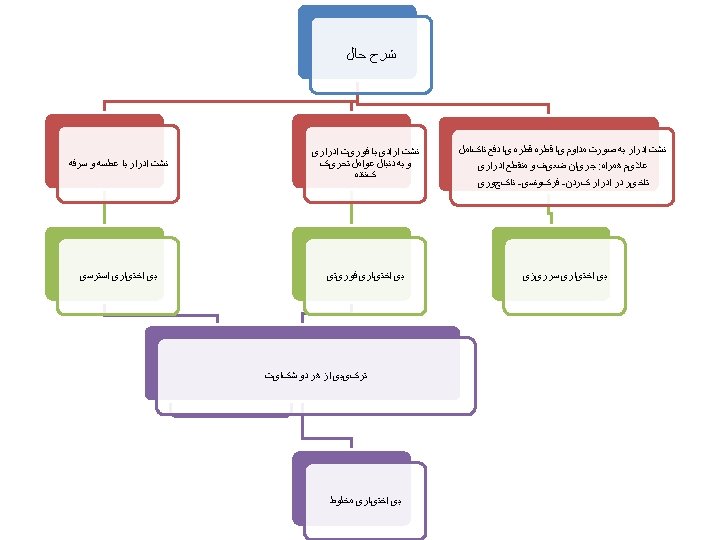
SUI The involuntary leakage of urine on effort













 : • Kegle exercises strengthen the muscular urethral closure mechanism.")








 TVT (Tenstion – Free Vaginal Tape) SUI ﺟﺮﺍﺣی ﺍﻧﻮﺍﻉ")

















 • urgency")









- Slides: 87
** SUI : The involuntary leakage of urine on effort or exertion or on sneezing or coughing. * Affects 4%-35% of women.
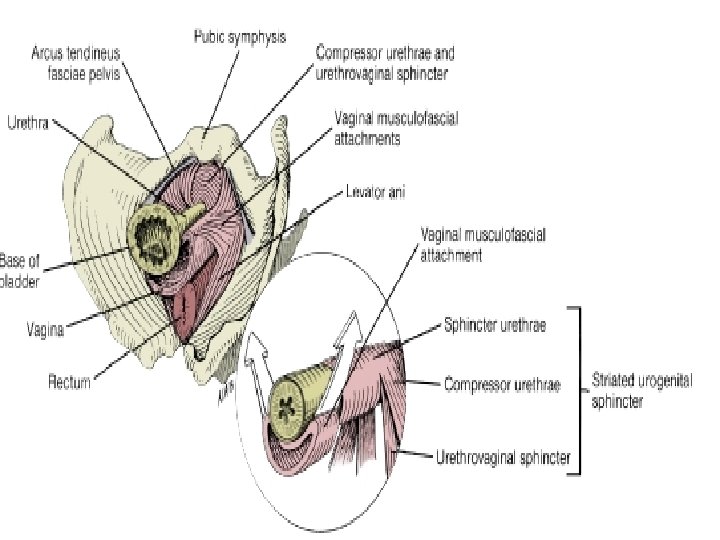
** Continence: * is achieved when the urethra maintains a pressure greater than bladder pressure. (during a detrusor muscle contraction or an increase in intraabdominal pressure)
Etiology 1 -- Pregnancy, child birth 2 – Aging 3 -- Repetitive stress on the pelvic floor 4 --Genetic factor (deficient collagen structure)
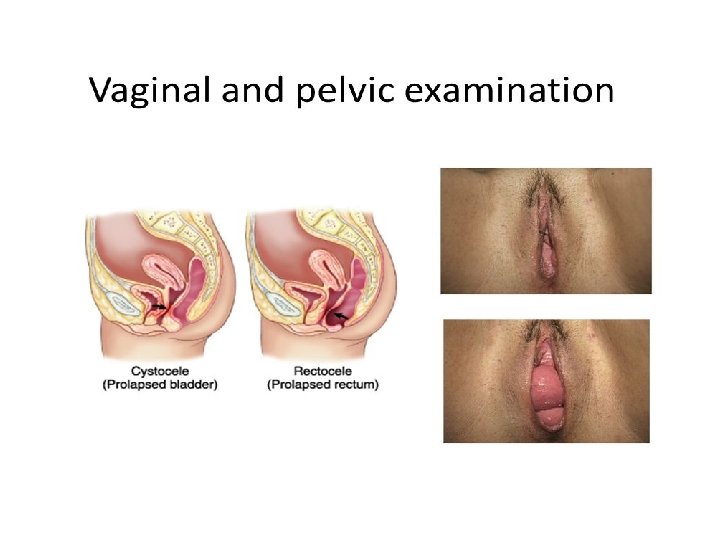
Clinical Evaluation
*** Bladder Diary: * Particularly in patients in whom the etiology of urinary incontinence is UNCERTAIN.
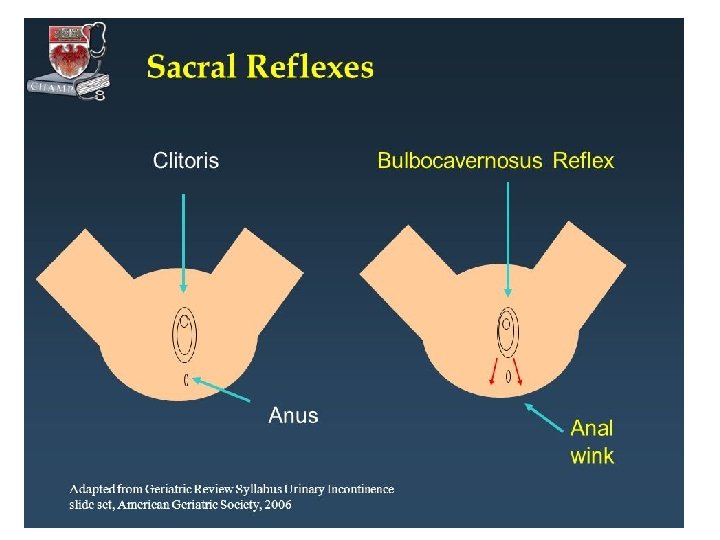
Detailed neurologic examination ? ? ?
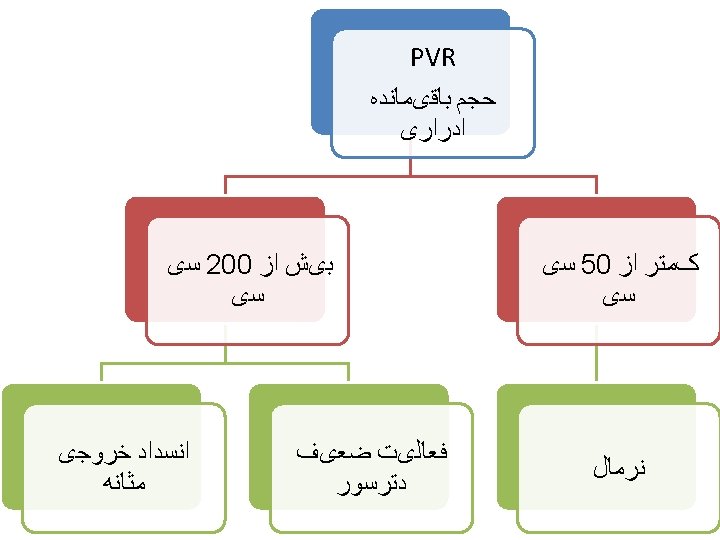
Post void Residual Volume ? ? ?
Laboratory tests FBS U/A , U/C
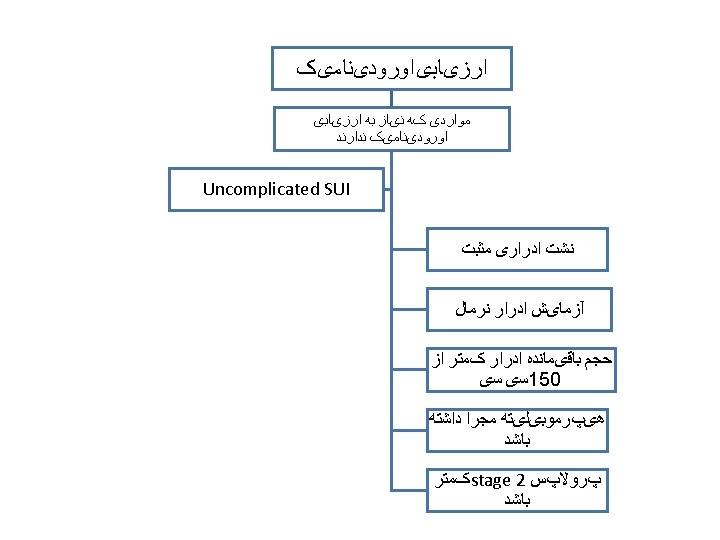
Level A • Preoperative UDS is not necessary before planning primary anti – incontinence surgery in women with uncomplicated SUI : • • 1 - defined as PVR less than 150 ml 2 – negative UA 3 – a positive cough stress test 4 – no pelvic organ prolapse beyond the hymen • ACOG 2015
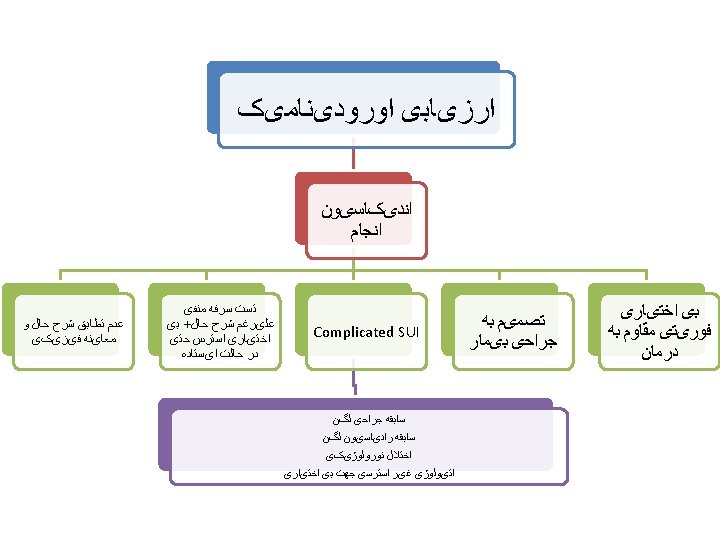
* UDS does not improve treatment outcomes in women with uncomplicated SUI prior to midurethral sling surgery. ** women with uncomplicated SUI in whom conservative treatment has failed and who desire midurethral sling surgery, UDS does not affect treatment outcomes.
** Mixed urinary incontinence does not impact the choice of surgical procedure. these women should undergo a trial of pharmacologic therapy prior to surgery. ** Occult SUI, can usually be diagnosed by repeating the urinary stress test while the prolapse is reduced by the examiner. there is no evidence that UDS is required to detect occult SUI.
Treatment
Level B • Incontinence pessaries may improve the symptoms of stress and mixed urinary incontinence but objective evidence regarding their effectiveness has not been reported. • When SUI is demonstrated during cough test : an increased rate of SUI after pelvic organ prolapse surgery is expected. ACOG 2015
Pelvic muscle exercises (PME) : • Kegle exercises strengthen the muscular urethral closure mechanism. ( grade 2 A )
Local topical Estrogen: • There is inconsistent evidence whether local topical estrogen ( cream , ring , dissolving tablets) improves incontinence symptoms. ( grade 2 C) * Randomized trials have demonstrated that Oral Estrogen worsen urinary incontinence. Up to date 2017
Surgical trearment
1 -- Women who decline or have persistent symptoms following conservative therapy • Surgical treatment have consistently been shown to have a higher efficacy rate than conservative therapy. *Surgery is associated with increased morbidity , postoperative voiding difficultly & development or worsening of urgency incontinence.
2 -- Women with occult SUI : *Concomitant anti-incontinence surgery is warranted in some women who are undergoing repair of advanced pelvic organ prolapse
3 -- Women finished with childbearing : * Since pelvic support may be disrupted during pregnancy and particularly a vaginal birth , most physicians recommend delaying surgical management of SUI until childbearing has been completed.
Pre operative counseling • Patient & surgeon satisfaction with treatment can be optimized by having a discussion during the planning phase for the surgery about the individual patient goals & expectations for her treatment & awareness of potential adverse events.
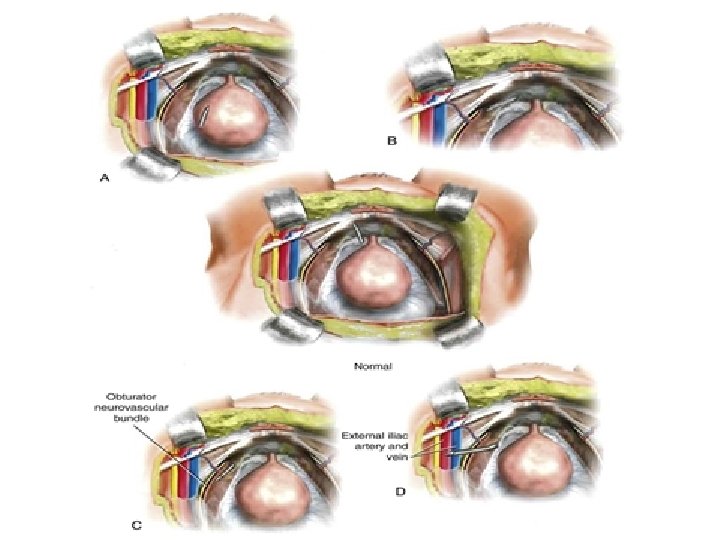
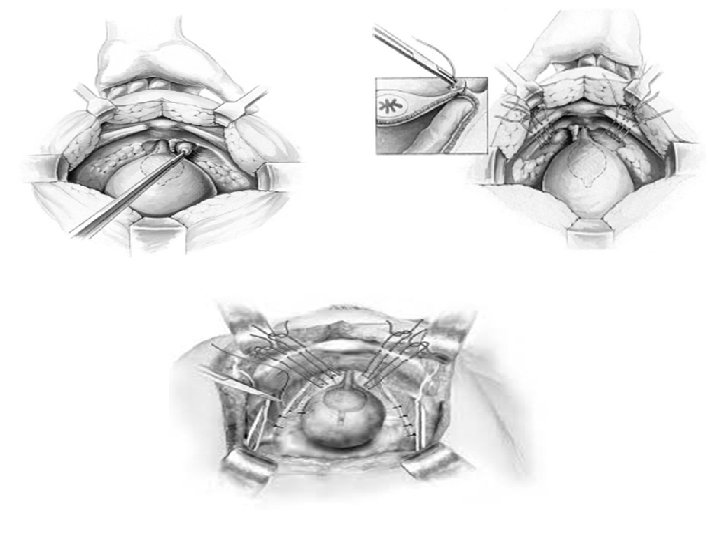
• Suburethral sling : A suburethral sling is a sling that is inserted through a small vaginal incision and placed either at the bladder neck, midurethra or proximal urethra. 1 - Bladder neck sling : A suburethral sling that is placed at the level of the proximal urethra and bladder neck 2 - Midurethral sling : A suburethral sling that is placed at the level of the midurethra in a tension free manner (eg, tension-free vaginal tape procedures). 3 - Retropubic colposuspension : Procedures performed through laparotomy or laparoscopy in which the vaginal wall adjacent to the midurethra and bladder neck is suspended, using sutures, in a retropubic position
TOT (Transe obturator Tape ) TVT (Tenstion – Free Vaginal Tape) SUI ﺟﺮﺍﺣی ﺍﻧﻮﺍﻉ Burch Fascial Sling
Level A • Initial midurethral sling surgery results in higher 1 – year subjective and objective cure rates than pelvic floor physical therapy in women with SUI. • MUS demonstrate efficacy that is similar to traditional suburethral fascial slings – open colposuspension and laparoscopic colposuspension. • Compared with suburethral fascial slings: fewer adverse events have been reported with MUS. ACOG 2015
Level A • Voiding dysfunction is more common with open colposuspension than with MUS. • There are substantial safety and efficacy data that support the role of MUS as a primary surgical treatment option for SUI in women. ACOG 2015
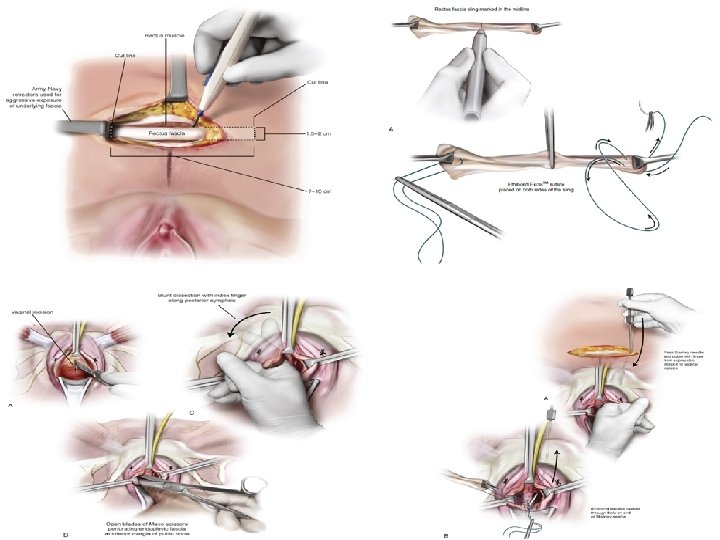
Surgical Technique 1. antibiotic administration. 2. Sterile urine 3. Patient positioning and preparation.
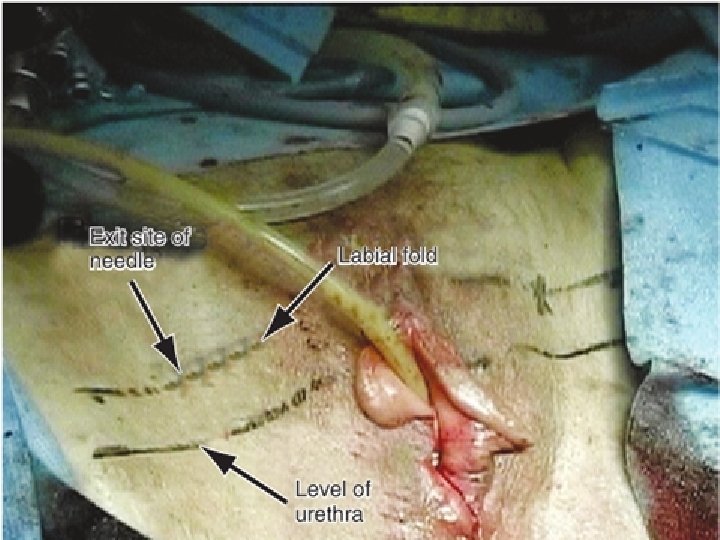
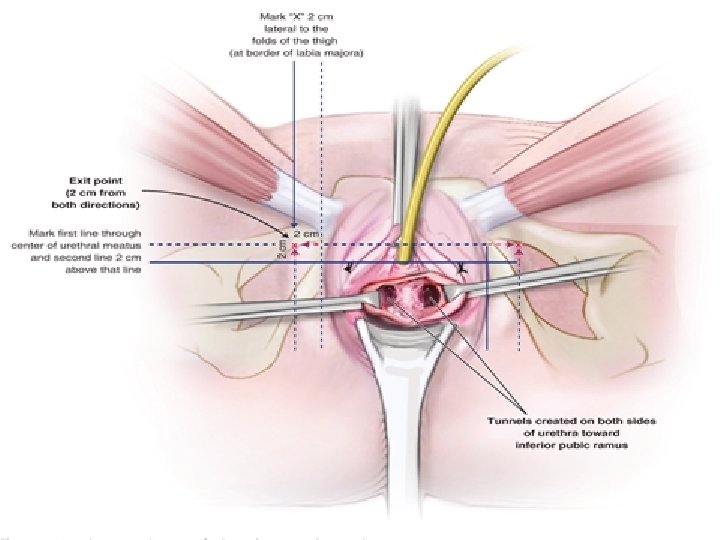
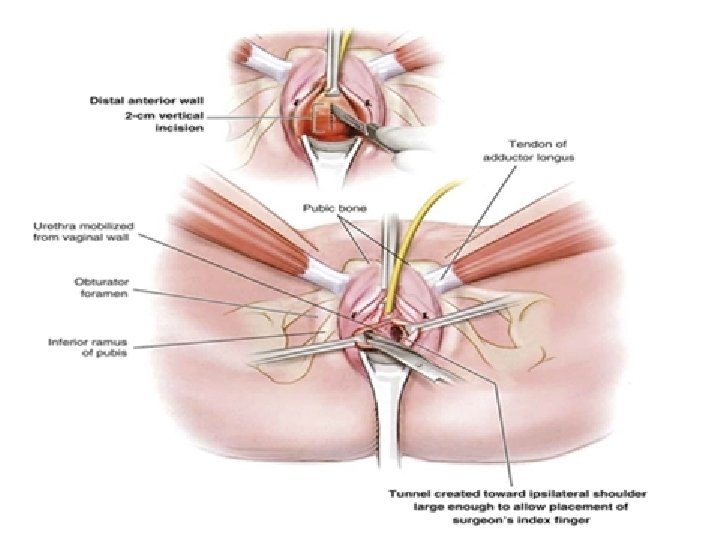
4. Anesthesia. 5. The exit site of the needle is marked. It should be 2 cm above the level of the urethra and 2 cm lateral to the labial fold.
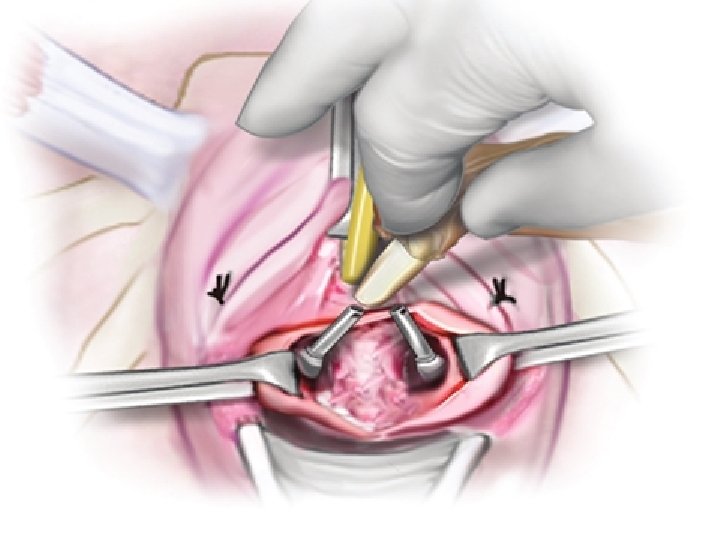
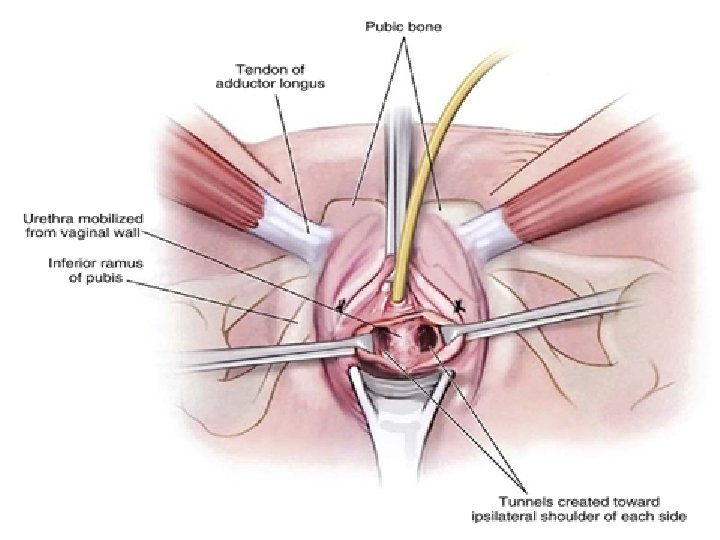
6. Vaginal incision. 7. Vaginal dissection
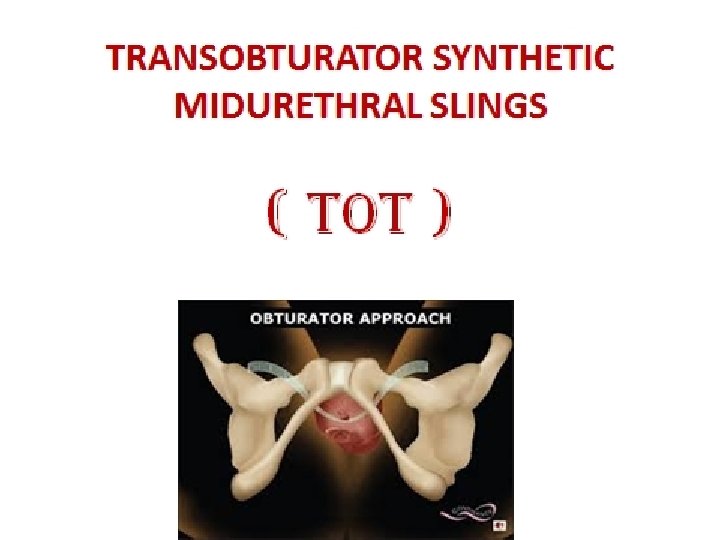
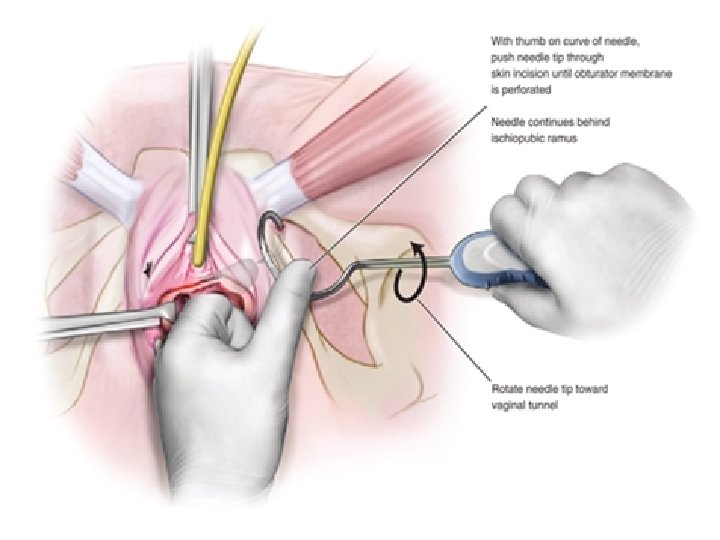
CHOOSING A TYPE OF TRANSOBTURATOR SLING ●Inside-out – The trocars are passed from a midurethral vaginal incision to exit through bilateral groin incisions (TVT Transobturator, often abbreviated as TVT-O). ●Outside-in – The trocars are passed from bilateral groin incisions to exit through a midurethral vaginal incision (Monarc, often abbreviated as TOT).
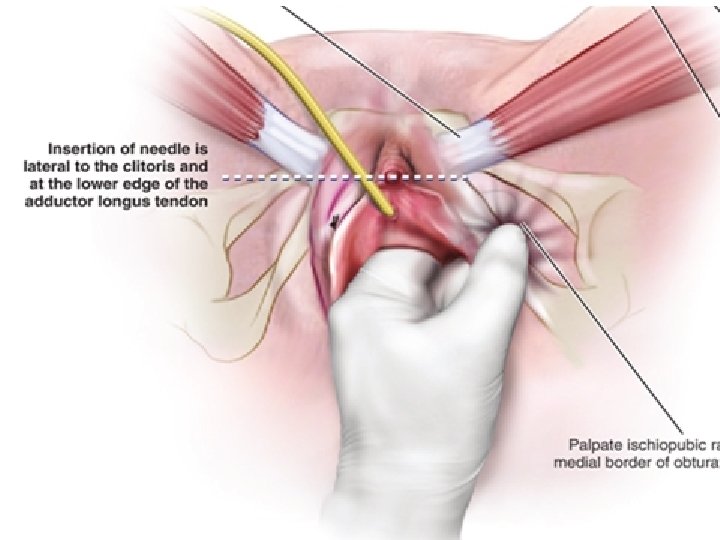
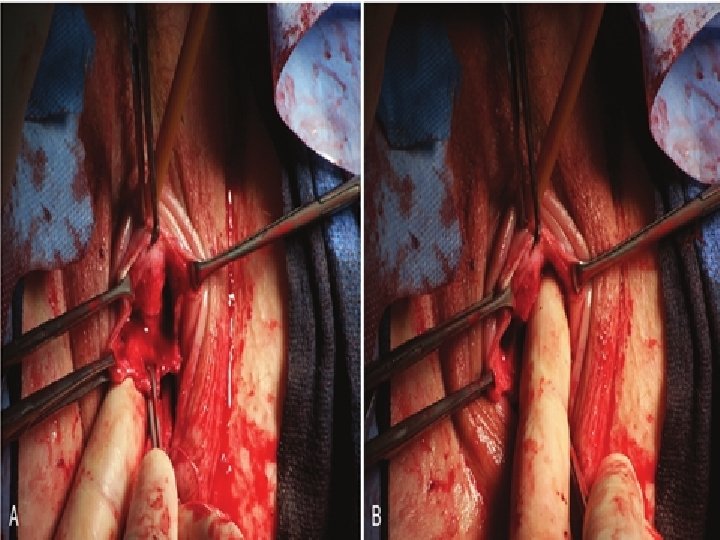
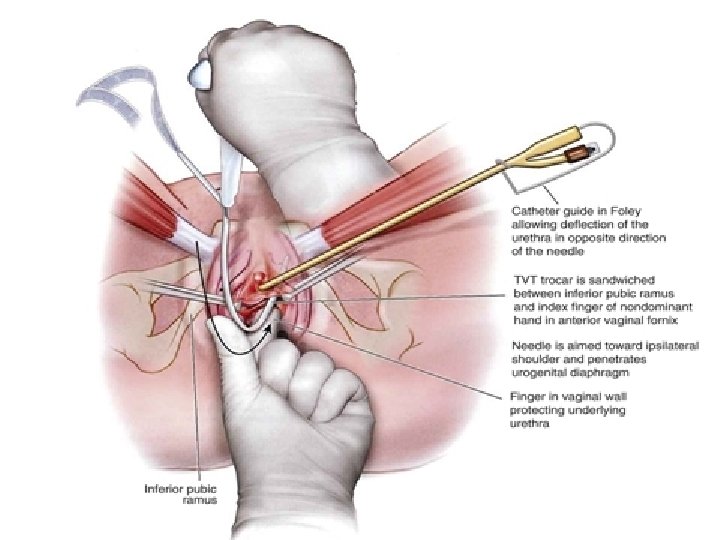
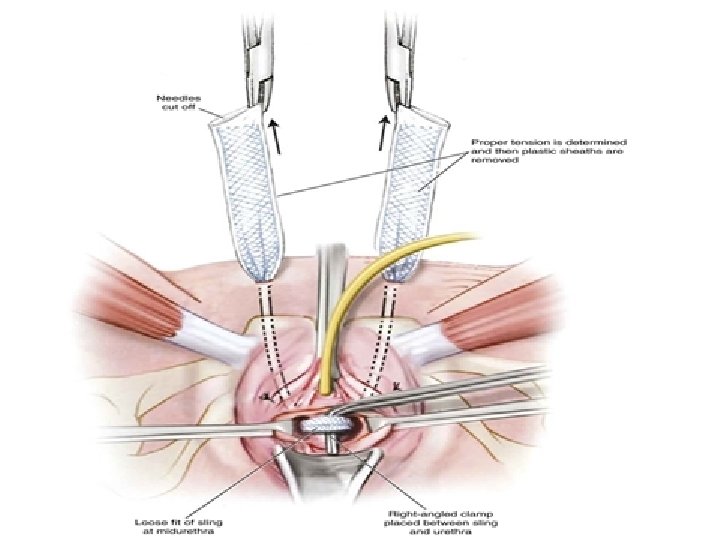
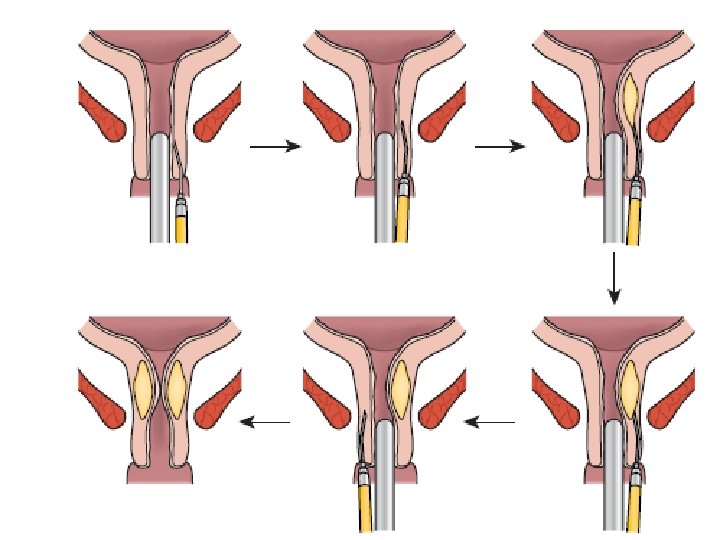
8. Trocar passage The trocar tip is inserted into the previously dissected vaginal incision lateral to the urethra and advanced gently while rotating the trocar handle.
• The two types of transobturator procedures appear to be equally effective and have similar complication rates • One disadvantage of the outside-in approach is that it results in a larger vaginal incision and has a higher rate of vaginal perforation. • some data suggest that the inside-out approach is more likely to cause groin pain, but this finding has varied across studies.
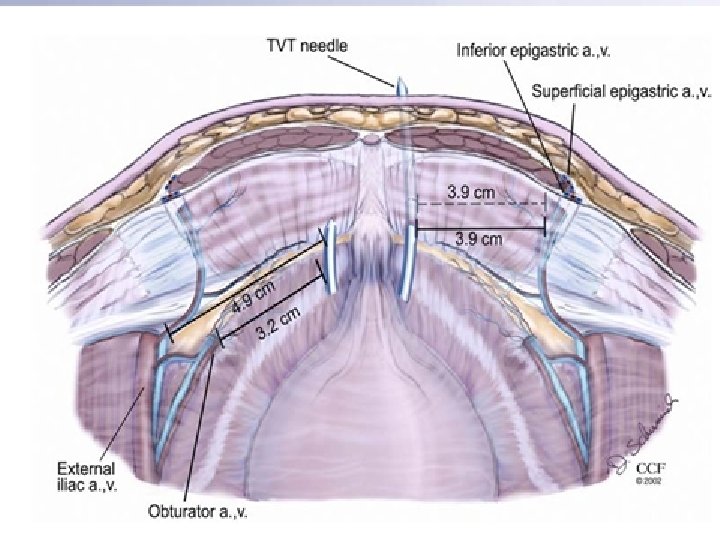
COMPLICATIONS • Transobturator insertion of midurethral slings was developed to avoid some of the complications of retropubic slings (eg, bladder perforation, vascular injury, bowel injury). • This appears to have been largely successful and few serious or long-term complications have been reported following transobturator midurethral sling procedures.
FOLLOW-UP • Women may experience vaginal, periurethral, or lower abdominal discomfort and pain at incision sites for up to two weeks following the procedure. • These symptoms are typically well controlled with oral narcotics and non-steroidal anti inflammatory drugs. • Many women also have vaginal spotting for up to two weeks.
• Patients are advised to avoid heavy lifting, actions that increase intraabdominal pressure, or exercise for at least two to four weeks. • Ambulation, however, is encouraged. • Sexual activity should be avoided until the vaginal epithelium is healed, which takes approximately four to six weeks. • The patient may return to work when she feels sufficiently comfortable.
• We see patients for a routine follow-up visit at four to six weeks. • We perform abdominal and vaginal examinations to ensure that the incisions have adequately healed and to check for vaginal mesh erosion. • We check a post void residual volume to assess whether the patient has been adequately emptying her bladder. • This can be measured with a bladder ultrasound or catheterization.
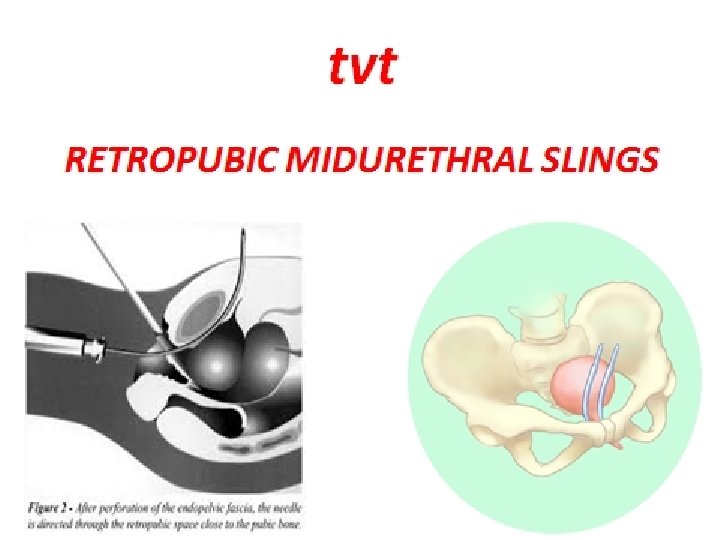
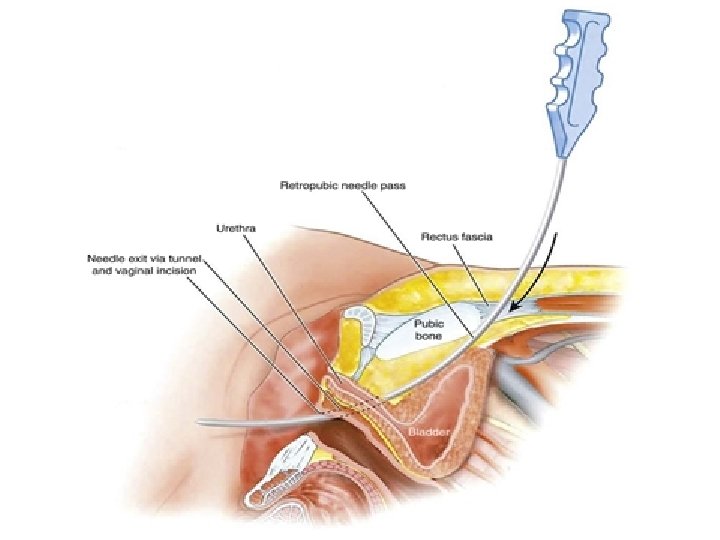
CHOOSING A TYPE OF RETROPUBIC SLING ●Bottom-to-top – Two needle trocars are inserted through a vaginal incision and passed through the retropubic space, exiting at the abdominal wall ●Top-to-bottom – Two needle trocars are inserted through abdominal incisions and passed through the retropubic space, exiting through a vaginal incision
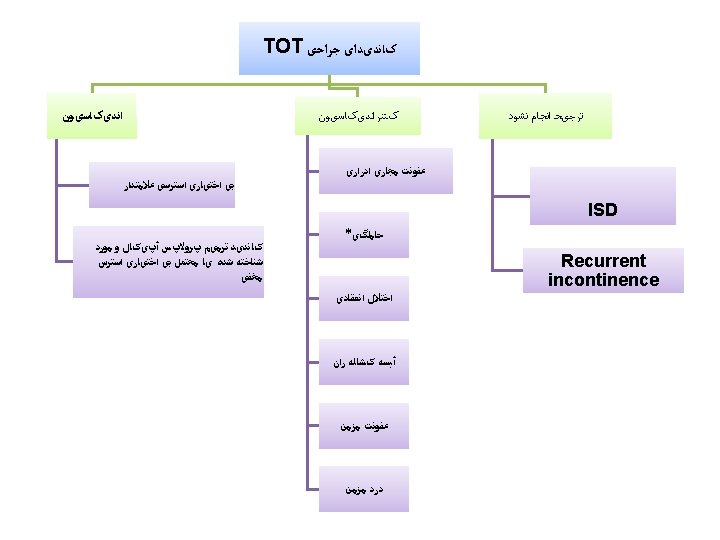
** Lower rates of urinary tract injury, voiding dysfunction, blood loss with TOT. ** Post operative de novo urgency or UI occurred at similar rates for TOT & TVT. ** Post operative groin pain was significantly more likely to occur with TOT. ** Higher rate of de novo dyspareunia in women who underwent TOT.
COMPLICATIONS • Retropubic midurethral sling placement is a minimally invasive procedure and complications are uncommon. • The most frequent complications of this procedure are bladder perforation, voiding dysfunction, and development of urinary urgency symptoms.
• Antibiotic prophylaxis is not required for short- or longterm bladder catheter use. Antimicrobial therapy should be reserved for patients with a urinary tract infection • Sling release — Most cases of postoperative urinary retention resolve with conservative management. Urinary retention that persists after four to six weeks may require surgical intervention in the form of a sling release
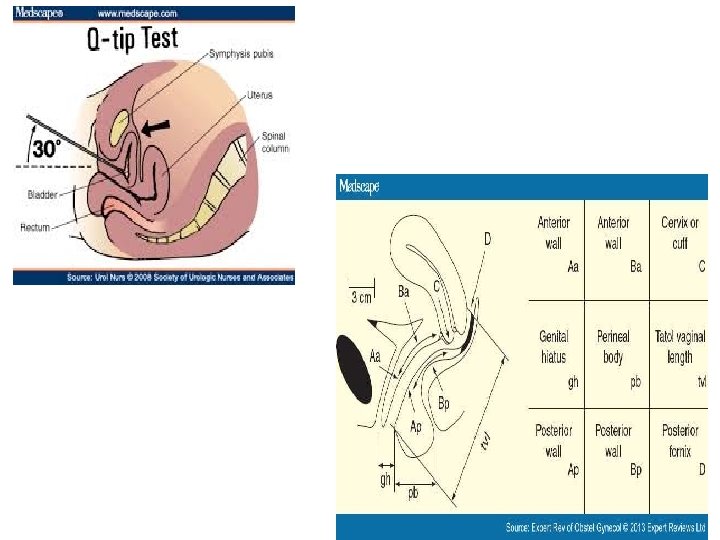
Risk factors for failure • previous anti-incontinence surgery (2 -fold increased risk) • urgency symptoms (as measured by a questionnaire score; 2 -fold) • maximum Q-tip excursion <30° on preoperative urethral hypermobility testing (1. 9 -fold) • Objective, but not subjective, failure was associated with age (1. 5 -fold per 10 years) • Having concomitant surgery was associated with a lower risk of subjective, but not objective, failure (0. 44 -fold)
Level C • Autologous fascial bladder neck slings should be considered in women with: 1 - severe SUI and a non mobile fixed urethra 2 – urethral diverticula or fistula 3 – with complications from mesh previously placed in the anterior vagina ACOG 2015
Injection of urethral bulking agents *The use of urethral injectable agents is often reserved for women who are unable to tolerate , or wish to defer , surgery. *these agents are used in some patients with recurrent or refractory incontinence after a prior incontinence procedure. ( grade 2 C ) Up to date 2017
Level B • Urethral bulking injections are a relatively noninvasive treatment for SUI that may be appropriate if : • 1 – surgery has failed to achieve adequate symptom reduction • 2 – symptoms recur after surgery • 3 – in women with symptoms who do not have urethral mobility • 4 – in older women with comorbidities who can not tolerate anesthesia or more invasive surgery ACOG 2015
PERSISTENT OR RECURRENT SUI ? ?
• For patients who present at the postoperative visit after a retropubic midurethral sling procedure and report persistent stress urinary incontinence, the position of the sling should be evaluated. • Clinicians may assess positioning of the sling with palpation along the urethra. They may also check for the presence or absence of urethral hypermobility.
• Failed slings were often positioned too proximally. • When a midurethral sling is too proximal, continence can be achieved by placing a repeat midurethral sling properly under the midurethra without removing the non-functioning sling.
SUBSEQUENT PREGNANCY ? ? ?
• Since pelvic support may be disrupted during pregnancy, and particularly following a vaginal birth, most physicians recommend delaying midurethral sling placement until childbearing has been completed. • In women who become pregnant following antiincontinence surgery, the best choice for mode of delivery is uncertain.