Adult nursing Caring for Clients With Hematologic and






 Folic acid ◦ ◦ Chronic malnourishment Glossitis Cheilosis Diarrhea")
, chronic")







 Primary type Production of all blood cells increased Cause unknown Insidious")













 Hemophilia B (Christmas disease) ◦ Less common ◦ Deficiency in Factor IX")


 Simultaneous blood clotting and hemorrhage Intrinsic and/or extrinsic clotting cascades")


")













 Client Teaching (continued) ◦ ◦ ◦ Avoid crowds, sick")







 Dietary Considerations ◦ Iron that is readily absorbed ◦ Iron")


 Bone marrow transplantation ◦ Allogenic ◦ Eliminate leukemic cells ◦")
 Stem cell transplant ◦ Donor treated with colony-stimulating factors to")





")




 Impaired Oral Mucous Membranes ◦ ◦ ◦ ◦ Assess")
 Self-Care Deficit ◦ Assist with ADL ◦ Rest periods")
 Evaluation ◦ ◦ Independent ADL Increased level of activity")


 Risk for Infection ◦ ◦ ◦ Infection precautions Avoid")
 Imbalanced Nutrition: Less than Body Requirements ◦ Monitor weight")
 Impaired Oral Mucous Membranes ◦ ◦ ◦ Assess mouth")
 Ineffective Protection ◦ ◦ ◦ Monitor LOC Report manifestations")
 Anticipatory Grieving ◦ Therapeutic communication ◦ Manage stressful situations")
 Evaluation ◦ ◦ ◦ Freedom from infection Weight Food")

 Fatigue ◦ ◦ ◦ Assess malaise Encourage talking")
 Disturbed Body Image ◦ ◦ ◦ Body image")

 Impaired Physical Mobility ◦ ◦ Reposition Change positions")




 Impaired Gas Exchange ◦ ◦ ◦ O 2 saturation")
 Acute Pain ◦ Pain scale ◦ Handle gently ◦")
 Fear ◦ ◦ ◦ ◦ Verbalize concerns Answer questions")

 ◦ ◦ Antiembolic stockings/intermittent pressure devices Elevate extremities Skin")
- Slides: 101
Adult nursing Caring for Clients With Hematologic and Lymphatic Disorders
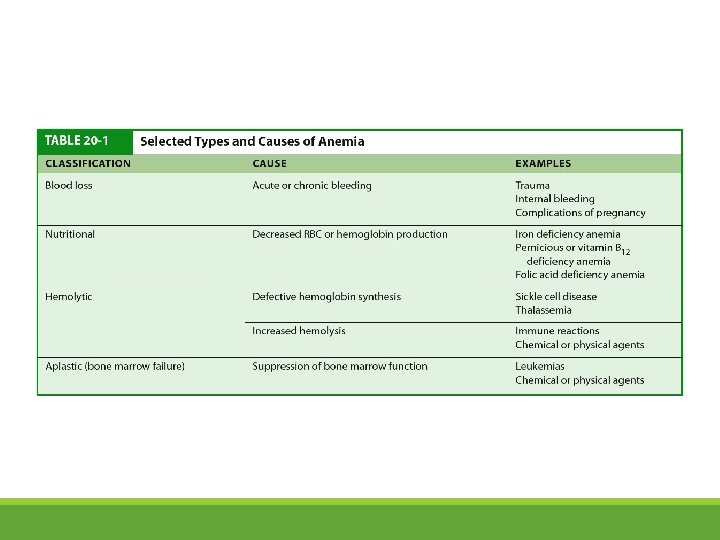
Anemia Hemoglobin concentration or number of circulating RBCs decreased Caused by ◦ Impaired RBC formation ◦ Excessive loss or destruction of RBCs
Anemia - Pathophysiology Reduces the oxygen-carrying capacity of the blood Causes tissue hypoxia Body attempts to restore oxygen delivery
Anemia - Manifestations Pallor Bone pain Angina Headache Fatigue Dizziness Dyspnea on exertion Dim vision Night cramps
Blood Loss Anemia Acute or chronic bleeding Both lead to anemia RBCs normal but reduced in number
Nutritional Anemia Lack of nutrients for RBC formation or development Iron deficiency ◦ Cheilosis (cracks at corners of mouth) ◦ Smooth, sore tongue ◦ Pica Vitamin B 12 ◦ Pernicious anemia ◦ Paresthesias
Nutritional Anemia (continued) Folic acid ◦ ◦ Chronic malnourishment Glossitis Cheilosis Diarrhea
Anemia of Chronic Disease Seen in AIDs, rheumatoid arthritis, inflammatory bowel disease (IBD), chronic hepatitis, chronic renal failure (CRF) Severity depends on the severity of underlying disease Manifestations similar to iron deficiency anemia
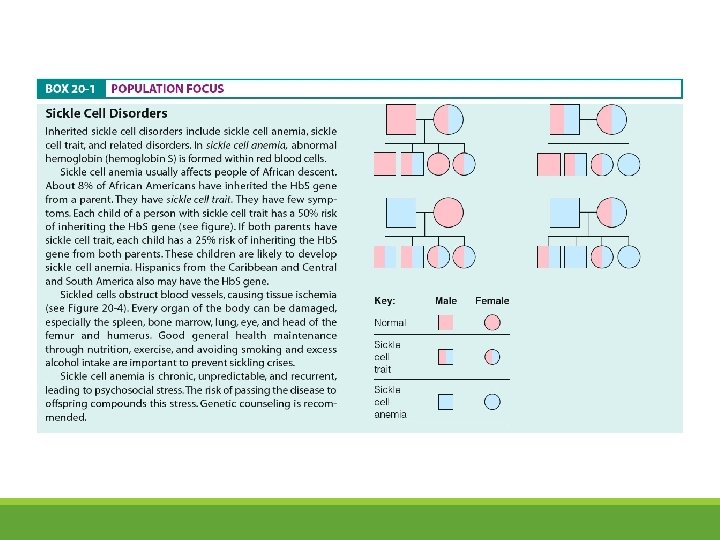
Hemolytic Anemias Premature destruction of RBCs Intrinsic or acquired causes Sickle cell disorders ◦ Abnormal Hgb, changes shape ◦ Intense pain, chest, back, joints
Sickle Cell Anemia
Thallassemia Inherited; caused by abnormal Hgb synthesis Liver and spleen enlarged Target cells
Acquired Hemolytic Anemias Damage by outside factors ◦ ◦ Mechanical trauma Antibody reactions Immune responses Drugs, toxins, chemical agents, venoms
Aplastic Anemia Bone marrow fails to produce RBCs Cause unknown Pancytopenia
Myelodysplastic Syndrome Group of stem cell disorders Seen in older adults Anemia, enlarged spleen
Polycythemia Erythrocytosis Abnormally high RBC count, high Hct Blood sticky Secondary form is the most common Develops due to chronic hypoxemia or excess erythropoietin
Polycythemia Vera (continued) Primary type Production of all blood cells increased Cause unknown Insidious onset Gangrene complication
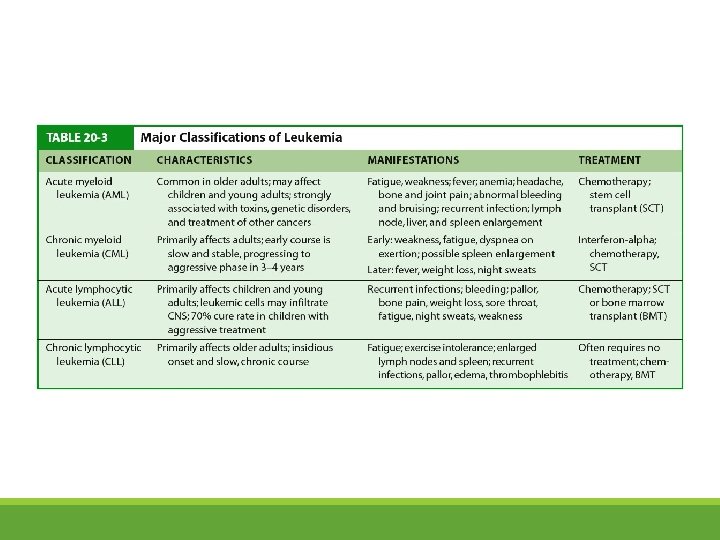
Leukemia Group of malignant disorders of WBCs Greater numbers of WBCs Cause of most unknown Classified by onset and duration: acute or chronic Four types
Leukemia - Pathophysiology Malignant transformation of a single stem cell Cells proliferate slowly, nonfunctional WBCs Bone marrow filled with leukemic cells Leave bone marrow and infiltrate other tissues Death from hemorrhage or infection
Leukemia - Manifestations Anemia Infection Bleeding
The multisystem effects of leukemia
Malignant Lymphoma Cancer of lymph tissue Classified as Hodgkin or non-Hodgkin
Hodgkin Disease Most curable Painless progressive enlargement of one or more lymph nodes Reed-Sternberg cells Cause unknown
Non-Hodgkin Lymphoma More common Multiple lymph nodes involved
Multiple Myeloma cells replace bone marrow, infiltrate bone Bone weakened, pathologic fractures Bone/back pain most common symptoms Kidney damage
Neutropenia Disease of number of circulating neutrophils Usually secondary to infection, hematologic disease, chronic disease, chemotherapy Severe form is called agranulocytosis Can result in impaired WBC formation or increased WBC destruction Protective measures are required
Neutropenia - Manifestations Fatigue Weakness Sore throat Stomatitis Dyphagia Fever Chills
Thrombocytopenia Platelet count less than 100, 000 per m. L Common cause of abnormal bleeding Idiopathic thrombocytopenia purpura most common form ◦ Platelets destroy more rapidly than normal ◦ Autoimmune disorder
Thrombocytopenia Manifestations ◦ ◦ ◦ Purpura Ecchymosis Petechiae Epistaxis Menorrhagia Hematuria
Hemophilia Group of hereditary clotting factor deficiencies Hemophilia A ◦ Most common type ◦ Deficiency in Factor VIII
Hemophilia (continued) Hemophilia B (Christmas disease) ◦ Less common ◦ Deficiency in Factor IX Transmitted from mother to son Sex-linked recessive disorder on X chromosome
The inheritance pattern for hemophilia A and B. Both are X-linked recessive disorders; females may carry the trait, but only males develop the disorder.
Hemophilia - Manifestations Hemorrhages into body tissues
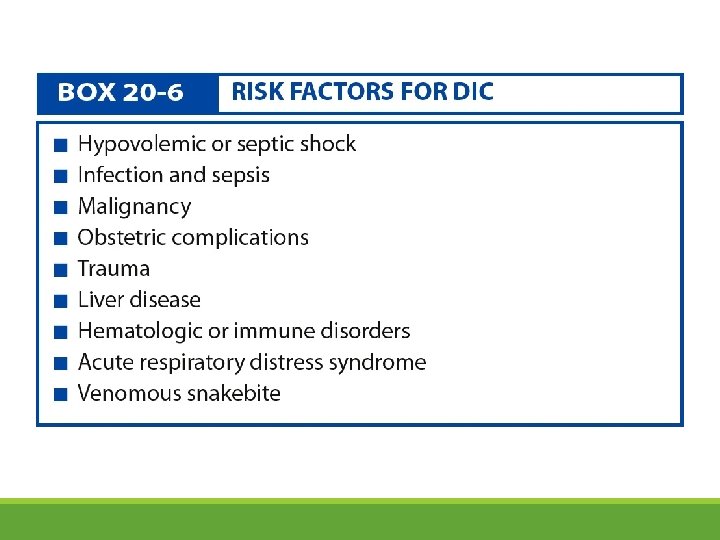
Disseminated Intravascular Coagulation (DIC) Simultaneous blood clotting and hemorrhage Intrinsic and/or extrinsic clotting cascades activated Widespread clotting of small vessels Clotting factors depleted; leads to bleeding
DIC - Manifestations Bleeding most obvious Tachycardia, hypotension Mottling Abdominal distention Decreased LOC
Lymphangitis/Lymphedema Lymphangitis ◦ Inflammation of lymph vessel Lymphedema ◦ Obstructed lymph vessel
Severe lymphedema of the lower extremity. (Source: NMSB, Custom Medical Stock Photos, Inc. )
Infectious Mononucleosis Acute infection caused by Epstein–Barr virus Benign and self-limiting Kissing disease
Infectious Mononucleosis Manifestations Headache Sore throat Fatigue Enlarged and painful lymph nodes Fever Enlarged spleen
Anemia – Diagnostic Tests CBC Iron levels Serum ferritin Sickle cell screening Hemoglobin electrophoresis Schilling’s test Bone marrow aspiration
Leukemia – Diagnostic Tests CBC with differential and platelet count Bone marrow
Multiple Myeloma – Diagnostic Tests Urine samples CBC Bone marrow Bone x-rays
Neutropenia - Diagnosis WBC count Neutophil count less than 1500 cells/mm 3 May be less than 500 cells/mm 3 in agranulocytosis
Thrombocytopenia – Diagnostic Tests CBC, platelet count Bone marrow Antinuclear antibodies
Hemophilia – Diagnostic Tests Platelet count Coagulation studies Clotting factors
DIC – Tests Clotting studies
Infectious Mononucleosis – Diagnostic Tests Increased lymphocytes and monocytes Increased WBC count Low platelets
Malignant Lymphoma – Diagnostic Tests Chest x-ray Abdominal CT Biopsy Ann Arbor staging system Cotswold staging classification system
Anemia – Nursing Implications Client Teaching ◦ ◦ ◦ Types of anemia Diet Medications Genetic counseling Follow-up appointments Support groups
Leukemia – Nursing Implications Client Teaching ◦ ◦ ◦ ◦ Diagnosis, treatment, bone marrow, complications Cancer as a chronic illness Balance activity with rest Maintain weight and nutrition Hydration Prevent infection Oral hygiene
Leukemia – Nursing Implications (continued) Client Teaching (continued) ◦ ◦ ◦ Avoid crowds, sick people Avoid immunizations Reduce risk of bleeding or injury Avoid OTC medications that can cause bleeding Refer to social services, support groups, home health
Malignant Lymphoma – Nursing Implications Client teaching ◦ ◦ ◦ ◦ Treatment and effects of treatment Skin care New symptoms Complementary pain management strategies Rest and exercise Diet American Cancer Society referral
Multiple Myeloma – Nursing Implications Client Teaching ◦ Teach S/S complications ◦ Hospice
Thrombocytopenia – Nursing Implications Client Teaching ◦ Continue treatment to maintain remission ◦ Long-term steroid treatment ◦ Splenectomy
Hemophilia – Nursing Implications Client teaching ◦ How to prevent bleeding ◦ Provide medications ◦ Genetic counseling
DIC – Nursing Implications Client teaching ◦ Proper foot care ◦ Heparin home therapy ◦ When to contact physician
Lymphangitis/Lymphedema Nursing Implications Client Teaching ◦ ◦ ◦ Use of pressure devices, elastic stockings Skin inspection Skin care Elevate extremity Activity, diet, diuretics
Anemia - Treatment Medications ◦ Depends on type and cause ◦ ◦ ◦ Iron replacement Vitamin B 12 Folic acid Hydroxyurea Immunosuppressive therapy or androgens
Anemia – Treatment (continued) Dietary Considerations ◦ Iron that is readily absorbed ◦ Iron sources Blood Transfusions ◦ Replace RBCs ◦ Whole blood or packed RBCs
Polycythemia - Treatment Reduce blood viscosity and volume Relieve symptoms Phlebotomy to keep blood volume within normal levels Chemotherapy
Leukemia - Treatment Chemotherapy ◦ Destroy leukemic cells ◦ Produce remission ◦ Achieve remission, cure, relieve symptoms Radiation therapy ◦ Shrink lymph nodes Biologic therapy ◦ Interferons, interleukins ◦ Colony-stimulating factors
Leukemia – Treatment (continued) Bone marrow transplantation ◦ Allogenic ◦ Eliminate leukemic cells ◦ Donor marrow transfused ◦ Autologous ◦ Own bone marrow withdrawn, treated, frozen, reinfused later
Leukemia – Treatment (continued) Stem cell transplant ◦ Donor treated with colony-stimulating factors to increase concentration of stem cells in blood ◦ Blood removed from donor, given to patient
Malignant Lymphoma - Treatment Chemotherapy ◦ Combination ◦ Remission in more than 75% Radiation ◦ Used for both ◦ Combined with chemotherapy
Areas of radiation for total nodal radiation therapy.
Multiple Myeloma Treatment No cure Relieving symptoms Death within 2 to 5 years Treatment ◦ Chemotherapy, radiation, medications, pain control, blood transfusions
Neutropenia - Treatment Discontinue drugs that may be cause of disorder Treat infection Filgrastim (Neupogen) may be used to treat disorder
Thrombocytopenia - Treatment Medications ◦ Steroids ◦ Immunosuppressive drugs Platelet transfusions Plasmapheresis Surgery: ◦ Splenectomy
Hemophilia - Treatment Replace clotting factors Fresh frozen plasma Cryoprecipitates Concentrates DDAVP (desmopressin acetate)
DIC - Treatment: underlying disease Medications ◦ Control bleeding ◦ fresh frozen plasma ◦ Heparin
Lymphangitis/Lymphedema Treatment Relieve edema, maintain skin integrity, prevent/treat infection Lymphangitis ◦ Moist heat, elevate, immobilize, skin/wound care, antibiotics Lymphedema ◦ Elevate, elastic stockings, skin care, bed rest, sodium restriction
Infectious Mononucleosis Treatment Recovery in 2 to 3 weeks Bed rest Analgesics
Anemia – Nursing Care Assessment Activity Intolerance ◦ ◦ Vital signs Rest periods Energy conservation Smoking cessation
Anemia – Nursing Care (continued) Impaired Oral Mucous Membranes ◦ ◦ ◦ ◦ Assess lips and tongue Mouthwash Frequent oral hygiene Avoid alcohol-based mouthwashes Petroleum jelly for lips Avoid spicy foods Encourage soft bland foods Small high-protein balanced meals each day
Anemia – Nursing Care (continued) Self-Care Deficit ◦ Assist with ADL ◦ Rest periods ◦ Concerns about self-care
Anemia – Nursing Care (continued) Evaluation ◦ ◦ Independent ADL Increased level of activity Skin and oral mucous membranes Diet
Polycythemia – Nursing Care Teaching ◦ ◦ ◦ Hydration Prevent blood stasis Elevate legs Support stockings Smoking cessation Report S/S thrombosis
Leukemia – Nursing Care Assessment ◦ Recognize manifestations
Leukemia – Nursing Care (continued) Risk for Infection ◦ ◦ ◦ Infection precautions Avoid invasive procedures Report evidence of infection Monitor vital signs Report lab values Explain precautions and restrictions
Leukemia – Nursing Care (continued) Imbalanced Nutrition: Less than Body Requirements ◦ Monitor weight ◦ Promote food and fluid intake ◦ Avoid procedures around meals
Leukemia – Nursing Care (continued) Impaired Oral Mucous Membranes ◦ ◦ ◦ Assess mouth 1: 1 solution saline/peroxide as mouthwash Soft-bristle toothbrush Medications for infection, pain Avoid alcohol-based mouth washes
Leukemia – Nursing Care (continued) Ineffective Protection ◦ ◦ ◦ Monitor LOC Report manifestations of bleeding Avoid invasive procedures Apply pressure to puncture sites Avoid straining with bowel movement
Leukemia – Nursing Care (continued) Anticipatory Grieving ◦ Therapeutic communication ◦ Manage stressful situations ◦ Support groups for the grieving process
Leukemia – Nursing Care (continued) Evaluation ◦ ◦ ◦ Freedom from infection Weight Food intake Oral mucous membranes Bleeding Coping
Malignant Lymphoma – Nursing Care Risk for Impaired Skin Integrity ◦ Measures to reduce itching Nausea ◦ Antiemetics ◦ Measures to relieve/reduce nausea
Malignant Lymphoma – Nursing Care (continued) Fatigue ◦ ◦ ◦ Assess malaise Encourage talking about disease Quiet activities Rest periods High-carbohydrate diet Fluids
Malignant Lymphoma – Nursing Care (continued) Disturbed Body Image ◦ ◦ ◦ Body image assessment Objective signs of altered body image Coping with alopecia Effects of illness on sexuality Support groups
Multiple Myeloma – Nursing Care Chronic Pain ◦ ◦ ◦ Assess pain Positioning, support with pillows Use of analgesics Nonpharmacology pain control Rest periods
Multiple Myeloma – Nursing Care (continued) Impaired Physical Mobility ◦ ◦ Reposition Change positions every 2 hours Trapeze Safety measures
Thrombocytopenia – Nursing Care Ineffective Protection ◦ ◦ ◦ Monitor LOC Manifestations of bleeding Avoid invasive procedures Pressure dressing to puncture sites Avoid straining at bowel movement
Hemophilia – Nursing Care Risk for Injury ◦ ◦ Signs of bleeding Stop bleeding with pressure, ice No IM injections Safety measures
Hemophilia – Nursing Care Risk for Ineffective Therapeutic Regimen Management ◦ Assess knowledge/reinforce teaching ◦ Emotional support ◦ Opportunities to learn/practice administration clotting factors
DIC – Nursing Care Ineffective Tissue Perfusion ◦ ◦ Assess pulses Turn every 2 hours No knee crossing Minimize tape use
DIC – Nursing Care (continued) Impaired Gas Exchange ◦ ◦ ◦ O 2 saturation levels ABGs Oxygen Fowler’s/semi-Fowler’s position Bed rest Deep breathing and coughing
DIC – Nursing Care (continued) Acute Pain ◦ Pain scale ◦ Handle gently ◦ Cool compresses to painful joints
DIC – Nursing Care (continued) Fear ◦ ◦ ◦ ◦ Verbalize concerns Answer questions Coping strategies Emotional support Calm environment Respond to calls for help Relaxation techniques
Lymphangitis/Lymphedema Nursing Care Implementation ◦ ◦ Measure effected extremity I&O Daily weights Sodium restriction
Lymphangitis/Lymphedema Nursing Care Implementation (continued) ◦ ◦ Antiembolic stockings/intermittent pressure devices Elevate extremities Skin care Protective devices