Chemical Pathology 1 Silvia Muttoni silvia muttoni 1nhs


 + urea")
 – Osmolality (hypothalamus) •")


 Cause Hypovolaemia > 20 = Renal Diuretics < 20")










 – Pituitary surgery – Irradiation –")

































- Slides: 53
Chemical Pathology 1 Silvia Muttoni silvia. muttoni 1@nhs. net
Contents • Sodium balance • Potassium • Enzymes and cardiac markers • Renal (AKI, CKD) • Metabolic disorders • Paediatric clinical chemistry Brief overview Will not be covered in this lecture – can be found in the path guide
Osmolarity vs osmolality • Osmolarity is calculated from blood tests: • 2(Na++K+) + urea + glucose • Why do we double sodium and potassium? • Osmolality is measurement of particles in solution by a machine • Normal range is 275 -295 m. Osmol/kg – The 2 should be roughly equal, if not then there is an “osmolar gap” – Excess “unmeasured solutes” such as mannitol, lipids, alcohol
Sodium regulation • 2 parameters: – Volume state (carotid sinus) – Osmolality (hypothalamus) • ADH – Causes insertion of aquaporin 2 into renal CD --> water reabsorbed from tubules – ADH = ADds H 2 O • High osmolality thirst + ADH release • Low osmolality ADH suppression
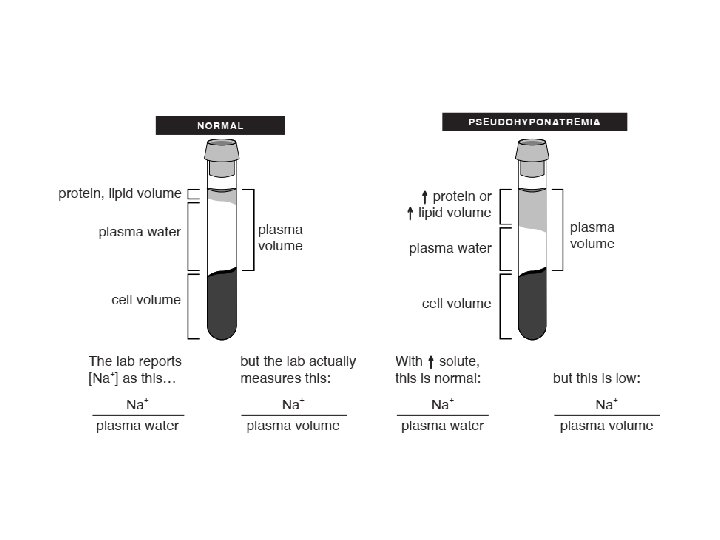
Sodium • Normal range: 135 – 145 mmol/l • First step is to determine whether it is true hyponatraemia by assessing the serum osmolality Osmolality High Causes Glucose/mannitol infusion Ethanol Normal Spurious e. g. drip arm sample Pseudohyponatraemia (hyperlipidaemia/ paraproteinaemia) Low True hyponatraemia
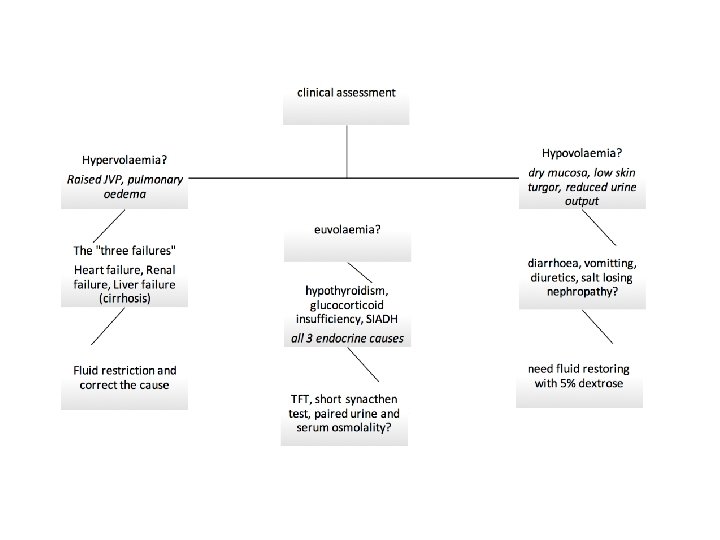
True hyponatraemia • Na <135 • Serum osmolality is LOW • Causes can be distinguished using hydration status and urinary sodium
Hydration status Urinary sodium (mmol/l) Cause Hypovolaemia > 20 = Renal Diuretics < 20 = Non-renal Vomiting, diarrhoea, excessive sweating, burns Euvolaemia > 20 SIADH, Addison’s, hypothyroidism Hypervolaemia >20 = Renal AKI, CKD < 20 = Non-renal Cardiac failure, cirrhosis
SIADH • Syndrome of inappropriate ADH • Criteria: – – True hyponatraemia (low serum osmolality) High urine osmolality Clinically euvolaemic Diagnosis of exclusion i. e. 9 am cortisol and TFTs are normal • Causes: – – Malignancy: small cell lung cancer, breast cancer CNS disorders: encephalitis, abscess Chest disease: pneumonia, TB Drugs: opiates, SSRIs, carbamazepine
Treatment of hyponatraemia – Hypovolaemia • Replace lost water • Treat the cause e. g. vomiting – give anti-emetics – Euvolaemia • Fluid restrict • Treat the cause – Hypothyroidism: thyroxine – Addison’s: hydrocortisone – SIADH: if resistant, can trial demeclocycline or tolvaptan – Hypervolaemia • Fluid restrict • Treat the cause
Treatment of hyponatraemia • Acute hyponatraemia can be symptomatic – – – Nausea and vomiting (< 134) Confusion (< 131) Seizures (< 125) Coma (< 117) In exceptional circumstances e. g. in a patient who is in status epilepticus secondary to hyponatraemia, hypertonic (3%) saline may be used on advise of a specialist and usually in ITU • Rapid correction can lead to central pontine myelinolysis (pseudobulbar palsy, paraparesis, locked-in syndrome) therefore aim to increase Na+ by no more than 8 -10 mmol per 24 h. • Note that chronic hyponatraemia may be asymptomatic even at low concentrations
Practice Question A patient presents with a seizure and his sodium is discovered to be 119 m. M on investigation. His mouth is dry and his capillary refill is >2 s. He has a urine sodium of 45 m. M What is the likely cause of the hyponatraemia? A. B. C. D. E. SIADH Cardiac failure Diuretic administration Excess diarrhoea and vomiting Hypothyroidism 13
Practice Question A patient presents with a seizure and his sodium is discovered to be 119 m. M on investigation. His mouth is dry and his capillary refill is >2 s. He has a urine sodium of 45 m. M What is the likely cause of the hyponatraemia? A. B. C. D. E. SIADH Cardiac failure Diuretic administration Excess diarrhoea and vomiting Hypothyroidism 14
Practice Question VSA – type 1. A patient with severe hyponatraemia is thought to have SIADH. What would you expect his urine sodium to be? 15
Practice Question VSA – type 1. A patient with severe hyponatraemia is thought to have SIADH. What would you expect his urine osmolality to be? Answer: By definition, urine osmolality is HIGH in SIADH 16
Hypernatraemia • Na >145 • Much less common that hyponatraemia • Causes: D&V, diabetes insipidus, Conn’s syndrome, iatrogenic • Hypernatraemia will cause thirst initially, therefore most people should be able to self-correct, unless: – Elderly / dementia – Fasting for surgery – Can’t keep up with losses
Practice Question A patient has had hypertension at a young age and the following blood test results on his U&Es, what is the next investigation to perform to confirm the likely diagnosis Sodium 146 (135 -145) Potassium 3. 4 (3. 5 -5. 0) Urea and Creatinine normal a) Fasting glucose b) 2 hour glucose tolerance test c) Aldosterone: renin ratio d) Calcium profile e) Water-deprivation test 18
Practice Question A patient has had hypertension at a young age and the following blood test results on his U&Es, what is the next investigation to perform to confirm the likely diagnosis Sodium 146 (135 -145) Potassium 3. 4 (3. 5 -5. 0) Urea and Creatinine normal a) Fasting glucose b) 2 hour glucose tolerance test c) Aldosterone: renin ratio d) Calcium profile e) Water-deprivation test 19
Diabetes Insipidus • Central (lack of ADH production) – Pituitary surgery – Irradiation – Trauma • Nephrogenic (resistance to ADH effects) – Hypercalcaemia – Hypokalaemia – Medications e. g. lithium
Fluid deprivation test
Fluid deprivation test • Normal or primary polydipsia: urine concentrates immediately after fluid restriction • Cranial DI: urine concentrates only after DDAVP administration • Nephrogenic DI: urine never concentrates
Practice Question VSA-type A woman with polyuria and polydipsia with a normal fasting glucose is sent for a water deprivation + DDAVP (desmopressin) test. Her results are below Start: urine volume 0 ml, urine osmolality 200 m. Osm/kg 8 hrs fluid restriction: urine volume 2 litres, urine osmolality 230 m. Osm/kg 16 hrs (8 h post DDAVP): urine volume 2. 4 litres, urine osmolality 880 m. Osm/kg What is the likely diagnosis? 23
Practice Question VSA-type A woman with polyuria and polydipsia with a normal fasting glucose is sent for a water deprivation + DDAVP (desmopressin) test. Her results are below Start: urine volume 0 ml, urine osmolality 200 m. Osm/kg 8 hrs fluid restriction: urine volume 2 litres, urine osmolality 230 m. Osm/kg 16 hrs (8 h post DDAVP): urine volume 2. 4 litres, urine osmolality 880 m. Osm/kg What is the likely diagnosis? Answer: Fluid restriction did not concentrate the urine, but DDAVP administration did, therefore this is cranial DI 24
Contents • Sodium balance • Potassium • Enzymes and cardiac markers • Renal (AKI, CKD) • Metabolic disorders • Paediatric clinical chemistry Brief overview Will not be covered in this lecture – can be found in the path guide
Potassium • Normal range 3. 5 – 5. 5 mmol/l
Hypokalaemia • Potassium < 3. 5 m. M • Causes: – GIT losses: vomiting, diarrhoea – Redistribution into cells, insulin, salbutamol, alkalosis – Renal losses: Conn’s, loop diuretics (and Barter’s syndrome), thiazide diuretics (and Gitelman syndrome), renal tubular acidosis – Very poor dietary intake
Na+ Cl. Cortex Na+ delivery to distal nephron Thiazide diuretics Gitelman syndrome Medulla Na+ K+ Cl- Loop diuretics Bartter syndrome
Hypokalaemia • Clinical features – Muscle weakness – Cardiac arrhythmia – Polyuria & polydipsia (nephrogenic DI) • Treatment – Mild: Sando. K (2 tablets TDS for 3 days and monitor) – Severe: IV KCI (<10 m. M/hr) – Treat the cause – Correct Mg
Practice Question Which of the following drugs is most likely to contribute to hypokalaemia in a patient? a) Spironolactone b) Digoxin c) Lithium d) Frusemide e) Ramipril 30
Practice Question Which of the following drugs is most likely to contribute to hypokalaemia in a patient? a) Spironolactone b) Digoxin c) Lithium d) Frusemide e) Ramipril 31
Hyperkalaemia • Potassium > 5. 5 m. M • Causes: – Spurious sample – Extracellular shift • Acidosis • Rhabdomyolysis – Decreased excretion • Renal: AKI, CKD • Drugs: spironolactone, ACE inhibitors • Addison’s
Hyperkalaemia • Potassium > 5. 5 m. M • Causes: – Spurious sample – Extracellular shift • Acidosis • Rhabdomyolysis – Decreased excretion • Renal: AKI, CKD • Drugs: spironolactone, ACE inhibitors • Addison’s • Investigations to identify the cause: – Repeat sample! • VBG to also look for acidosis – CK – Creatinine and urea – Cortisol / short syn. ACTHen test
Potassium release from cells • Rhabdomyolysis K+ • Acidosis H+ K+ Need to maintain electroneutrality
Hyperkalaemia • ECG changes: – Tall tented t-waves – Broad QRS – Bradycardia – Loss of p-waves
Peaked T waves
Treatment of hyperkalaemia • 10 ml 10% calcium gluconate • Protects the myocardium but does not decrease the level of potassium • • 10 units insulin with 50 ml 50% dextrose Nebulised salbutamol Dialysis Treat the cause
Practice Question What is the likely cause of hyperkalaemia in a patient with the following blood test results: Sodium 140 (135 -145) Bicarbonate 16 (22 -26) Creatine kinase 1600 (<200) a) b) c) d) e) Potassium 6. 2 (3. 5 -5. 0) Creatinine 210 (30 -90) Glucose 7. 2 (3. 4 -6. 0 fasted) Acute kidney injury Metabolic acidosis Rhabdomyolysis Spironolactone Diabetic ketoacidosis 38
Practice Question What is the likely cause of hyperkalaemia in a patient with the following blood test results: Sodium 140 (135 -145) Bicarbonate 16 (22 -26) Creatine kinase 1600 (<200) a) b) c) d) e) Potassium 6. 2 (3. 5 -5. 0) Creatinine 210 (30 -90) Glucose 7. 2 (3. 4 -6. 0 fasted) Acute kidney injury Metabolic acidosis Rhabdomyolysis Spironolactone Diabetic ketoacidosis 39
Contents • Sodium balance • Potassium • Enzymes and cardiac markers • Renal (AKI, CKD) • Metabolic disorders • Paediatric clinical chemistry Brief overview Will not be covered in this lecture – can be found in the path guide
Enzymes and cardiac markers • • • Amylase CK Troponin ALP BNP
Amylase • Typically raised in acute abdominal pathology • Very high serum levels (usually >10 x ULN) in acute pancreatitis
CK • Creatine Kinase • Marker of muscle damage • Causes: – Physiological: Afro-Carribean, body-builders – Pathological: Duchenne Muscular Dystrophy (>10 x ULN), statin related myopathy, rhabdomyolysis
Troponin • Myocardial injury biomarker • Serial measurements particularly useful • Measure at 6 h, then at 12 h after onset of chest pain (remains elevated for 3 -10 days) • In clinical practice, often measured at 2 h intervals
ALP • Alkaline phosphatase • Present in high concentrations in liver, bone, intestine and placenta • To differentiate liver from bone ALP you can measure another organ-specific enzyme e. g. GGT • Causes: – Physiological: pregnancy – Pathological: • >5 x ULN: bone (e. g. Paget’s – isolated rise), liver (cholestasis – will also have raised GGT) • <5 x ULN: bone (tumours, fractures), liver (hepatitis)
BNP • Brain natriuretic peptide • Released from ventricles in the heart in response to ventricular stretch • Levels <100 are highly specific for excluding heart failure • Levels >400 highly sensitive for heart failure
Contents • Sodium balance • Potassium • Enzymes and cardiac markers • Renal (AKI, CKD) • Metabolic disorders • Paediatric clinical chemistry Brief overview Will not be covered in this lecture – can be found in the path guide
Acute kidney injury • Considered a medical emergency • Causes: – Pre-renal: usually hypovolaemia • Treatment: volume replacement – Renal: vascular, glomerular, tubular, interstitial • Treat the cause – Post-renal: usually obstruction e. g. BPH, ureteric stone • Treatment: relieve the obstruction
Chronic kidney disease • Causes: – Diabetes & hypertension – Others: atherosclerotic renal disease, glomerulonephritis , polycystic kidney disease
Chronic kidney disease • Complications are related to the primary functions of the kidney • Progressive failure of homeostatic function – Acidosis • Progressive failure of hormonal function – Anaemia (loss of EPO synthesis) – Renal Bone Disease (secondary hyperparathyroidism due to low Vit D) • Progressive failure to maintain water balance – Fluid overload • Progressive failure to maintain electrolyte balance – Hyperkalaemia • Cardiovascular disease – Vascular calcification and subsequent atherosclerosis (biggest mortality in CKD) • Uraemia and Death
Indications for dialysis • Remember your vowels: A E I O • • • U Acidosis (metabolic) Electrolytes (refractory hyperkalaemia) Ingested toxins Overload (pulmonary oedema) Uraemia (symptomatic)
Renal replacement therapy • Dialysis – Haemodialysis • Via central line or AV fistulae (requires surgery to create) • Usually done 3 x/week in hospital – Peritoneal dialysis • Done via a Tenckoff catheter – uses peritoneum as the dialysis membrane • Can be done at home • Increased risk of infections • Renal transplant – The only definitive cure – Requires life long immunosuppression
Thank you for listening! Any questions? Feedback link: https: //forms. gle/P 3 X 31 X 9 WEUxgawb 36