Assessment of the Chest and Lungs Anatomy w





 diameter")




 Ø Ø Ø Place both thumbs at about 7")








/")






 disease gradually destroys the lungs. This")
 is a disease caused by bacteria called Mycobacterium tuberculosis. w")

 Cough Shortness of breath Chest")










- Slides: 42
Assessment of the Chest and Lungs
Anatomy w Anatomy of the respiratory system is available on blackboard as an online lecture.
Subjective Data w w w Cough Shortness of breath Past history of respiratory infections Smoking history Environmental exposures Self care habits
Physical Examination Equipment and Techniques w Equipment Ø Stethoscope w Techniques Ø Ø Inspection Palpation Percussion Auscultation
Inspection w General Ø Ø Appearance Posturing Breathing effort Trachea position l Midline
Inspection w Chest Wall Configuration Ø Ø Form Symmetry Muscle development Anterior-Posterior (AP) diameter l l Ø Approximately ½ the transverse diameter Transverse: Anterior-Posterior = 2: 1 Costal angle l 90 degrees or less
Inspection w Oxygenation: cyanosis Ø Ø Ø Nails Skin Lips w Respiratory Effort Ø Ø Ø Respiratory rate and depth Breathing pattern Chest expansion
Abnormal Breathing Patterns Kussmaul
Abnormal breathing patterns w Hypoventilation Ø Ø Ø Slow, shallow breathing Causes CO 2 to build up in the blood Acidosis w Hyperventilation Ø Ø Ø Rapid, deep breathing Causes CO 2 to be blown off Alkalosis
Palpation Tactile Fremitus: Do you know where it is the greatest? w Increased: in periphery with consolidation or compression of lung tissue. Ex lobar pneumonia w Decreased: When anything obstructs transmission of vibrations: Ex. Pleural effusion, pneumothorax or emphysema
Palpation w Thoracic Expansion (Excursion) Ø Ø Ø Place both thumbs at about 7 th rib posteriorly along the spinal process Extend the fingers of both hands outward over the posterior chest wall Have the person take a deep breath and observe for bilateral outward movement of thumbs l l Normal: bilateral, symmetric expansion Abnormal: unilateral or unequal Click on the pictures to view video
Percuss w If you suspect over inflation or consolidation w Sound depends on the air-tissue ratio w Resonance: normal lung fields w Hyperresonance: Overinflated lung w Dull tone: consolidation
Auscultation Auscultate in a systematic manner Compare one side to the other Listen one full respiration at each spot Compare bilaterally Displace breast tissue to listen directly over chest wall w DO NOT listen through gowns, clothes, etc. w w w Ø Place your stethoscope over bare skin
Auscultation w Know where the lungs are!! w Assess both anterior and posterior every time w Ask patient to lean forward slightly, with arms resting in lap w Ask them to breath in through mouth, a little deeper than normal w Move from the apices to the bases
Copyright © 2013 by Mosby, an imprint of Elsevier Inc. 15
Auscultation Use the diaphragm of the stethoscope
Auscultation w Evaluate for normal sounds Sound Pitch Intensity Quality I: E Location Bronchial High Loud Blowing/ hollow I<E Trachea Bronchovesicular Moderate Combination I=E Between scapulae, 1 st & 2 nd ICS lateral to sternum Vesicular Low Soft Gentle rustling/ breezy I>E Peripheral lung
Copyright © 2013 by Mosby, an imprint of Elsevier Inc. 19
Auscultation w Evaluate for adventitious sounds Sound Intensity/ Pitch I/E Crackles/ Rales Soft (fine)/ High Loud (coarse)/ Low Wheeze Ronchi Pleural Friction Rub Stridor Quality Clear with Cough I Discontinuous, nonmusical, brief Possibly High E Continuous musical sounds Possibly Low E Continuous snoring sounds Possibly Continuous or discontinuous creaking or brushing sounds Never Continuous, crowing Never I&E I
Hemothrorax w Blood in the pleural space w Chest injury or thoracic surgery w Short of breath, anxious, chest pain, respiratory distress, dyspnea, tachypnea, cyanosis. w Muffled breath sounds and dullness over affected area.
Atelectasis w Collapsed alveoli w Caused by external pressure from Ø Tumor, fluid, air in the pleural space Ø Lack of air from hypoventilation or obstruction of secretions w Diminished or absent breath sounds w O 2 sat <90
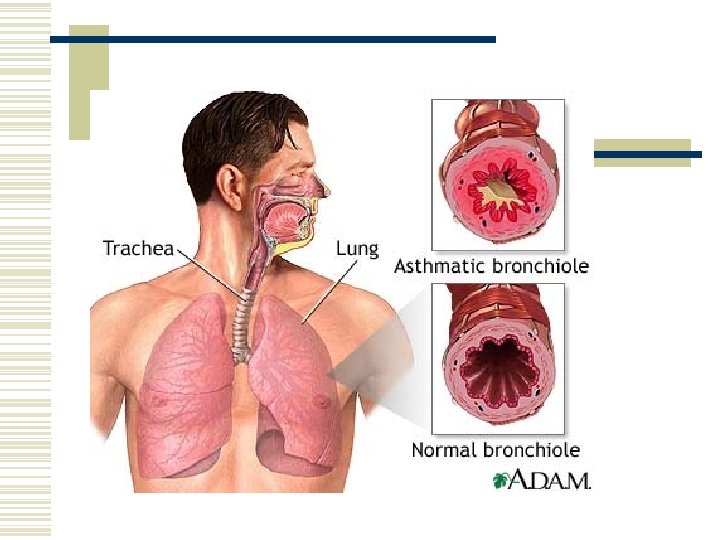
Asthma – What is It? w Asthma is a chronic lung disease that obstructs airflow w The obstruction is reversible w It involves difficulty in breathing due to Ø Inflammation (swelling) Ø Mucus in the airways Ø Tightening of muscles around the airways
Bronchitis • • Most prevalent in winter Signs and Symptoms Generally part of an acute URI 1. Malaise 2. Chilliness It may develop after a common cold or other viral infection of the nasopharynx, throat, or bronchi 3. Slight fever 4. Back and muscle pain 5. Sore throat 6. Onset of a distressing cough usually signals onset of bronchitis 7. Cough starts off dry and later produces mucous. Often with secondary bacterial infection
Pneumonia w Symptoms • • • Fever Tachypnea Dyspnea Crackles Wheezes - Pneumonia occurs when bacteria (most commonly Streptococcus pneumoniae), chemical irritants, or viruses get into your lungs. - Pneumonia causes the alveoli in the lungs to fill with pus or other liquid. This causes difficulty in breathing
Pneumonia w Most deadly infectious disease in the U. S. w 6 th leading cause of death
Emphysema w Emphysema : Ø Ø chronic (long-lasting) disease gradually destroys the lungs. This destruction means unable to breathe in enough oxygen. Ø You also have trouble breathing out carbon dioxide. Ø
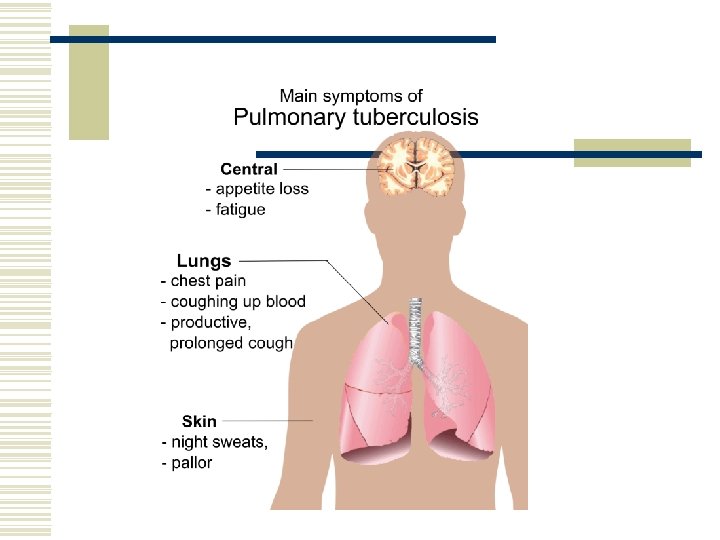
Tuberculosis w Tuberculosis (TB) is a disease caused by bacteria called Mycobacterium tuberculosis. w ► The TB bacteria can affect any part of the body, but usually affects the lungs. w ► If not treated properly, a person who has TB infection can develop TB disease. w ► If a person develops TB disease and does not get appropriate medical treatment he/she can die.
Lung Cancer w • Lung cancer is the #1 cause of cancer-related deaths by far in the U. S. …more than breast, prostate, and colon cancer combined. Smoking (90% of all cases) • Second-hand smoke (25% of non-smoker cases) • Occupational/environmental
Lung Cancer Symptoms w w w w Fatigue (tiredness) Cough Shortness of breath Chest pain Loss of appetite Coughing up phlegm Hemoptysis (coughing up blood) If cancer has spread, symptoms include bone pain, difficulty breathing, abdominal pain, headache, weakness, and confusion
Developmental Variations w Neonates Ø Measure the chest circumference l l Ø Ø Usually 2 -3 cm smaller than head circumference Chest is round (i. e. AP diameter = transverse) Obligate nose breathers Periodic breathing is common l l Sequence of vigorous breathing followed by apnea for 10 -15 seconds Only concern if it is prolonged or baby becomes cyanotic
Developmental Variations w Neonates Ø Ø Breathing is diaphragmatic and abdominal Signs of compromise l l Stridor (“crowing”) Grunting Central cyanosis Flaring nares
Developmental Variations w Infants and Young Children Ø Ø Roundness of the chest persist for first 2 years Chest walls are thinner than the adult’s l Breath sounds may sound louder, and more bronchial than the adult w Bronchovesicular sounds may be heard throughout the chest
Developmental Variations w Pregnancy Ø Ø Ø Costal angle increases to about 105 degrees in the third trimester Dyspnea and orthopnea are common Breathes more deeply
Developmental Variations w Older Adult Ø Ø Ø Chest expansion is often decreased Bony prominences are marked AP diameter is increased with respect to transverse (but not 1: 1)
Videos of Thorax and Lung Assessment Ø Ø Inspection l General appearance l Posture l Breathing effort Posterior Thorax l Inspect: shape, symmetry l Palpate: tenderness and Tactile fremitus l Thoracic expansion l Tell me percussion would be performed if you suspected overinflation or consolidation of the lungs l Auscultate lungs bilaterally
Videos of Thorax and Lung Assessment Anterior Chest Ø Inspect: Respirations Ø Palpate for tenderness and tactile fremitus Ø Ausculate breath sounds Bilaterally
Videos of Thorax and Lung Assessment
Conclusion w Today you learned Ø Ø Ø How to complete a physical examination of the respiratory system Identify normal and abnormal variations Common Problems with the respiratory system Age related variations. What is expected for your video.
Lab w Bring your stethoscope, pen, textbook w You will be Practicing listening to breath sounds w You will also be practicing your respiratory exam on your partner using the lab guide I will provide you with. w It is highly recommended that you record the video the week that you learn the material.