Review of Antenatal Care ESMOE What is the



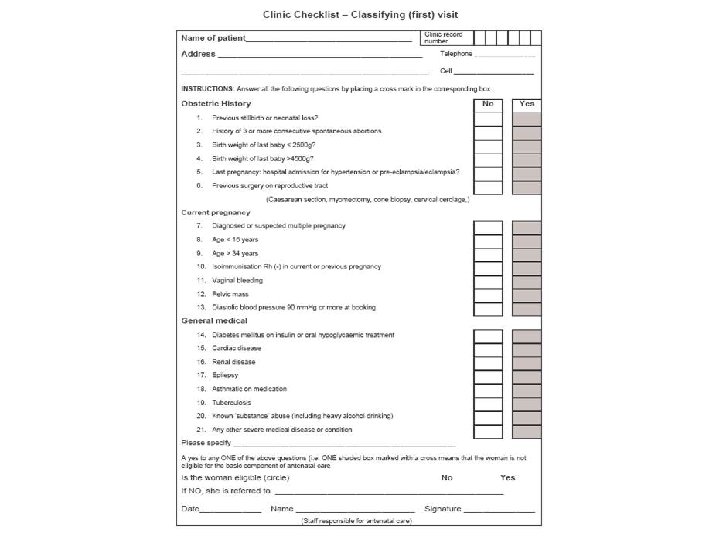
 • Simple checklist for problem identification •")



 Examination Pregnancy duration established and recorded Screening")

 Number of previous pregnancies Parity (P) Number of pregnancies to reach")



 Check EDD Examination Update the problem")




























 with no")
 babies • Smoker •")


- Slides: 69
Review of Antenatal Care ESMOE
What is the aim of Antenatal Care? To end up with a happy mum and healthy baby
What Are The Principles Of Antenatal Care?
The Principles of Basic Antenatal Care (BANC) • Simple checklist for problem identification • Risk assessment & appropriate level of care • Balancing visit: benefit ratio • Only doing appropriate On-site testing • Having a definite plan for ANC • Respectful care
It is essential to understand the importance of antenatal care and realise that a poorly planned ANC programme is little better than no antenatal care
Past obstetric history Past pregnancy performance is the single most important outcome predictor for the current pregnancy • Past perinatal death • Previous preterm labour • Previous caesarean section (C/S) • History of ante- or postpartum haemorrhage
The Bottom Line Is……. You cannot manage a problem if you have not identified it!!!
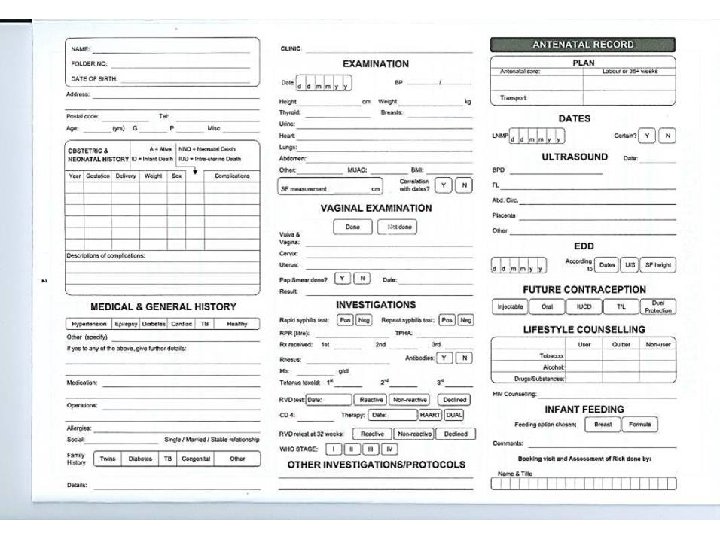
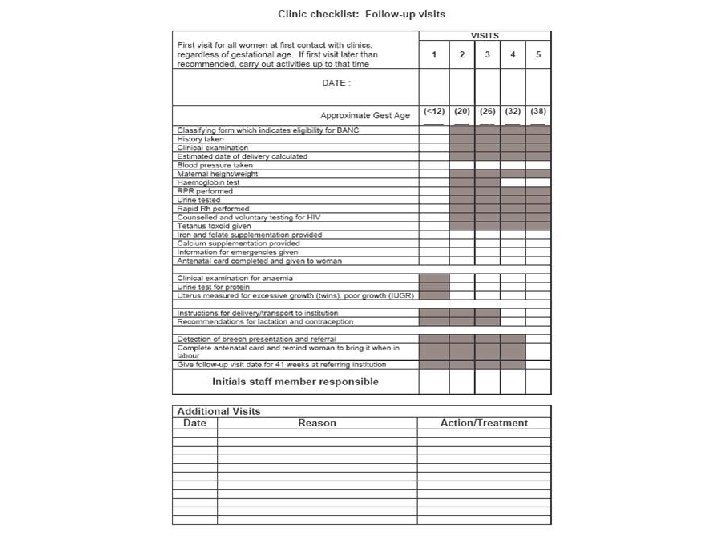
Booking visit Full history (including TB screen) Examination Pregnancy duration established and recorded Screening tests First assessment of risk factors (Problem list)
Dating this pregnancy - EDD Gestational age LNMP/LMP Uterine size - 4 -12 weeks - 13 -24 weeks - 24 -36 weeks Ultrasound (up to 24 weeks) Estimated fetal mass RECORD AND EXPLAIN
Definitions Gravidity (G) Number of previous pregnancies Parity (P) Number of pregnancies to reach viability irrespective of outcome or number
General examination General impression Pulse, BP, temperature, respiratory rate System examination Abdominal examination Per vaginal examination (PV) if indicated Side room investigations
Routine testing – must be done on-site Rapid RPR Rapid Rh Anaemia screen HIV MUAC Dipstix for protein and glucose
Final assessment Identification of problems and risks Antenatal care plan
Subsequent Visits Screen card History (including TB screen) Check EDD Examination Update the problem list Modify the plan
Educational Opportunity ü Encourage ANC attendance ü Pregnancy warning signs: • Reduced fetal movements • Vaginal bleeding • Rupture of membranes • Abdominal pain (not discomfort) • Severe headache • Report early in labour ü Self care & delivery ü Breast feeding ü Immunization ü Contraception ü HIV & STD’s ü MOM connect
Why Is It Important To Complete The Card? Because if it is not done problems will be not be identified The patient will not be treated correctly
Problem List & Notes Ø Be aware that the problems change as pregnancy progresses Ø Short and to the point! Ø Alert HCW at next visit to intervention
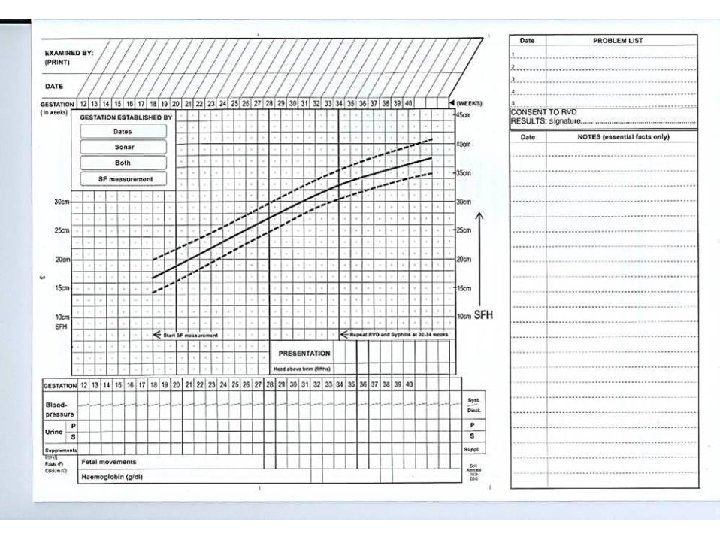
Monitoring Fetal Growth
Measuring The SFH • Make sure the bladder is not full • Let the woman lie comfortably on her back • Identify highest point of fundus. This might not be in the midline
Measuring The SFH • Mark the highest point of the fundus with a ball-point pen (ask for permission first) • Do not correct dextroversion of the uterus or exert pressure on the fundus
Measuring The SFH • Fix the zero of the tape measure at the top of the symphysis and stretch the tape over the curve of the uterus up to the pen mark • Read the measurement to nearest cm
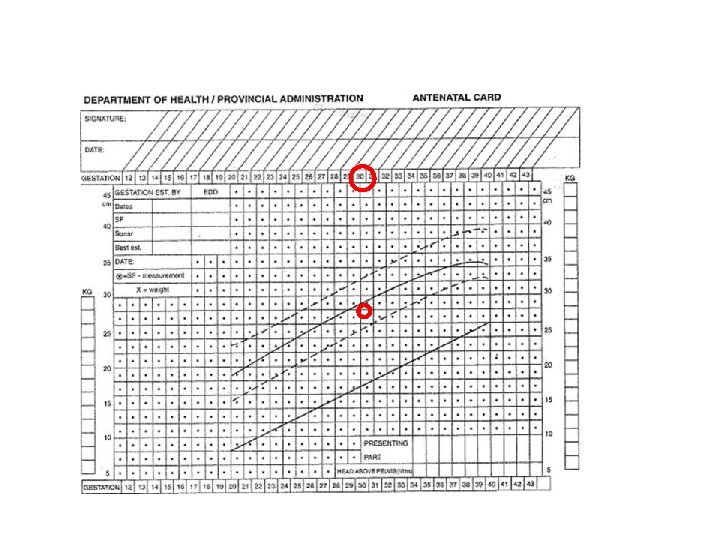
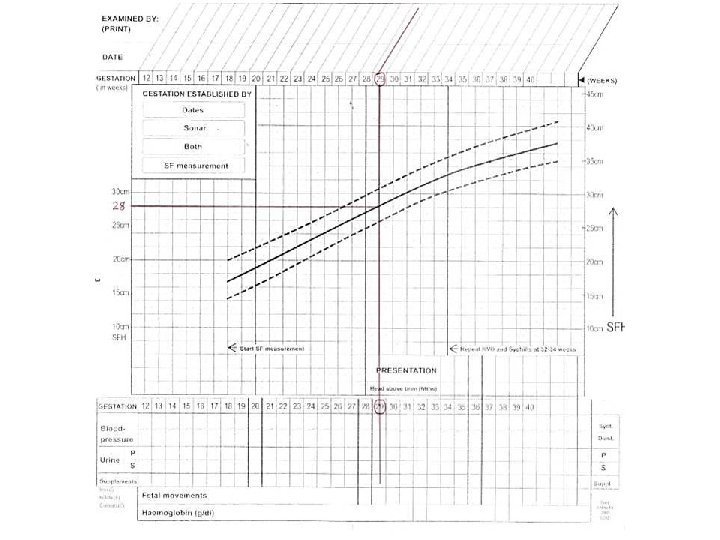
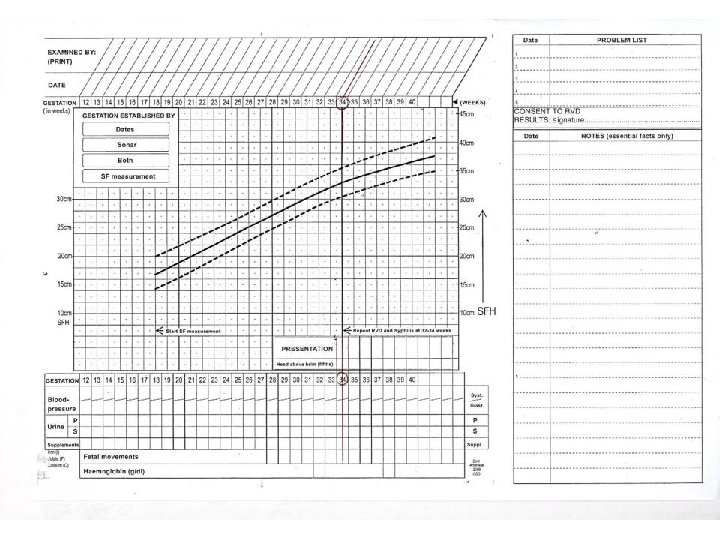
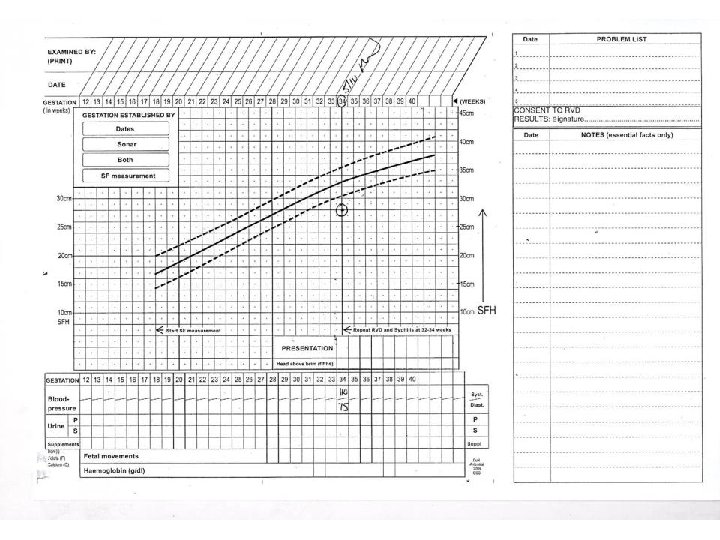
if the EDD is the 30 th September, and the date of the visit is the 22 nd July, then the gestational age at the time of the visit is 30 weeks gestation. Circle 30 weeks on the gestation line.
The SF measurement was 28 cm. Go the 28 cm on the SF measurement line and follow it across (blue line) until it meets the 30 week line (red). Mark where they meet with a circle.
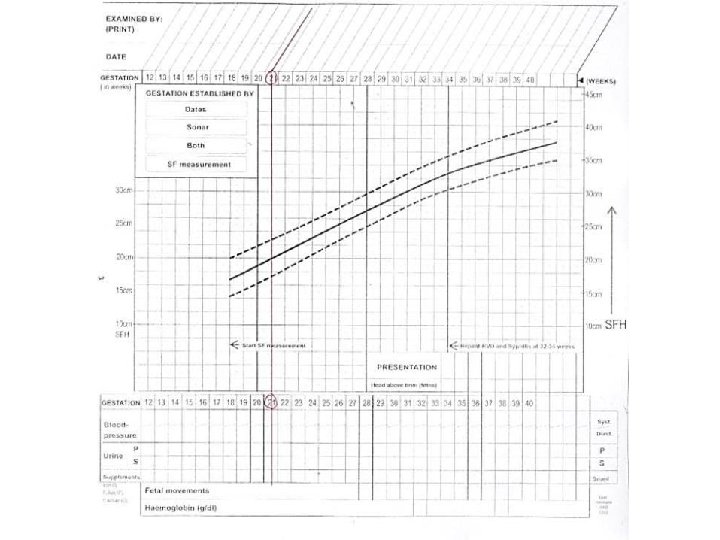
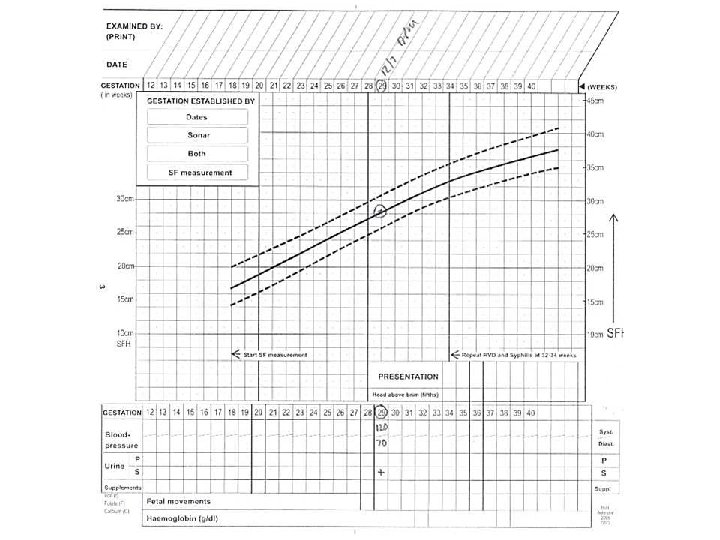
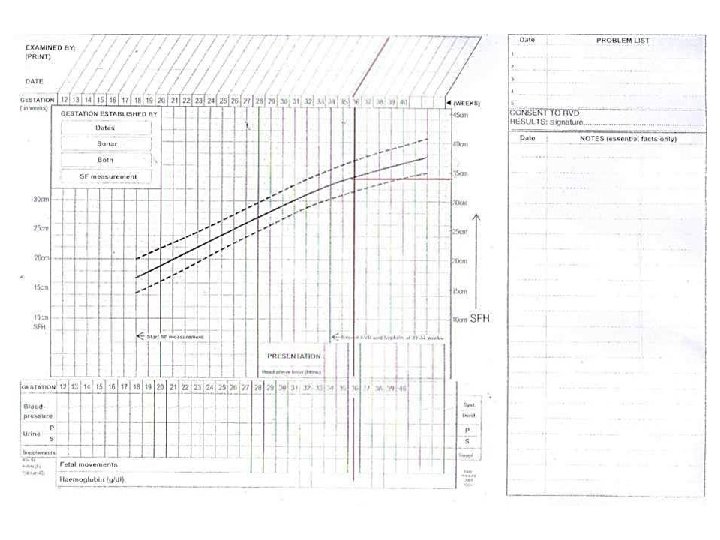
If the dates are unknown. SF is 26 cm. Go to 26 cm on SF line. Draw line across until it meets the 50 th percentile line.
Go up the verticle line to the gestation line. Circle the gestation line. That is the estimated gestation. From now on start at the gestation line and plot the SF as if the gestational was certain.
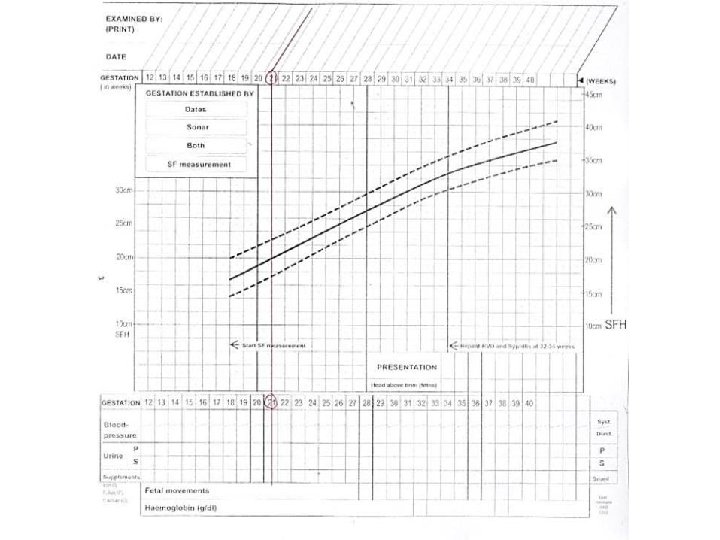
Enter The Following Information LMP - certain Now 21 weeks SF 22 cm BP 110/70 mm. Hg
What Is The 1 st Question To Ask? Do we have certain gestation? Yes Why? Because we have certain dates (21 wks)
Enter The Following Data • LMP? • SF 28 cm • B/P 120/70 • Urine 1+ glucose
What Is the 1 st Question To Ask? Do we have certain gestation? No So? Use the SF measurement
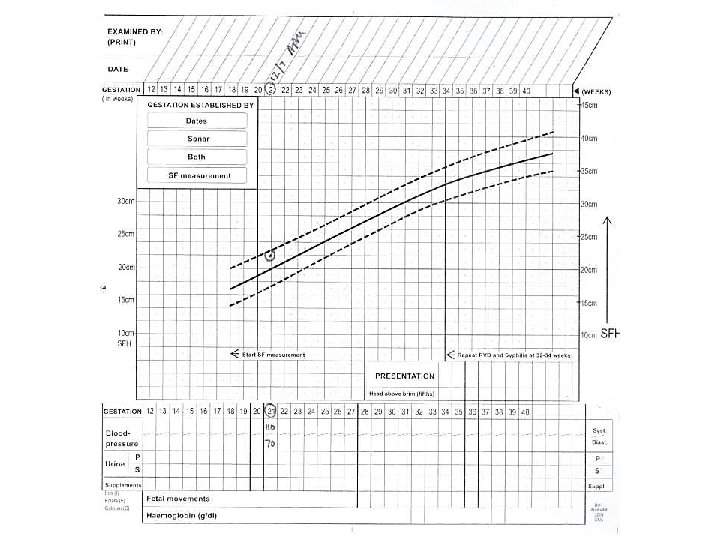
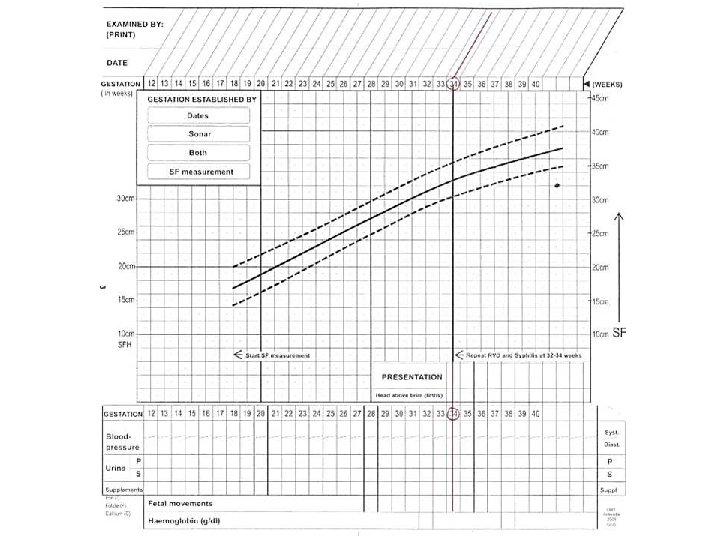
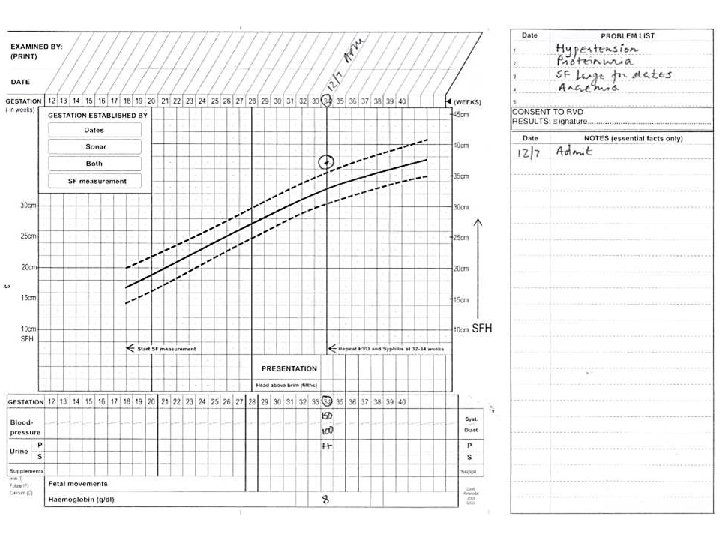
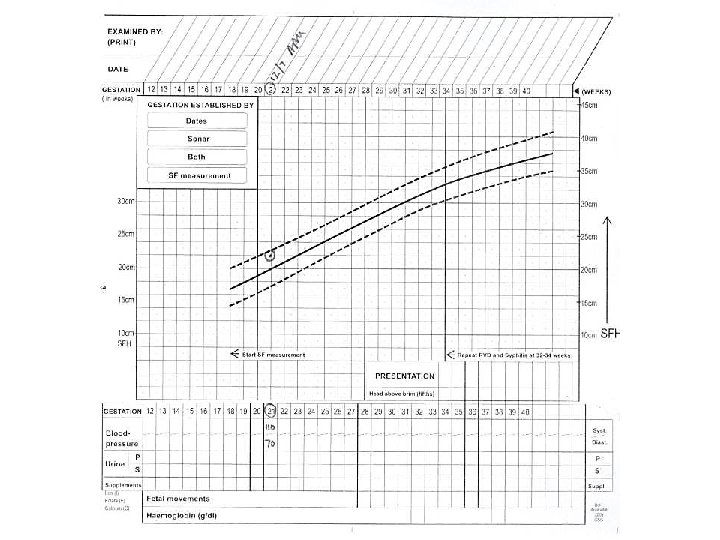
Enter The Following Data Certain dates - 34 wks SF 37 cm BP 150/100 mm. Hg Urine 2++ Protein Haemoglobin 8 g/dl
What is the 1 st question to ask? Do we have certain gestation? Yes So? Enter at 34 weeks
Is the card now complete? No Why? No problem list!
Enter The Following Data Unsure dates Ultrasound 21 wks SF 22 cm BP 110/70 mm. Hg
What Is The 1 st Question To Ask? Do we have certain gestation? Yes Why? Because we have early ultrasound
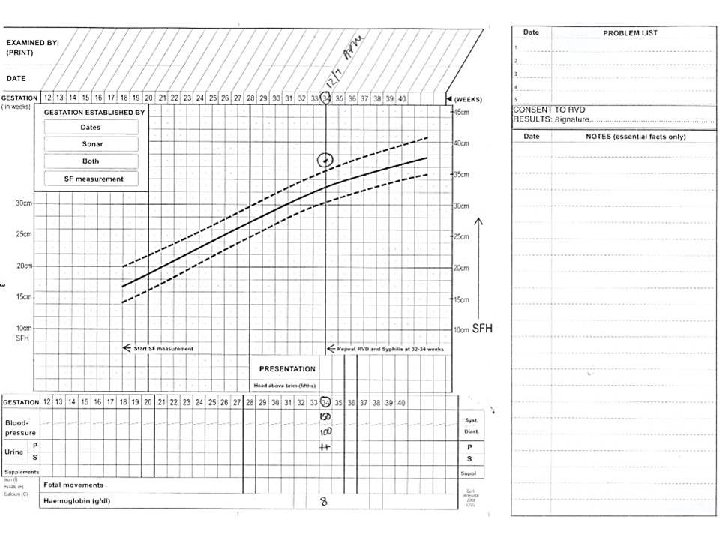
Enter The Following Information Certain dates 34 weeks SF 28 cm BP 110/75 mm. Hg
What Is The Problem? Certain dates and SF do not correspond So? IUGR or incorrect dates and a late booker
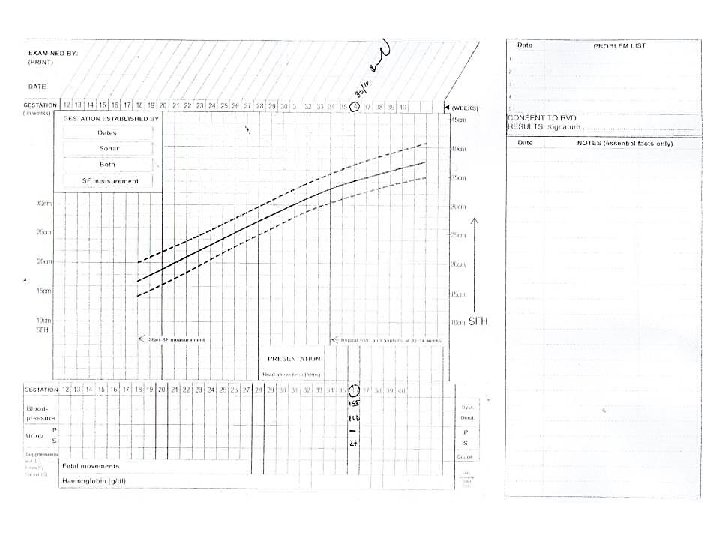
Enter The Following Information 38 yr old G 6 P 5 ( 2 x prev C/S) LMP ? ? ? Ultrasound 32 weeks SF 34 cm BP 155/100 mm. Hg Urine: Protein –ve, 2+ glucose
1 st Question? Do we have certain dates? No But U/S = 32 weeks So? Use SF Why not U/S? Because late U/S is not accurate!
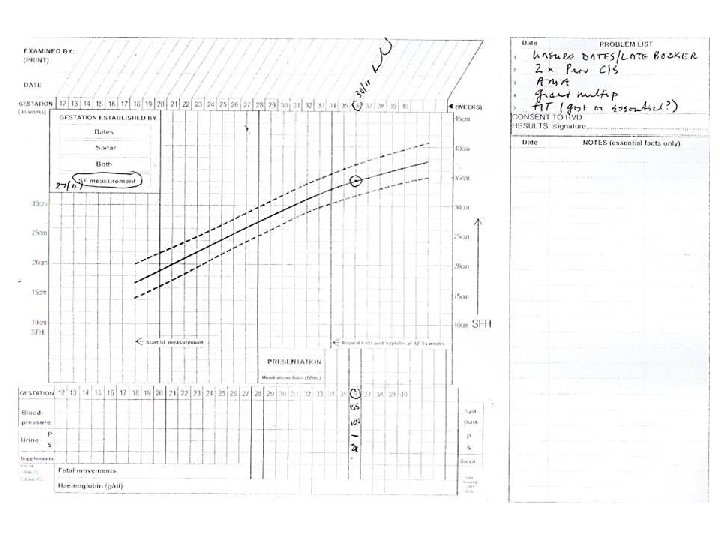
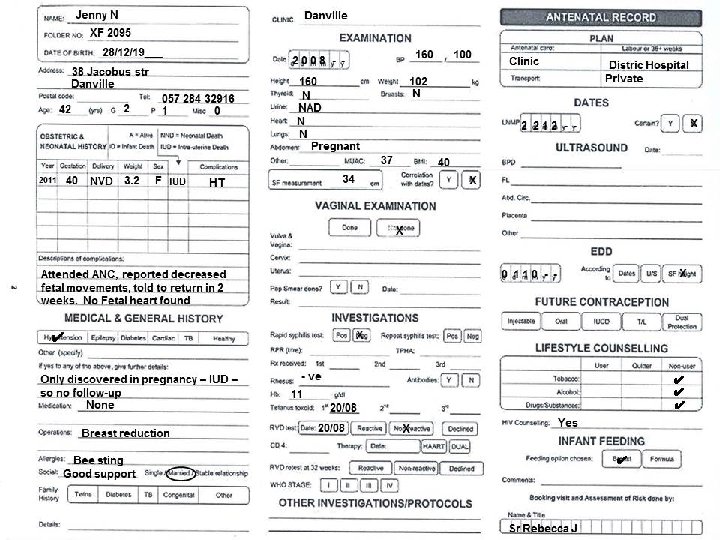
Work out problem lists for the following antenatal card, and start SF graph
Problem List • Previous IUD • Pregnancy was complicated by hypertension (HT) with no follow-up • Advanced maternal age (AMA) • Unsure dates & late booker • HT and obesity (BMI = 40, UMAC = 37) • Rh –ve (no Ab titre done) • Inappropriate level of care
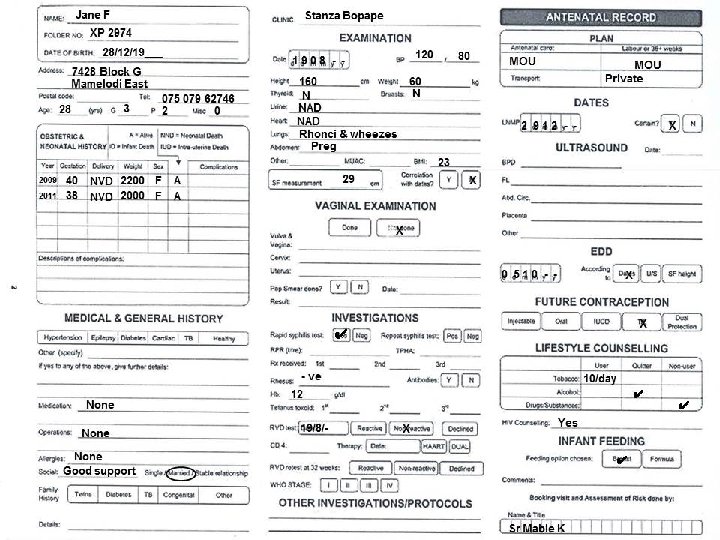
Problem List • 2 x small for gestational age (SGA) babies • Smoker • No MUAC • Ronchi & Wheezing • SF small for dates (29 @ 33/52) • No tet toxoid • RPR +ve, Rh –ve • Inappropriate level of care
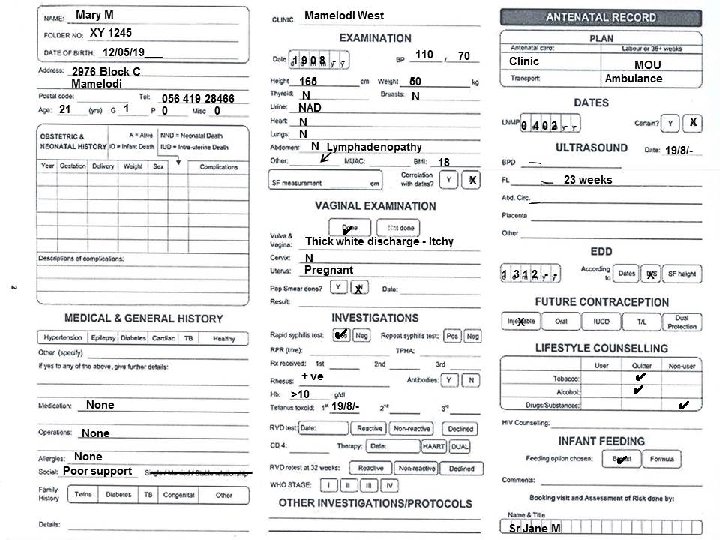
Problem List • Unsure dates? • Poor social circumstances • Small and underweight – no UMAC • Lymphadenopathy and vaginal candidiasis • No Rx of candidiasis or Pap smear taken • RPR +ve – no treatment • No HIV counseling or testing
Any Questions ?