Respiratory for Finals Natalie Grundmann Natalie grundmann 1nhs


















")


")








 Urea >7 mmol/L RR >30/min")




















 Right upper lobe collapse")






















- Slides: 75
Respiratory for Finals Natalie Grundmann Natalie. grundmann 1@nhs. net
What we will cover ◦ Content = common respiratory conditions that will come up in finals (not an exhaustive list, not covid) ◦ Structure = best of 5 question followed by teaching, some data interpretation throughout ◦ Ask questions as we go ◦ You will get slides at the end
D – Details R – RIPE How to read a CXR: DR ABCDE Rotation, Inspiration, Projection, Exposure A – Airway and mediastinum B – Breathing C - Circulation D – Diaphragm E - Extras
An 18 year old boy presents with sudden onset SOB and chest pain. Usually fit and well. What is the cause for his symptoms? 1. Right sided spontaneous secondary pneumothorax 2. Tension pneumothorax 3. Right sided rib fracture 4. Right sided spontaneous primary pneumothorax 5. Right sided collapsed upper lobe
An 18 year old boy presents with sudden onset SOB and chest pain. Usually fit and well. What is the cause for his symptoms? 1. Right sided spontaneous secondary pneumothorax 2. Tension pneumothorax 3. Right sided rib fracture 4. Right sided spontaneous primary pneumothorax 5. Right sided collapsed upper lobe
Types of Pneumothorax ◦ Primary = no underlying disease ◦ Cause = ruptured subpleural bulla ◦ Secondary = underlying lung disease ◦ Smoker >50 ◦ COPD, asthma, carcinoma etc. ◦ CTD: Marfans, EDs Non spontaneous causes o Trauma – rib fracture, penetrating injury o Iatrogenic: NIV, biopsies/aspiration
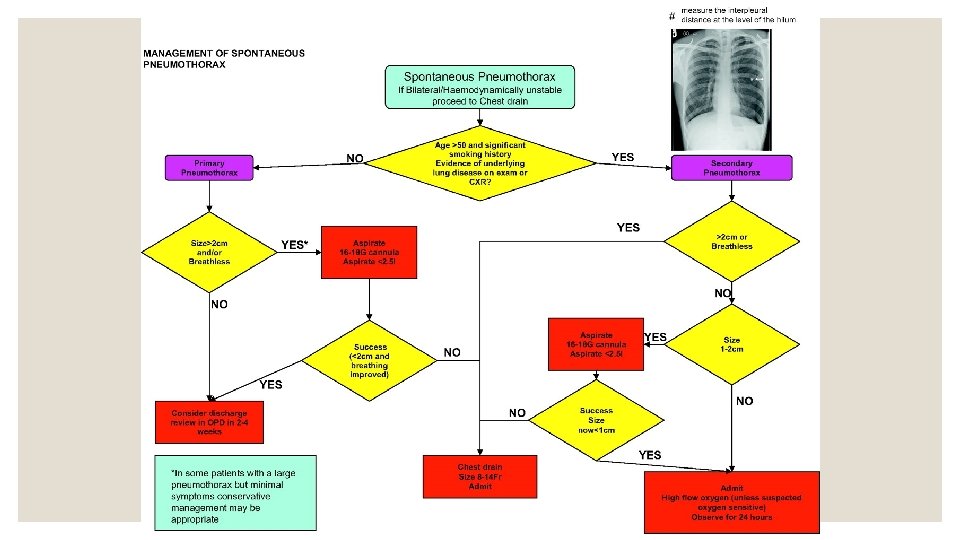
A 57 year old smoker presents to ED with SOB and chest pain. CXR showed a simple pneumothorax with rim of air of 1. 5 cm. What is the most appropriate management? 1. Aspiration 2. Discharge with safety netting advice 3. Chest drain 4. Urgent needle decompression 5. CPAP
A 57 year old smoker presents to ED with SOB and chest pain. CXR showed a simple pneumothorax with rim of air of 1. 5 cm. What is the most appropriate management? 1. Aspiration 2. Discharge with safety netting advice 3. Chest drain 4. Urgent needle decompression 5. CPAP
A 36 year old man presents in respiratory distress. HR 120, RR 32, Sp. O 2 97%, BP 96/70. What is the most appropriate management? 1. Urgent needle decompression 2. Urgent portable CXR followed by needle decompression 3. Urgent needle decompression followed by chest drain 4. Urgent chest drain insertion 5. Urgent intubation and ventilation
A 36 year old man presents in respiratory distress. HR 120, RR 32, Sp. O 2 97%, BP 96/70. What is the most appropriate management? 1. Urgent needle decompression 2. Urgent portable CXR followed by needle decompression 3. Urgent needle decompression followed by chest drain 4. Urgent chest drain insertion 5. Urgent intubation and ventilation
SIMPLE TENSION No mediastinal shift Trachea/mediastinal deviation away from the pneumothorax. CXR diagnosis Prompt clinical diagnosis – CXR delays management • Sit up, give 15 l/min oxygen • GET HELP • Immediate needle decompression (thoracocentesis)- 2 nd intercostal space, midclavicular line. Chest drain (to prevent reaccumulation)
An 81 year old smoker presents with a chronic cough, weight loss and left arm pain. On examination you notice he has a pin point left pupil and a left sided ptosis. Which of the following is the most likely cause of this man’s symptoms? 1. Disseminated TB 2. Adenocarcinoma 3. Squamous cell carcinoma 4. Pancoast tumour 5. Large cell carcinoma
An 81 year old smoker presents with a chronic cough, weight loss and left arm pain. On examination you notice he has a pin point left pupil and a left sided ptosis. Which of the following is the most likely cause of this man’s symptoms? 1. Disseminated TB 2. Adenocarcinoma 3. Squamous cell carcinoma 4. Pancoast tumour 5. Large cell carcinoma
Pancoast tumour ◦ A pancoast tumour is a tumour at the apex of the lung - defined by its location rather than pathology (most commonly squamous cell) Signs & symptoms ◦ Arm pain- brachial plexus & chest wall invasion ◦ Wasting of small muscles of the hand ◦ Facial swelling - SVC compression ◦ Hoarseness- damage to recurrent laryngeal nerve ◦ Horner’s syndrome – compression of the sympathetic ganglion (miosis, ptosis, anhidrosis)
A 65 year-old smoker presents with confusion and drowsiness. He used to work in the docks with asbestos. U&Es show Na+ 120, K+ 4. 5, Urea 6. 2 and Creat 52. Which of the following is the most likely cause of this man’s symptoms? 1. Small cell lung carcinoma 2. Adenocarcinoma 3. Squamous cell carcinoma 4. Malignant mesothelioma 5. Large cell carcinoma
A 65 year-old smoker presents with confusion and drowsiness. He used to work in the docks with asbestos. U&Es show Na+ 120, K+ 4. 5, Urea 6. 2 and Creat 52. Which of the following is the most likely cause of this man’s symptoms? 1. Small cell lung carcinoma 2. Adenocarcinoma 3. Squamous cell carcinoma 4. Malignant mesothelioma 5. Large cell carcinoma
Lung Cancer ◦ Most important distinction is between small-cell and non-small cell Type Epidemiology Pathology Behaviour Squamous Cell Carcinoma 35% M>F Smokers Centrally located (bronchial) Locally invasive Metastasises late via lymph nodes PTHr. P Ca 2+ Adenocarcinoma 30% F>M Non-smokers Peripherally located Extra-thoracic metastasis common and 80% present with metastasis Large-cell 5 -10% Peripherally or centrally located Poor prognosis Small-cell 20% Smoking (85%) Centrally located, (bronchial) Paraneoplastic syndromes 70% present with advanced disease, very poor prognosis Malignant Mesothelioma Asbestos Tumour of mesothelial cells in the pleura. Long latent period between exposure and presentation. Very poor prognosis.
Mesothelioma
Paraneoplastic Syndrome = non-metastatic manifestations of lung cancer Endocrine ◦ ADH SIADH (euvolemic Na+) ◦ ACTH Cushing’s syndrome ◦ Serotonin carcinoid (flushing, diarrhoea) ◦ HCG gynaecomastia ◦ PTHr. P 1 o HPT ( Ca 2+, bony pain) SCC
Paraneoplastic Syndrome = non-metastatic manifestations of lung cancer Cutaneous ◦ Acanthosis nigricans ◦ Trousseau syndrome: thrombophlebitis migrans
Paraneoplastic Syndrome = non-metastatic manifestations of lung cancer Rheumatology ◦ Dermatomyositis ◦ Polymyositits
Paraneoplastic Syndrome = non-metastatic manifestations of lung cancer CNS ◦ Purkinje cells (CDR 2) cerebellar degeneration ◦ Peripheral neuropathy ◦ Proximal myopathy - Lambert. Eaton syndrome Lambert Eaton Myaesthenic Syndrome • Weakness of the limbs – usually more in the legs than the arms. • Weakness of eye muscles is uncommon. • Temporarily relieved with exercise – distinguishing exam buzz word from MG
Lung Cancer Investigation and Management Investigation ◦ Cytology- sputum & pleural fluid ◦ CXR- first line ◦ Bronchoscopy – biopsy and to assess operability ◦ CT - stage disease ◦ PET/bone scans ◦ Lung function tests before operations Management ◦ NSCLC – surgical resection ◦ SCLC – chemotherapy
An 18 year-old girls presents with a sore throat for two days. She has a temperature of 38. 3. On examination she has pus on her tonsils and they look inflamed. What is the appropriate management? 1. Phenoxymethylpenicillin 2. No antibiotics needed 3. Delayed antibiotic prescription 4. Erythromycin 5. Clarithromycin
An 18 year-old girls presents with a sore throat for two days. She has a temperature of 38. 3. On examination she has pus on her tonsils and they look inflamed. What is the appropriate management? 1. Phenoxymethylpenicillin 2. No antibiotics needed 3. Delayed antibiotic prescription 4. Erythromycin 5. Clarithromycin
Antibiotics in sore throat Centor Criteria 1. Tonsillar exudate 2. Tender anterior cervical lymph nodes 3. Absences of cough 4. History of fever 3 -4: antibiotics 0 -2: no antibiotics Fever. PAIN criteria 1. Fever 2. Pus on tonsils, tonsillar exudate 3. Attends in <3 days 4. Inflamed Tonsils 5. No cough or coryza 0 -1: no antibiotics 2 -3: delayed antibiotics 4 -5: immediate antibiotics.
18 year old boy presented three days ago with a sore throat and malaise. He was given an antibiotic. He presents again today with this rash. What antibiotic was he given? 1. Phenoxymethylpenicillin 2. Amoxicillin 3. Doxycycline 4. Erythromycin 5. Clarithromycin
18 year old boy presented three days ago with a sore throat and malaise. He was given an antibiotic. He presents again today with this rash. What antibiotic was he given? 1. Phenoxymethylpenicillin 2. Amoxicillin 3. Doxycycline 4. Erythromycin 5. Clarithromycin
A 40 year old women presents to ED with a productive cough and pleuritic chest pain. She has no PMH. What is the most appropriate management? RR 28 Hb 130 HR 86 WBCs 11. 2 BP 110/76 CRP 56 Temp 38. 1 Na 136 Sp. O 2 96% on air K 4. 3 Urea 6. 5 Creat 51 1. 2. 3. 4. 5. Discharge with IV antibiotics Discharge with safety netting advice Discharge with delayed antibiotics Discharge with oral antibiotics and repeat CXR in 6 weeks
A 40 year old women presents to ED with a productive cough and pleuritic chest pain. She has no PMH. What is the most appropriate management? RR 28 Hb 130 HR 86 WBCs 11. 2 BP 110/76 CRP 56 Temp 38. 1 Na 136 Sp. O 2 96% on air K 4. 3 Urea 6. 5 Creat 51 1. 2. 3. 4. 5. Discharge with IV antibiotics Discharge with safety netting advice Discharge with delayed antibiotics Discharge with oral antibiotics and repeat CXR in 6 weeks
CURB-65 1. 2. 3. 4. 5. Confusion (AMT 8) Urea >7 mmol/L RR >30/min BP <90/60 65 Score • 0 -1 home management • 2 hospital management • 3 consider ITU In primary care, use CRB-65 (same as above without urea). In this case, only score of 0 should be managed at home. Admit for 1 -3
A 70 -year-old lady with a background of type 2 diabetes mellitus and alcohol abuse presents with a fever and productive cough. She reports no weight loss or haemoptysis. She was born in England has never travelled outside of the UK. She has never smoked. O/E she has crackles in her right upper lobe but is otherwise well. CXR reveals consolidation which is cavitating in her right upper lobe. What is the diagnosis? 1. Lung cancer 2. TB 3. Pneumococcal pneumonia 4. Aspergillosis 5. Klebsiella pneumonia
A keen bird keeper presents with a dry cough, headache, and patchy consolidation on CXR. What organism is likely causing his symptoms? 1. Chlamydophila pneumoniae 2. Streptococcus pneumoniae 3. Haemophilus influenzae 4. Legionella pneumophilia 5. Chlamydophila psittaci
A businessman has just got home from a work trip to Thailand. He presents to his GP with a dry cough and a flu like illness prior to this. His bloods show Na 127, K 4. 7, Urea 6. 2, Creat 52, Hb 132, WBCs 13. 2. What investigation would be diagnostic? 1. Chest x-ray 2. Urinary antigens 3. Respiratory PCR swab 4. Urinary antibodies 5. Sputum sample
Organism Risk Factors Pulmonary Features Elderly, ETOH, Pneumococcus Immunocompromised, CHF, Lobar consolidation Pulmonary disease Staphylococcal Influenza infection, IVDU Klebsiella Elderly, ETOH, DM, HAP Mycoplasma Legionella Occurs in epidemics Travel Air conditioning Pisittacosis: Chlamydiophila Zoonotic: parrots psittaci Pneumocystis pneumonia (PCP) Immunocompromised Pneumocystis jiroveci Extra-pulmonary Features Herpes labialis Bilateral cavitating bronchopneumonia CXR: Cavitating pneumonia, especially in upper lobes. Red current jelly sputum Dry cough CXR: Reticulo-nodular shadowing or patchy consolidation often of one lower lobe Diagnosis: serology Dry cough CXR: bi-basal consolidation Diagnosis = urinary antigen Dry cough CXR: patchy consolidation Dry cough, exertional dyspnoea , Pa. O 2 Bilateral crepitations CXR: normal or bilateral perihilar interstitial shadowing Flu-like prodrome, autoimmune haemolytic anaemia, erythema multiforme, encephalitis, GBS Flu-like prodrome, Na, deranged LFTs Causes psittacosis. Headache, fever, lethargy, arthralgia. D&V Horder’s spots/rose spots
A 70 -year-old lady with a background of type 2 diabetes mellitus and alcohol abuse presents with a fever and productive cough. She reports no weight loss or haemoptysis. She was born in England has never travelled outside of the UK. She has never smoked. O/E she has crackles in her right upper lobe but is otherwise well. CXR reveals consolidation which is cavitating in her right upper lobe. What is the diagnosis? 1. Lung cancer 2. TB 3. Pneumococcal pneumonia 4. Aspergillosis 5. Klebsiella pneumonia
A keen bird keeper presents with a dry cough, headache, and patchy consolidation on CXR. What organism is likely causing his symptoms? 1. Chlamydophila pneumoniae 2. Streptococcus pneumoniae 3. Haemophilus influenzae 4. Legionella pneumophilia 5. Chlamydophila psittaci
A businessman has just got home from a work trip to Thailand. He presents to his GP with a dry cough and a flu like illness prior to this. His bloods show Na 127, K 4. 7, Urea 6. 2, Creat 52, Hb 132, WBCs 13. 2. What investigation would be diagnostic? 1. Chest x-ray 2. Urinary antigens 3. Respiratory PCR swab 4. Urinary antibodies 5. Sputum sample
p. H This gas was taken from a patient having an acute asthma attack. What is the worrying feature? p. O 2 7. 40 15 p. CO 2 5 HCO 3 - 24 BE -1
p. H This gas was taken from a patient having an acute asthma attack. What is the worrying feature? p. O 2 7. 40 15 p. CO 2 5 HCO 3 - 24 BE • -1 • Normal PCO 2 in a patient with acute asthma – patient is getting tired and cannot expire the CO 2 Raised Pa. CO 2 is a sign of a near fatal asthma attack and an indication for mechanical ventilation
A 24 -year-old male is admitted with acute severe asthma. Treatment is initiated with 100% oxygen, nebulised salbutamol and ipratropium bromide nebulisers and IV hydrocortisone. Despite initial treatment there is no improvement. What is the next step in management? 1. IV aminophylline 2. IV magnesium 3. IV salbutamol 4. NIV 5. IV adrenaline
A 24 -year-old male is admitted with acute severe asthma. Treatment is initiated with 100% oxygen, nebulised salbutamol and ipratropium bromide nebulisers and IV hydrocortisone. Despite initial treatment there is no improvement. What is the next step in management? 1. IV aminophylline 2. IV magnesium 3. IV salbutamol 4. NIV 5. IV adrenaline
Management of acute severe asthma: O SHIT ME If not improving: Immediate treatment • O 2 • Salbutamol neb 5 mg (up to back) • Hydrocortisone 100 mg IV OD • Ipratropium 0. 5 mg neb • • Escalate care: inform ITU Mg. SO 4 IV infusion Theophylline: aminophylline Salbutamol IV infusion
A 63 presents with productive cough, reduced exercise tolerance and increased SOB on exertion. He has a PMH of BPH, COPD and T 2 DM. He has a CXR shown below. What is the most likely diagnosis? 1. CAP 2. Pneumothorax 3. IE COPD 4. Heart failure 5. Sarcoidosis
A 63 presents with productive cough, reduced exercise tolerance and increased SOB on exertion. He has a PMH of BPH, COPD and T 2 DM. He has a CXR shown below. What is the most likely diagnosis? 1. CAP 2. Pneumothorax 3. IE COPD 4. Heart failure 5. Sarcoidosis
Management of Acute Exacerbation of COPD Controlled O 2 Therapy • Vary target according to ABG • Aim for Pa. O 2 >8 and increased in PCO 2 of <1. 5 KPa Antibiotics Nebulisers • Salbutamol • Ipratropium 0. 5 mg/6 h Steroids • Hydrocortisone IV • Prednisolone PO for 7 -14 d • Antibiotic therapy indicated if two of: • Increased SOB • Increased sputum volume • Increased sputum purulence Non invasive ventilation • Consider NIV (Bi. PAP) if p. H 7. 257. 35 (T 2 RF) • Consider invasive ventilation if p. H<7. 25
What is the most likely cause of this CXR? 1. Pleural effusion 2. Lung cancer 3. Pneumonectomy 4. Pulmonary oedema 5. Ruptured diaphragm
What is the most likely cause of this CXR? 1. Pleural effusion 2. Lung cancer 3. Pneumonectomy 4. Pulmonary oedema 5. Ruptured diaphragm
Hemi-thorax whiteout Trachea Pulled Towards Trachea Central Trachea pushed away Pneumonectomy Consolidation Pleural effusion Total lung collaps Pulmonary oedema Diaphragmatic hernia
An 83 year old man presents with shortness of breath and weight loss. On examination you note reduced air entry in the right upper zone. Which of the following best describes his X-ray appearances? 1. Right upper lobe collapse 2. Left upper lobe collapse 3. Right middle lobe collapse 4. Right upper lobe consolidation 5. Right lower lobe collapse
An 83 year old man presents with shortness of breath and weight loss. On examination you note reduced air entry in the right upper zone. Which of the following best describes his X-ray appearances? 1. Right upper lobe collapse 2. Left upper lobe collapse 3. Right middle lobe collapse 4. Right upper lobe consolidation 5. Right lower lobe collapse
Golden ‘S’ sign (if right hilar mass) Right upper lobe collapse
Mrs Jones is an 79 year old patient who presents to ED with a 2 day history of worsening shortness of breath and haemoptysis. 1. Left sided pneumothorax 2. Left lower lobe collapse 3. Left middle lobe collapse 4. Right sided pneumothorax 5. Left lower lobe consolidation
Mrs Jones is an 79 year old patient who presents to ED with a 2 day history of worsening shortness of breath and haemoptysis. 1. Left sided pneumothorax 2. Left lower lobe collapse 3. Left middle lobe collapse 4. Right sided pneumothorax 5. Left lower lobe consolidation
Sail sign Left lower lobe collapse
Veil sign Left upper lobe collapse
Difficult to see on CXR Depression of horizontal fissure Right middle lobe collapse
Sail sign Right lower lobe collapse
Lobar Collapse Look for loss of volume ◦ Raised hemidiaphragm ipsilaterally ◦ Trachea and mediastinal shift towards the collapsed side ◦ Displacement of the hila ◦ Narrowing of the space between the ribs compared to the opposite side Management ◦ Chest physio, treat the cause
A 45 year old woman presents to AMU with right sided pleuritic chest pain and shortness of breath. Which of the following is not a cause of an exudative pleural effusion? 1. Pneumonia 2. Acute pancreatitis 3. Cirrhosis 4. Pulmonary infarction 5. TB
A 45 year old woman presents to AMU with right sided pleuritic chest pain and shortness of breath. Which of the following is not a cause of an exudative pleural effusion? 1. Pneumonia 2. Acute pancreatitis 3. Cirrhosis 4. Pulmonary infarction 5. TB
Types of Pleural Effusions Transudate Pleural Effusions <30 g/L protein Bilateral Pathology: capillary hydrostatic or oncotic pressure Causes o CCF: most common Hypoalbuminaemia: liver failure, nephrotic syndrome, enteropathy or other malabsorption o Renal failure Exudate Pleural Effusions >30 g/L protein, lower PH Pathology: capillary permeability Causes o Infection: pneumonia (most common), TB o Neoplasm: lung, metastases o Connective tissue disease: RA, SLE o Pancreatitis o PE
A 36 year old lady with a PMH of breast cancer presents with SOB and pleuritic chest pain. What is the most likely diagnosis? 1. Pulmonary effusion 2. Pneumothorax 3. Pericarditis 4. Pneumonia 5. Pulmonary embolism
A 36 year old lady with a PMH of breast cancer presents with SOB and pleuritic chest pain. What is the most likely diagnosis? 1. Pulmonary effusion 2. Pneumothorax 3. Pericarditis 4. Pneumonia 5. Pulmonary embolism
What is the most common ECG finding in pulmonary embolism? Sinus tachycardia!
Pulmonary Embolism Treatment Length • If cause: 3 months of anticoagulation • No identifiable cause: 6 months anticoagulation • Cancer as cause: 6 months, previously with LMWH but now can use DOAC
Surgical emphysema
Normal CXR!
Heart Failure
Covid pneumonia
Sarcoidosis
Pneumoperitoneum
Any Questions?
Feedback Link