 mm
Pitting edema The most common local conditions that cause edema are varicose veins and thrombophlebitis of the deep veins of the legs.
Nonpitting edema The skin does not result in a persistent indentation. Non-pitting edema can occur in certain disorders of the lymphatic system such as lymphedema, that may occur after a mastectomy, lymph node surgery, or congenitally. Pretibial myxedema is a swelling over the shin that occurs in some patients with hyperthyroidism.
Edema
Unilateral pedal edema For Unilateral pedal edema, DVT should be at the top of your DDx
0 -2 low, 3 -6 moderate, >6 high probability of DVT
Ankle Fractures Signs an Symptoms: inability to bear weight Can’t walk more than 4 steps Pain and swelling Point tenderness Obvious deformity
Ankle Sprain Mechanism: Inversion forces Most common injury of the ankle Most common ligament injured— anterior talo-fibular ligament
Anterior Talofibular ligament
Ankle Sprain
Sprain versus Strain Sprain: involves collagenous tissue such as ligaments and tendons Mechanism by twist or stretch Strain: injury to the bone-tendon unit at the myotendinous junction or the muscle itself Mechanism by muscle contraction
Check ankle ligament instability with the drawer test
Ankle Fractures Signs an Symptoms: Inability to bear weight Can they walk more than 4 steps Pain and swelling Point tenderness Obvious deformity HMMM sounds just like a sprain! If in doubt get an Xray
Ankle Fractures are commonly either medial or lateral, but may be complex: Bimalleolar fracture—Pott’s fx or Dupuytren fx Trimalleolar fracture—Henderson fx (involves medial, lateral, and posterior malleoli of tibia)
Ankle Fractures
Ankle Fracture treatment Stable fracture (fibula) Boot Unstable (tibia or both) Splint and refer to ortho depending on the Mof. I, N/V status
Same mechanism as sprain Boot top fracture
Plantar Fasciitis Common cause of foot/heel pain Inflammation of the plantar fascia as it inserts into anterior calcaneus. Pain is worse upon getting out of bed in the morning is almost pathonmeumonic. Often associated with a bony exostoses on calcaneus i. e. a “spur”. Tx: Ice, NSAIDS, Stretching, arch supports Responds very well to local steroids.
Plantar Fasciitis 162 3/5/2021
Plantar Fasciitis – Treatment Stretching exercises Prefabricated, OTC, shoe heel inserts Rest Short course (2 – 3 weeks) NSAID If the above fail (3 -4 weeks no improvement) try glucocorticoid + anesthetic injection
Fractures of the Foot Forefoot Metatarsal and phalanges Midfoot Navicular, cuboid, cuniform Hindfoot Talus, calcaneus Lisfranc joint separates the forefoot from the midfoot Chopart joint divides the hindfoot from the midfoot
Mechanism of Injury Talar neck Forced dorsiflexion usually from a fall or MVC Lateral aspect of talus Snowboarding Calcaneus Fall >3 m landing on the heel, MVC Cuboid Fall, usually associated with talar, calnaeus or metatarsal fractures Tarsometatarsal (Lisfranc) Violent plantar flexion and/or abduction usually from falling from significant height
Treatment Emergent ortho consult with Open fracture Compartment syndrome Vascular compromise Urgent ortho consult Talar nec fracture Intrarticular calneus fracture Lisfranc fracture Generally RICE, analgesia
Metatarsal Fracture Most common foot fracture N/V assessment very important Assess overlying skin condition Palpate Lisfranc complex and refer if in doubt Displaced or unstable first metatarsal require ortho referral Fractures of 2 -5 metatarsal usually don’t require reduction or casting unless displaced > 3 -4 mm
Morton’s Neuroma Thought to be due to swelling and scar formation on the small interdigital nerves May complain of pain and/or numbness exacerbated by activity Usually affects the 3 rd interdigital space but may be in the 2 nd and 4 th Palpation may reproduce pain. Mulder’s sign is a clicking sensation when palpating the interspace while compressing the metatarsal joints Conservative treatment should precede diagnostic procedures U/S is an inexpensive imaging option
Musculoskeletal Exam Summary Good Hx: Trauma, Constitutional Sx, Red flags, restrained in MVC? Good PE: Inspect Palpate what hurts gently! ROM active and passive Neurovascular exam Good workup: radiography if indicated
References Patel, Nina H. , Holman and John R. Overuse or injury: is it Tendonitis or Bursitis? Consultant April 1, 2008 Bol. 48 No. 4, pages 314 to 320. Provenzano, David A. and Levin, Morris. Chronic Pain Syndromes: How to break the cycle, Part 1, Consultant April 1, 2008 Bol. 48 No. 4, pages 297 to 304. Seidel, Ball, Davis and Benedict. Mosby’s Guide to Physical Examination Fourth Edition. Benson, Leon S. Orthopedic Pearls. Hoppenfeld, Stanley. Physical Exam of the Spine and Extremities. Appleton-Century. Crofts 1976. Bickley, Lynn S. and Szilagyi, Peter G. Bates’ Guide to Physical Examination and History Taking Ninth Edition Lippencott Williams & Wilkins 2007. Dr. Samuel Cleveland, Barry University PA Program Medical Director Tintinalli, Ruiz, and Krome. EM 4 th edition. Tierney, Mc. Phee, Papadakis. Current Medical Dx&Tx 2002.
References • • Larson, Betty and Kuntz, Susan. Dx and Pharm management of Back Pain. JAAPA, 25(3) March 2012. Koehler SM, Fields KB, Grayzel J. AC joint injuries in Upto. Date 2012 Hsu PS, Armon C, Levin K. Lumbosacral radiculopathy in Upto. Date 2012. Topic 5262 Version 9. 0 Maughan KL, Upto. Date 2012 Topic 189 Version 9. 0 Schiff D. Upto. Date 2012. Topic 2819 Version 4. 0 Sherman. Shraider. Shoulder dislocation and reduction Uptodate 2012. Topic 258 Version 8. 0 Burroughs KE. Scaphoid fractures. Uptodate Topic 197 Version 11. 0. 2012 Dr. Armstrong, lecture slides Kienstra AJ, Macias CG. Ossgood Shlatter Disease. Up to date Topic 6289 Version 7. 0 2012 Isolated clavicle fracture with secondary pneumothorax, Hong Kong Journal of EM Upto. Date. Topic Causes of limp in children 6460 Version 11. 0 Upto. Date Approach to child with bow-legs Topic 6285 Version 11. 0 Up. To. Date Pelvic trauma: Initial evaluation and management Wendy Langen, lecture content Albert Armstrong- shoulder X rays SA Landaw, KA Bauer. Uptodate, 2015 Topic 1322 Version 33. 0