Glenohumeral shoulder Joint By Cameron Debbie Laura and
 Joint By: Cameron, Debbie, Laura and Wendy")
Glenohumeral (shoulder) Joint By: Cameron, Debbie, Laura and Wendy

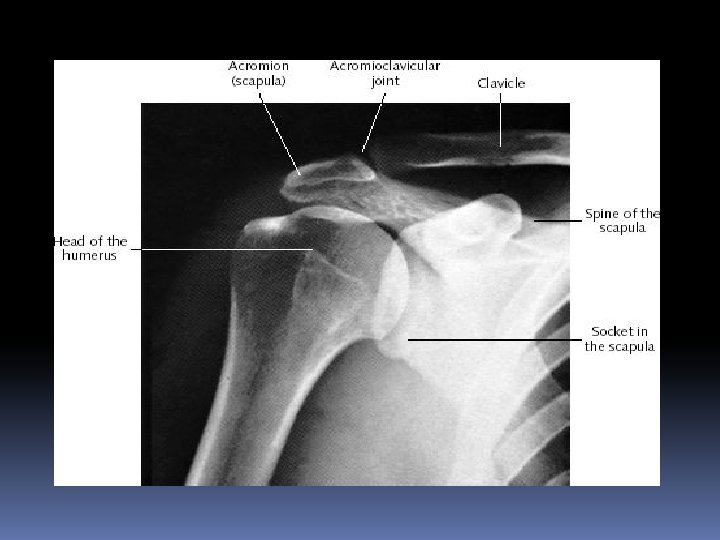
Humerus Greater tubercle Lesser Tubercle Intertubercular Sulcus Head Anatomical Neck Surgical Neck Detloid tuberosity

Anterior Scapula Acromion process Coracoid process Borders: Superior Vertebral Axillary Angles: Superior Inferior Fossae: Subscapular Glenoid cavity Superior angle Superior border Subscapular fossa Coracoid process Acromion process Glenoid cavity Axillary border Vertebral border Inferior angle

Posterior Scapula Acromion process Fossae: Infraspinatous Supraspinatous Spine Glenoid cavity Angles: Superior Inferior Borders: Superior Vertebral Axillary Acromion process Glenoid cavity Axillary border Superior angle Supraspinatous fossa spine Infraspinatous fossa Vertebral border Inferior angle

Clavicle Acromial End Conoid Tubercle

Cartilage Articular Cartilage Glenoid Labruim

Ligaments • Coracohumeral • Glenohumeral • Transverse humeral • Coracoclavicular • Conoid • Superior transverse scapular • Acromioclavicular Glenohumeral ligament

Bursae Subscapular , Subacromial Subdeltoid, Subcoracoid

Articular Capsule Articular Cavity is filled with Synovial fluid, which is secreted by the synovial membrane. Synovial membrane is the inner layer, Fibrous layer is the outer layer. Bursae also have synovial fluid inside them.

Articular Capsule Synovial Membrane Fibrous Layer
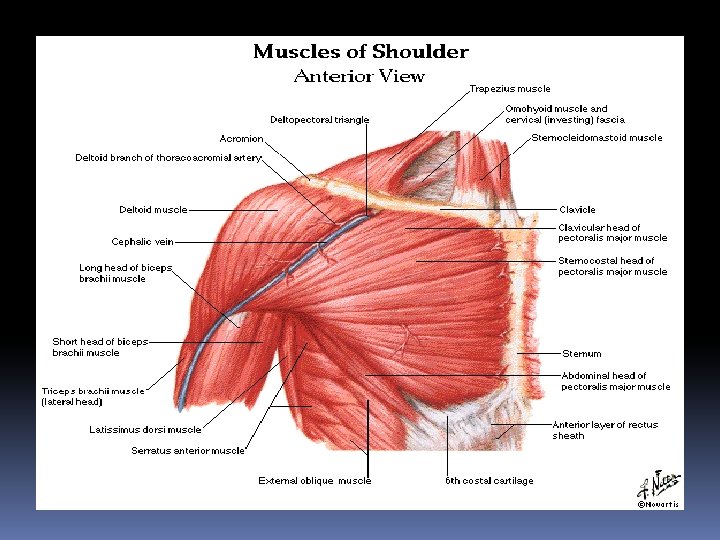

Red = origin Blue = insertion
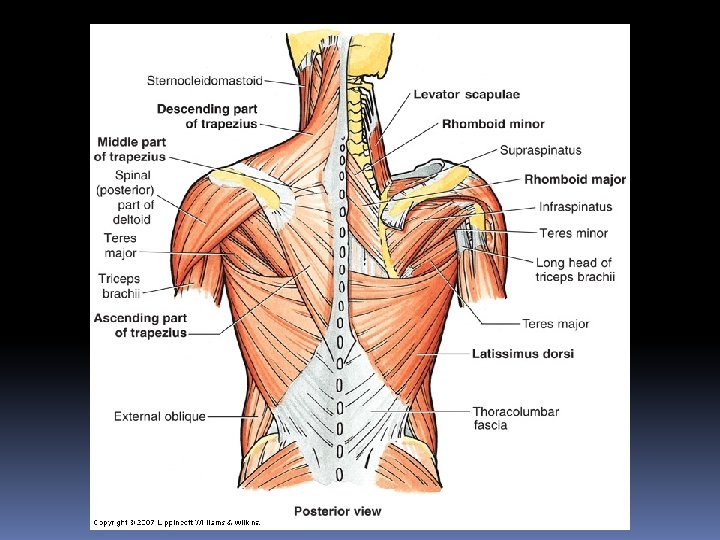

Red = origin Blue = insertion

Innervation

Innervation and Vascular Supply

Vascular supply and Innervation

Vascular Supply

Anterior Surface Anatomy

Posterior Surface Anatomy

Physical Therapy Protocol Torn Rotator Cuff

Ruptured Supraspinatus Tendon

The Muscles of the Rotator Cuff S. I. T. S. Suprasinatous Infraspinatous Teres Minor Subscapularis

Rotator Cuff Repair Rehab Protocol General Considerations: Quality of tissue and integrity of repair Acute vs. chronic tear Chronic repairs typically harder to achieve ROM Extent of repair Early PROM of glenohumeral joint is important to prevent capsular adhesions and fibrosis. This is done in a range that SHORTENS involved mm PT will start immediately following surgery, focus on ROM

0 -2 Weeks Post-Op Protection, Dressing, PROM AROM, Pain control, Other Activities Keep shoulder in a sling unless showering or during exercise. Biceps curls, putty grip, neck stretches as tolerated. Okay to shower after 2 days. Stitches removed 8 -10 days. PROM=flexion, pendulums, pulleys. STM, modalities for pain control. Walking, bike.

2 -4 Weeks Post-Op Protection, PROM, AROM Isometrics, Other Activities Still in sling unless showering, meals, or exercise. ISO. For Uninvolved tendons as tolerated. PROM for repaired tendons, only in direction that SHORTENS tendon. AROM for Uninvolved tendons. AVOID STRESSING REPAIRED TENDONS!! LE conditioning, aquatic therapy.

4 -8 Weeks Post-Op Protection, PROM, Mobs AROM, Other Activities No sling needed. GENTLE PROM into previously protected ranges. Most plane motions should be 75% of normal. Make sure and check glenohumeral joint for excessive loss of mobility. Grade 1 -2 w/o restrictions. Pure ABD. and ER. Slowly introduce against gravity ROM exercises into extension.

8 -12 Weeks Post-Op PROM, Mobs, AROM, Other Activities Cont. w/ Passive stretching to pain tolerance. Progress to high repetitions and then increase resistance. Grade 1 -4 mobs. As tolerated. MONITOR SHOULDER AND POSTURAL MECHANICS AS WELL AS PAIN WITH ALL EXERCISES. Jogging, UBE for ROM.

3 -6 Months Post-Op ROM Other Activities If ROM is still limited, focus on achieving full ROM. Rowing, UBE for strengthening, weightlifting with extreme caution NOT to stress repair!!! If ROM is not limited, focus on strengthing. Motion in most planes should be almost normal. More aggressive stretching and resistive exercises.
 ROM Other Activities Hard resistive exercises, aggressive stretching. Swimming, weightlifting,")
6 Months(M. D. Visit) ROM Other Activities Hard resistive exercises, aggressive stretching. Swimming, weightlifting, throwing progression.

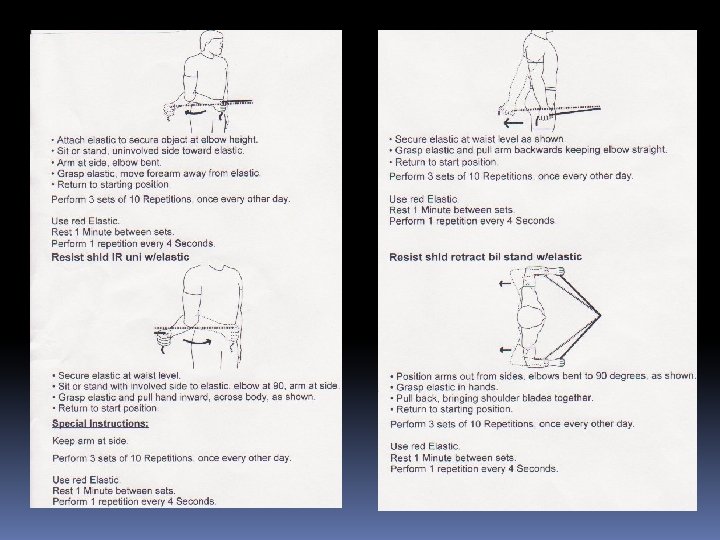
Exercise Program

- Slides: 35