MRI Anatomy of the Shoulder Functional Anatomy Glenohumeral




























 Anterior clavicular fibres – arise from superior anterior aspect of lateral")




 • • • Thick triangular muscle which occupies most of the infraspinatous")



 Origin: Superior part of lateral border of scapula Insertion: Inferior facet")
 Axial The")




















 in direct AP")








- Slides: 70
MRI Anatomy of the Shoulder
Functional Anatomy Glenohumeral joint is a ball and socket synovial. Glenoid cavity inherently unstable. Stability provided by: i) Static constraints - 3 glenohumeral ligaments - glenoid labrum - joint capsule • Dynamic constraints, rotator cuff muscles counteract the action of the deltoid by preventing the head of the humerus from moving superiorly when the arm is raised
The glenohumeral joint has the following supporting structures: Superiorly Coraco-acromial arch Long head of the biceps tendon Tendon of supraspinatus muscle Anteriorly Anterior labrum 3 Glenohumeral ligaments -SGHL, MGHL, IGHL (anterior band) Subscapularis tendon Posteriorly Posterior labrum Posterior band of the IGHL Infraspinatus tendon Teres minor tendon
Articular surfaces The shoulder joint is composed of 3 bones and five articulations. Bones: Scapula Humerus Clavicle Articulations: Glenohumeral joint Acromio-clavicular joint Scapulothoracic joint Sternoclavicular joint Coracoclavicular joint
Joint capsule • Attached proximally to the glenoid labrum • Attached distally to the anatomical neck of the humerus • Capsule is thickened anteriorly by glenohumeral ligaments • Herniation of synovial membrane through an anterior defect in capsule & glenohumeral ligaments forms the subscapular bursa
Subdeltoid Between joint capsule and deltoid muscle Subcoracoid Between joint capsule and coracoid process Coracobrachial Between subscapularis and coracobrachialis Subacromial Between joint capsule and acromion Subscapular bursa Between joint capsule and subscapularis tendon Bursae
Rotator Interval • Triangular space between the supraspinatus and subscapularis tendons – Contains long head of biceps and SGHL – Acts to prevent anterior dislocation of the shoulder
Ligaments • 3 glenohumeral ligaments – Superior – Middle – Inferior • Coracohumeral ligament • Transverse humeral ligament – Between greater and lesser tuberosities of humerus, maintains long head of biceps in bicipital groove
Superior glenohumeral ligament Coracohumeral ligament Long head biceps tendon
SGHL Sagittal
SGHL Axial
Middle glenohumeral ligamant
MGHL Sagittal
MGHL Axial
Inferior glenohumeral ligament Axillary recess Subacromialsubdeltoid bursa
Glenoid labrum • The glenoid labrum is a fibrocartilaginous structure that attaches to the glenoid rim and is about 4 mm wide. • increases the superior-inferior diameter of the glenoid by 75% and the anterior-posterior diameter by 50% • Anteriorly, the glenoid labrum blends with the anterior band of the inferior glenohumeral ligament. • Superiorly, it blends with the biceps tendon and the superior glenohumeral ligament. • It is usually rounded or triangular on cross-sectional images.
Labral anatomy: Axial • The normal labrum demonstrates low signal intensity on all pulse sequences, due to the lack of mobile protons in this dense fibrocartilage. • On cross sectional imaging, the normal labrum is most commonly triangular, but can also be round, cleaved, notched, flat, or absent.
Labral Anatomy: Coronal • A fat suppressed oblique coronal T 2 weighted MR image demonstrates homogeneously low signal intensity in the normal superior labrum.
Labral variants • These normal variants are all located in the 11 -3 o'clock position.
• It is important to recognise these variants, because they can mimick a SLAP tear. • These normal variants will usually not mimick a Bankartlesion, since these are located at the 3 -6 o'clock position, where these normal variants do not occur.
Sublabral recess Synovial recess between the superior labrum and the glenoid rim created by the attachment of the biceps tendon on the supraglenoid tubercle. Because of this recess, the labrum does not attach to the glenoid rim at the 12 o'clock position. There are 3 types of attachments of the superior labrum: Type I No recess between glenoid cartilage and labrum Type II Small recess. Type III Large sublabral recess.
Sublabral Foramen An unattached anterosuperior labrum at the 1 -3 o'clock position. Anterior to biceps tendon It is seen in 11% of individuals. Not to be confused with a sublabral recess or SLAP-tear, which are also located in this region.
Differences between an sublabral recess and a SLAP-tear: A recess more than 3 -5 mm is always abnormal and should be regarded as a SLAPtear.
Buford complex Congenital labral variant 2 Features: Anterosuperior labrum is absent in the 1 -3 o'clock position Middle glenohumeral ligament is usually thickened. It is present in approximately 1. 5% of individuals.
Os Acromiale Results from failure of one of the acromial ossification centers to fuse. 5% of the population. Usually an incidental finding, regarded as a normal variant. May cause impingement because if it is unstable, it may be pulled inferiorly during abduction by the deltoid, which attaches here. On MR an os acromiale is best seen on superior axial images.
Acromion: 3 types Type 1 is a flat undersurface with a high angle of inclination. Type 2 is a curved arc and decreased angle of inclination. Type 3 is hooked anteriorly with a decreased angle of inclination.
Axial Anatomy
The axillary artery begins at the lateral border of the first rib as a continuation of the subclavian artery. It changes its name to brachial artery at lower inferior border of the teres major muscle (8).
Axial Deltoid 1) Anterior clavicular fibres – arise from superior anterior aspect of lateral clavicle 1) Lateral acromial fibres – arise from superior aspect of acromion process 1) Posterior fibres – arise from posterior border of spine of scapula
Supraspinatus muscle Relatively small muscle Runs from the supraspinatous fossa of scapula to the greater tubercle of the humerus Axial
Axis of supraspinatous tendon The supraspinatus tendon is the most important structure of the rotator cuff and subject to tendinopathy and tears. Tears of the supraspinatus tendon are best seen on coronal oblique and ABER-series. In many cases the axis of the supraspinatus tendon (arrowheads) is rotated more anteriorly compared to the axis of the muscle (yellow arrow). When you plan the coronal oblique series, it is best to focus on the axis of the supraspinatus tendon.
The attachments of the 3 rotator cuff muscles that insert onto the greater tubercle of the humerus Sagittal can be abbreviated SIT when viewed from superior to inferior: post Supraspinatus Infraspinatus Teres minor post SITS inlcudes Subscapularis which inserts onto the lesser tubercle of the humerus
Axial Pec major Deltoid anterior Pec minor Supraspinatus inserts most superiorly to greater tuberosity humeral head Subscapularis Infraspinatus Deltoid posterior
Infraspinatus (SIT) • • • Thick triangular muscle which occupies most of the infraspinatous fossa Attaches medially to the infraspinatus fossa and laterally to the middle facet of the greater tubercle of the humerus Trapezoidal insertion of infraspinatus onto humerus is much larger than the insertion of the supraspinatus
Coronal oblique MRI *Tip* • Supraspinatus – fibres run horizontally • Infraspinatus – fibres have a slightly oblique orientation
Subscapularis Large triangular muscle which fills the subscapular fossa Inserts onto the lesser tubercle of the humerus Subscapular fossa = anterior Infraspinatous fossa = posterior ant post
Axial Deltoid as one Coracobrachialis Teres minor Coracobrachialis is the smallest of the three muscles that attach to the coracoid process. The other 2 muscles are pectoralis minor and biceps brachii. Distal insertion upper medial aspect of arm
Teres minor (SIT) Origin: Superior part of lateral border of scapula Insertion: Inferior facet of greater tuberosity of humerus
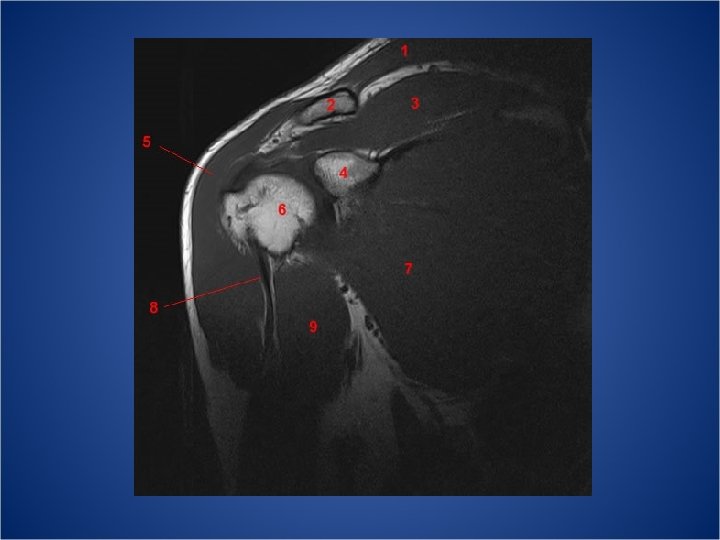
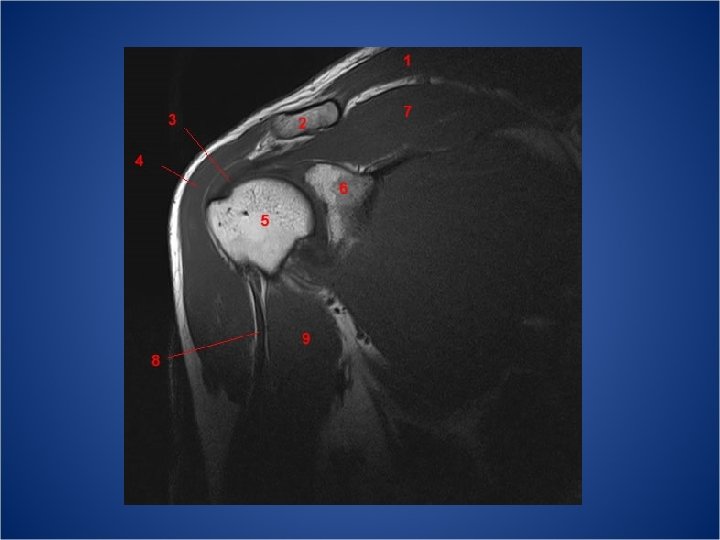
The short head of the biceps originates from the coracoid process (2) Axial The long head originates from the supraglenoid tubercle (3)
Tendon of long head passes down along the intertubercular/bicipital groove of the humerus into the joint capsule Both heads arise on the scapula and join to form a single muscle belly which is attached to the upper forearm. Long head forms biceps-labral complex with superior glenohumeral ligament When the humerus is in motion, the tendon of the long head is held firmly in place in the bicipital groove by the greater and lesser tubercles and the overlying transverse humeral ligament.
Coronal Long head
Coronal anatomy
Coronal Trapezius Posterior humeral circumflex artery and axillary nerve Triceps Teres major extends longitudinally from the occipital bone to the lower thoracic vertebrae and laterally to spine of the scapula
Teres major It arises from the dorsal surface of the inferior angle of the scapula Inserts onto intertubercular sulcus of humerus (Teres minor)
Coronal Infraspinatus Teres minor Triceps Teres major
Coronal Supraspinatus Subscapularis Teres major
Sagittal Anatomy
Sagittal P A
Acromioclavicular joint Axial: Clavicle medial Acromion lateral Sagittal: Acromion posterior Coracoid anterior The undersurface of the acromion should align with the undersurface of the clavicle Cl Ant Co Ac Post
Sagittal: SIT
MR shoulder arthrogram • Technique whereby injection of contrast media into the joint allows for evaluation of capsule and internal joint structures. • Originally performed using plain radiography. • Now injection of gadolinium allows MR arthrography. • CT arthrograms can also be performed.
Advantages • Joint distension, outlining intra-articular structures • Improved detection of tears, including articular surface partial tears • Demonstration of communication between joint and extra-articular abnormalities eg. Paralabral cysts and bursae.
Disadvantages and pitfalls • Risks assoc with needle placement into joint: infection, haemorrhage, synovial reaction. • Avoid oblique position – glenoid in profile – aiming for joint space places the labrum at risk • Correct needle positioning is essential – Extra articular contrast can complicate findings on MR and simulate tears
Technique • Fluoroscopically guided anterior approach is most widely performed. • Perform routine preparation – – – Correct patient Correct side No iodine allergies Explain procedure to patient, obtain consent Confirm indication
Indications • • Assessment of integrity of rotator cuff Evaluation of shoulder instability Diagnosis of labral pathology Diagnosis of adhesive capsulitis
Technique • Sterile procedure • Fluoroscopically guided • Obtain control images of shoulder – Patient supine, AP view – Arm in external and internal rotation – Angle tube to view acromion in profile – clear visualisation of sub-acromial space – Evaluate for calcium deposition in tendons
Patient Positioning • Supine position creates oblique orientation of glenoid surface. • Posterior glenoid overlaps humeral head on AP • Anterior glenoid lies medial to humeral head • Thus needle directed AP at humeral head will not injure anterior labrum • External rotation exposes a larger articular surface anteriorly • Placing a sandbag in the patient’s hand may help maintain the position
Technique • Determine skin entry site using fluoroscopy • Just lateral to the medial cortex of the humeral head (never medial) • At junction of middle and lower third of humeral head • Ideally central in fluoroscopic image • Locally anaesthetise skin and subcutaneous tissue
Technique • Prepare contrast whilst allowing local anaesthetic to take effect (can also be done before procedure starts) • Bloem protocol: – – – 20 ml syringe 10 ml sterile water 5 ml iodine based non-ionic LOCM (eg. Ultravist, Omnipaque) 5 ml lignocaine 0. 1 ml gadolinium • Other: – Test injection with 1 -2 ml of lignocaine – Contrast: 10 ml saline, 10 ml Iodine LOCM, 0. 1 ml gadolinium, 0. 3 ml 1: 1000 adrenaline • Syringe connected to connecting catheter(line)
Technique • Advance needle (usually 20 G spinal needle with stylet) in direct AP direction posteriorly. • Continue until contact with humeral head. • Consider test injection with lignocaine. • Should only meet low resistance when in joint space • If high resistance – possibly in hyaline cartilige – carefully manipulate needle by rotation and minimal retraction (few mm) • Loss of resistance indicates either intra-articular or bursal location
Technique • Inject iodinated contrast to distinguish between intra-articular and bursal location • Intra-articular contrast will collect in glenohumeral joint space • If intra-articular position is confirmed, continue with proper contrast injection • Usually inject 14 – 16 ml of contrast, depending on patient and pathology.
Alternative: Posterior approach • When suspecting anterior pathology. • Avoids the interpretative difficulties that may be associated with anterior extracapsular contrast extravasation • Aim for the inferomedial quadrant of humeral head within boundary of anatomic neck (interrupted line).
Other techniques • Inject only water, no gadolinium – Achieves effect of distension – Need to use T 2 sequences – Disadvantage: • Difficult to distinguish between small full thickness and partial tears • Indirect arthrogram – – – 1 mmol/kg Gd IV Exercise joint for 5 to 5 minutes Gd passes into joint space Can perform T 1 images Disadvantages: • Joint not distended • Extra-articular structures will also enhance
MR technique • Three plane T 1 with fat sat • T 2 with fat sat axial and coronal oblique (Consider Ax GRE to evaluate for calcification) • Sagittal oblique T 1/PD without fat suppression • Some protocols suggest pre contrast T 2 sequences. – Detection of intra-substance and bursal surface tears. – Pre-existing fluid collections and cysts • Coronal oblique parallel to supraspinatus tendon (not muscle) • Sagittal oblique perpendicular to glenoid surface • (ABER – Abduction and External rotation sometimes used for evaluation of anterior and inferior GHL’s)
ABER view Images in the ABER position are obtained in an axial way 45º off the coronal plane (figure). In that position the 3 -6 o'clock region is imaged perpendicular. Labral tears The abduction external rotation (ABER) view is excellent for assessing the anteroinferior labrum at the 3 -6 o'clock position, where most labral tears are located. Inferior glenohumeral ligament stretched resulting in tension on the anteroinferior labrum, allowing intraarticular contrast to get between the labral tear and the glenoid. Rotator cuff tears Very useful for both partial- and full-thickness tears of the rotator cuff. Releases tension on the cuff relative to the normal coronal view obtained with the arm in adduction.
Rotator cuff tears • Arthrography improves detection of tears as the joint is being distended and contrast forced into small defects. • T 1 (quicker) sequences with improved SNR can be used • Diagnoses full thickness tears and articular surface partial thickness tear • Not of value in intra-substance or bursal surface partial thickness tears
• Full-thickness tear will demonstrate the gadolinium contrast solution extending first through a defect in the cuff and then into the subacromial-subdeltoid bursa. • Articular-surface partial-thickness tears show a focal extension of the contrast solution into the substance of the tendon. • Fat suppression is necessary as peribursal fat may mimic contrast.
References • • • Ryan S, Mc. Nicholas M, Eustace S. Anatomy for diagnostic imaging. CT and MR Arthrography of the Normal and Pathologic Anterosuperior Labrum and Labral-Bicipital Complex. October 2000 Radio. Graphics, 20, S 67 -S 81. www. radiologyassistant. nl Radiology Assistant: MR Shoulder Part I. http: //musculoskeletal-radiology. blogspot. com/2006/09/glenohumoralligaments. html Jacobson et al. Aids to Successful Shoulder Arthrography Performed with a Fluoroscopically Guided Anterior Approach. Radiographics. 2003; 23: 373– 379 Beltran et al. MR Arthrography of the Shoulder: Variants and Pitfalls. Radiographics. 1997; 17: 1403 -14 12