MAXILLOFACIAL TRAUMA Cerrahpaa Tp Fakltesi Plastik Rekonstrktif ve






")





 zygoma maxilla mandibula")
 fractures • Pure ( intact orbital rim) •")
 Fracture • Clinical findings – Periorbital hemorrhage- ecchymosis and subconjunctival hemorrhage")
 paralysis")







 condyle ve subcondylar fracture kırık hattının yanında")






- Slides: 35
MAXILLOFACIAL TRAUMA İ. Ü. Cerrahpaşa Tıp Fakültesi Plastik, Rekonstrüktif ve Estetik Cerrahi Anabilim Dalı Dr. Hakan Arslan
Maxillofacial trauma • Soft tissue injuries • Soft tissue with bone fractures • Bone fractures
Etiology • Traffic accidents • Assault • Sport injuries • Domestic accidents • Industrial accidents • Gunshot wounds
Primary survey Ⓐ Airway maintenance with cervical spine control Ⓑ Breathing and ventilation Ⓒ Circulation with hemorrhage control Ⓓ Disability assessment of neurological status Ⓔ Exposure and complete examination of the patient 8
Priority in Maxillofacial injuries • Airway maintenance – clearence of blood, teeth or vomit from oropharynx – Aspiration – Tracheostomy
Priority in Maxillofacial injuries • Hemorrhage Control – Direct pressure – Ligation of vessels (A. Facialis, A. Temporalis Superficialis, A. Angularis, A. Carotis Externa) – Antero-posterior nasal tamponade – Embolization of vessel
Priority in Maxillofacial injuries • Assessment of concomitant injuries (cervical, cranial, thoracic, abdominal injuries) • Assessment of facial trauma
Tracheostomy Indications in Maxillifacial Injuries • Panfacial fracture • multi fragment mandibular fracture associated with significant edema of oral floor and neck • maxillofacial trauma requires intermaxillary fixation • concomitant thoracic and intracranial injury
Tracheostomy Indications in Maxillifacial Injuries • Head and Neck burn injury • Occlusion of larynx and hypopharynx • Possibility of long duration of airway problem after operation
Clinical Findings • soft tissue injury • crepitus, pain and mobility of underlying bone part • paresthesia or anesthesia • paralysis of motor nerve • Malocclusion • ocular injury – Diplopia and/or decreased visual acuity • facial asymetry or deformity • intra oral laceration • Nasopharengeal hemorrhage
Soft tissue Injuries superficial/deep simple/complex special zones eyebrow eyelids lips nose special tissue facial nerve facial muscles
12
Facial Fractures nose orbital (floor-roof) zygoma maxilla mandibula
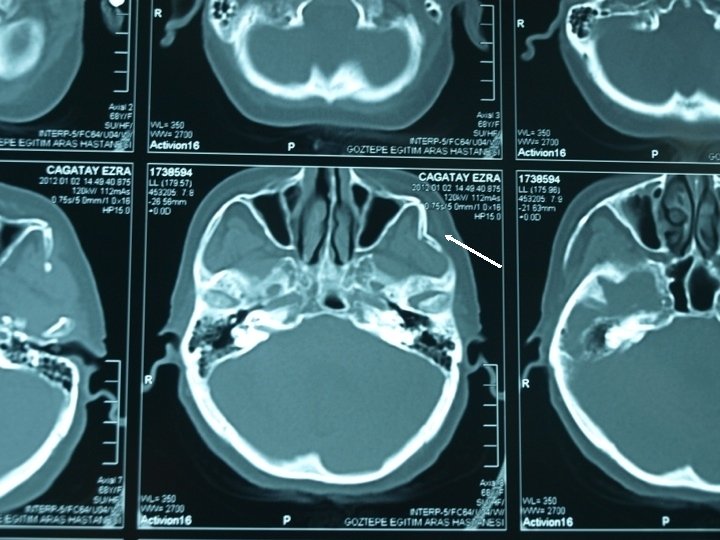
Orbital Fractures – Orbital floor (blow-out) fractures • Pure ( intact orbital rim) • Inpure (with orbital rim fracture) – Orbital floor fracture without blow out • Linear fractures • with maxillary fractures • orbital floor fracture with only zygomatic part
Orbital Floor (Blow-out) Fracture • Clinical findings – Periorbital hemorrhage- ecchymosis and subconjunctival hemorrhage – İnfraorbital nerve damage- paresthesia, anesthesia – Diplopia – Enophtalmos – Positive Forced duction test (+) – CT scan confirmation of fracture and herniation of orbital contents into maxillary sinus
Superior Orbital Fissure Syndrome ve Orbital Apex Syndrome • N. Occulomotorus (CN III) paralysis (levator, superior rectus, medial rectus, inferior rectus ve inferior oblique muscle) • N. Trochlearis (CN IV) paralysis (superior oblique muscle) • N. Abducens (CN VI) paralysis (lateral rectus muscle) • Trigeminal nerve (CN V) ophtalmic branch- anesthesia (upper eyelid, eyebrow, upper nose area, ipsilateral frontal zone) • N opticus involvement ----- Orbital Apex Syndrome
Nasoethmoidoorbital Fracture • clinical findings – Telecantus – decreased dorsal nasal projection – rhinorrhea
Tip 1 Tip 3 Tip 2 Classification of Nasoethmoidoorbit al Fracture
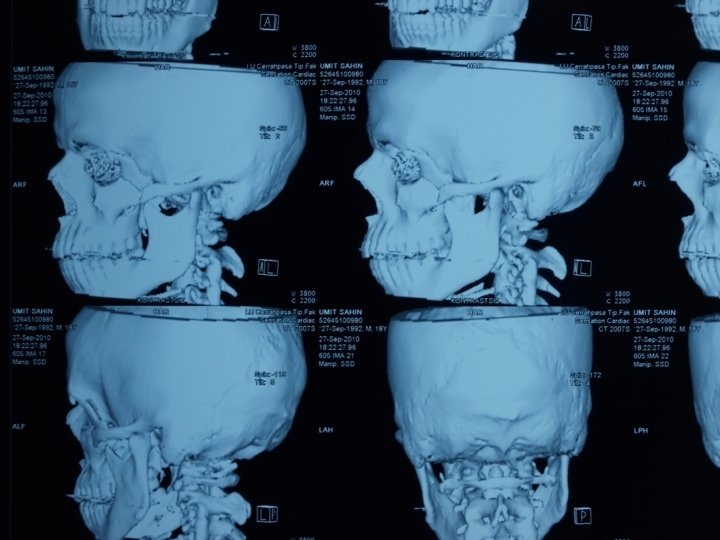
Maxillary Fractures Le Fort Le. Fort I fracture is a horizontal maxillary fracture across the inferior aspect of the maxilla and separates the alveolar process containing the maxillary teeth and hard palate from the rest of the maxilla. Le. Fort II fracture is a pyramidal fracture starting at the nasal bone and extending through the ethmoid and lacrimal bones; downward through the zygomaticomaxillary suture; continuing posteriorly and laterally through the maxilla, below the zygoma; and into the pterygoid plates. Le. Fort III fracture or craniofacial dysjunction is a separation of all of the facial bones from the cranial base with simultaneous fracture of the zygoma, maxilla, and nasal bones.
Maxillary Fractures – Periorbital hemorrhage – Nasopharengeal hemorrhage – facial edema – intaoral lacerations – Maloclussion – Facial elongation – Maxillary retrution – Anterior open bite – Maxillary dental arch mobility – Rhinorrhea (Le Fort II ve III % 250
Zygoma Fractures Classification 6 type usually tripod fracture isolated zygoma archus fracture usually concomitant with orbital and maxillary fracture
Tripod Fracture
Zygoma Fracture Clinical findings malar depression and flattening subconjunctival hemorrhage periorbital eccyhmosis- edema no maloclussion paresthesia-anesthesia (inferior orbital nerve)
Mandibula Fractures Classification anatomic region (most common) condyle ve subcondylar fracture kırık hattının yanında diş olup olmaması dişlerin olup olmaması (edontolous)
Body 30 -40 % Angle 25 -30 % Condyle 15 -17 % Symphysis 7 -15 % Ramus 3 -9 % Alveolar 2 -4 % Coronoid Process 1 -2 %
Mandibular Fractures In almost every mandibular fracture Pain during opening-closing the mouth Malocclusion
Facial Fractures in Children • Features – older than 5 years old – the most common subcondylar fracture – Pediatric bones are cancellous and soft, may displaced without fracture – Bone healing is faster after fracture. reduction of bones is quite difficult after 1 week.
Facial Fractures in Children Little deformities can be corrected spontanously due to the adaptive potential of the alveolar bone and the permanent teeth eruption due to the mixed dentition, open reduction and rigid fixation should be done carefully. intermaxillary fixation is quite difficult because of the superficial localization of the teeth roots Paranazal sinüsler küçüktür
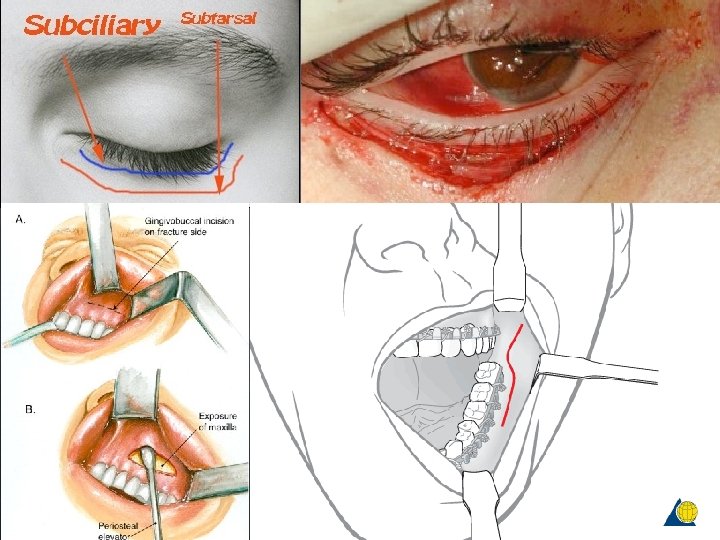
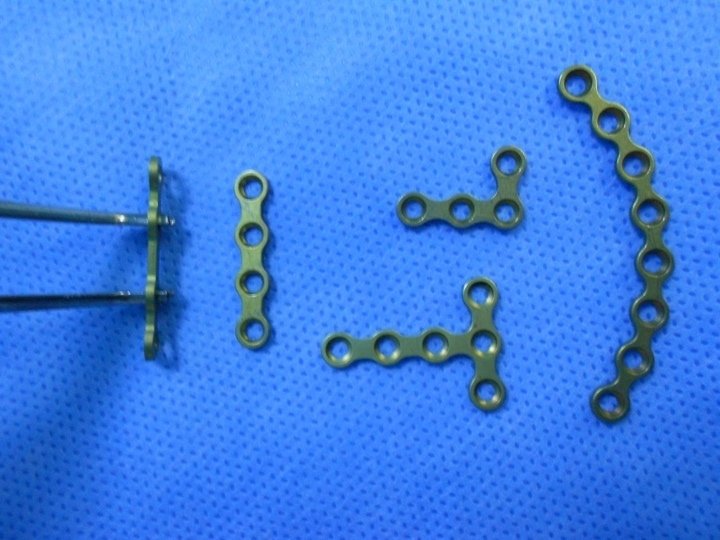
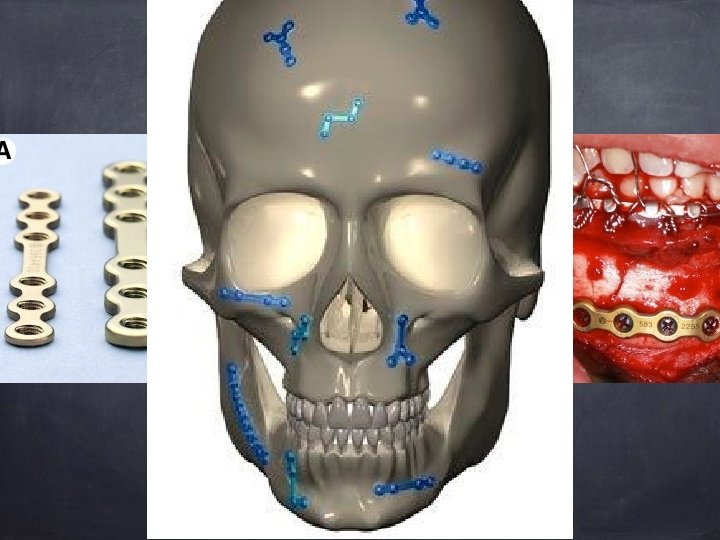
Treatment open reduction- internal fixation mini plates- screws cerkilage wires Basic principles fixate butresses establish occlusion normal facial contour maintaine globe position
TEŞEKKÜR EDERİM