Osteoporosis The silent killer Michele T Glasgow MD


 • 200 million")






")




 • Anticonvulsants (Dilantin, Phenobarbital) •")



 • In the absence of a fracture,")





 Bone Mineral Density • Use total hip or femoral neck, whichever is")










 • FDA approved for prevention")
 • Administration: Nasal")
 • Administration: Oral, IV (Boniva and Reclast) • Side")
 • Actonel (Risedronate) • Boniva (Ibandronate) • Reclast (Zolendronic Acid)")

 • Class: SERM (selective estrogen receptor modulator) • MOA: anticatabolic (antiresorptive) •")
 • Class: anticatabolic (antiresorptive) • MOA: RANK ligand inhibitor • Administration: 60")
 • Class: Biologic agent • MOA: anabolic • Administration: 20 mcg injection")






- Slides: 55
Osteoporosis: The silent killer � Michele T. Glasgow, MD � Midwest Orthopaedic Institute � Bone Health Center � 2111 Midlands Court � Sycamore, Illinois
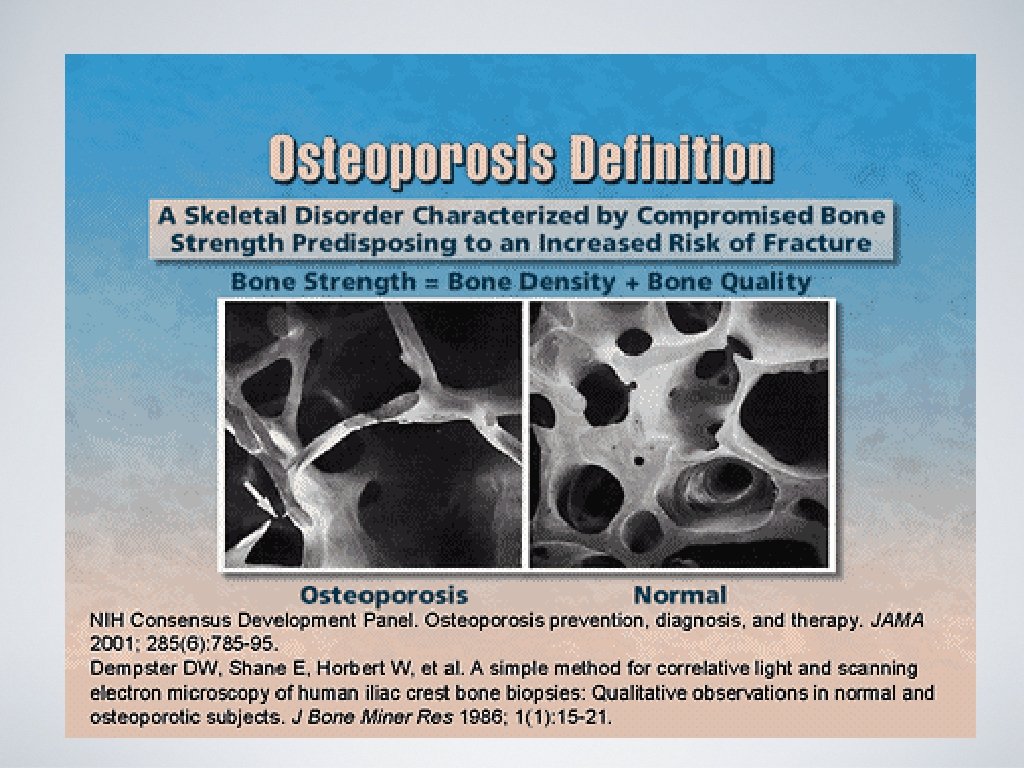
What is osteoporosis? • Means “porous bone. ” • Skeletal disorder characterized by compromised bone strength predisposing to an increased risk of fracture
Osteoporosis is Common • 9 million Americans have osteoporosis (~80% women) • 200 million people worldwide • 1 in 2 women and 1 in 4 men >50 yo will have an osteoporosis fracture in their lifetime • By 2020, it is projected that there will be ~14 million Americans with osteoporosis.
Osteoporosis is Costly • Responsible for 2 million fractures annually • $19 billion in related costs per year • By 2025, experts estimate osteoporosis will be responsible for ~3 million fractures and $25. 3 billion in costs each year
Osteoporosis is Serious • 20% of hip fractures die within one year REGARDLESS OF REPAIR from complications related to surgery or other co-morbidities • ~50% of hip fracture survivors require long term nursing home care and have some degree of permanent disability
Osteoporosis is “Silent” • Bone loss occurs without symptoms • Often it is not detected until a fracture occurs • Compression fractures of the spine often occur without trauma and may present with back pain, kyphosis, or simple height loss
Osteoporosis = TICKING TIME BOMB!!
Bone Composition • Bone Matrix • • Bone mineral • • 90% collagen and 10% other proteins Hydroxyapatite (calcium and phosphorus) Bone cells • Osteoclasts, osteoblasts, osteocytes
Bone Basics • Cancellous Bone Cortical Bone
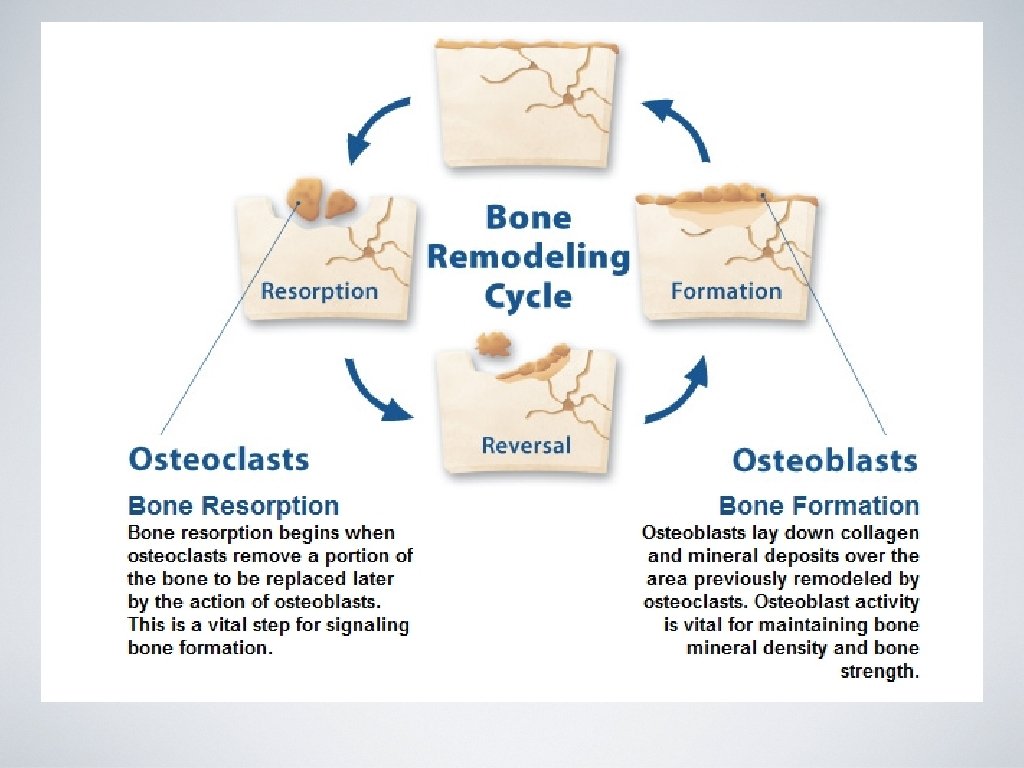
Bone science • Bone is constantly remodeling in a coordinated sequence of resorption (osteoclasts) and formation (osteoblasts). • Peak bone mass occurs between ages 18 -25. • Bone loss occurs when resorption > formation. • Age related bone loss occurs at a rate of ~0. 5 -1. 0% per year. • Bone loss accelerates with menopause (early and surgically induced) at an estimated rate of 1 -2% per year. • Women can lose up to 20% of bone mass in 5 -7 years after menopause.
Fracture Rates Displayed by Age and Gender
Who needs to be screened? ASK YOUR DOCTOR!!
Osteoporosis Risk Factors • Female • Thin, petite frame • Post menopausal • Age (>50 for women, >70 for men) • Race (Caucasian or Asian) • Family history • Hx of fracture or height loss • Poor calcium and vitamin D diet • Smoking • Excessive alcohol • Inactive lifestyle • Excessive caffeine intake
Diseases that cause bone loss Autoimmune Disorders - RA, MS, Lupus Digestive and GI Disorders - IBD, Celiac Disease, Wt loss surgery Endocrine/Hormonal Disorders –DM, Hyperparathyroidism, Hyperthyroid, Low estrogen or testosterone Hematologic/ Oncology - Cancer, Leukemia, Lymphoma, MM, Sickle Cell Disease Neurological Disorders - PD, Stroke, MS Mental Illness - Eating Disorders, Depression Other - AIDS/HIV, Kidney/Liver Disease, COPD
Medications that cause bone loss Medroxyprogesterone acetate (Depo provera) • Anticonvulsants (Dilantin, Phenobarbital) • Aromatase inhibitors (Arimidex, Aromasin, Femara) • Methotrexate • Chemotherapy/XRT • Cyclosporine/Tacrolimus • Gn. RH (Lupron, Zoladex) • Heparin • • PPIs (Nexium, Prevacid, Prilosec) • SSRIs (Lexapro, Prozac, Zoloft) • Steroids (glucocorticosteroids IE prednisone) Lithium • Tamoxifen (pre-menopausal use) Thyroid Hormones (In excess) • Thiazolidinediones (Actos, Avandia)
Fractures • Most typical osteoporosis sites: Hip, Spine and Wrist • Disease is systemic – occurs throughout the body • Fall from a standing height or low trauma resulting in a fracture IS by definition an osteoporotic fracture (aka fragility fracture)
Prevention • Balanced diet of calcium and vitamin D • Regular weight bearing and muscle strengthening exercise • Healthy lifestyle, avoid excess alcohol, caffeine, soda • Bone density testing and medication when appropriate • Fall prevention
Detection • DXA or bone density scan can: • Detect osteoporosis before a fracture occurs • Predict your chances of fracturing in the future • Determine your rate of bone loss and/or monitor the effects of treatment if the test is conducted at intervals of a year or more • Paid for by Medicare every two years
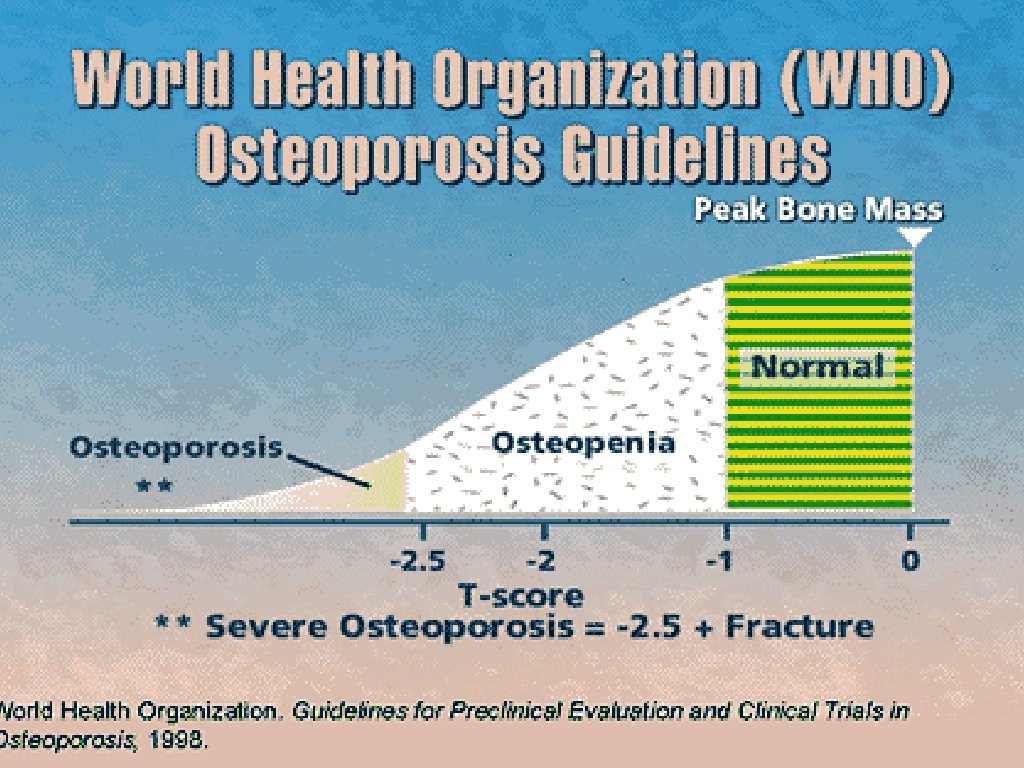
Diagnosis • Central dual-energy DXA (GOLD STANDARD) • In the absence of a fracture, T-score > -2. 5 in the spine, femoral neck or total hip. • Fracture of the hip or spine • AACE American Association of Clinical Endocrinologists) Guidelines for Diagnosis and Treatment of Osteoporosis 2010
Limitations of World Health Organization Definition • Established in post-menopausal osteoporosis • Does not recognize fragility fractures and therefore may have a “normal result” in patients with osteoporotic fractures • Only for central DXA and forearm • REMEMBER: This is a SCREENING TOOL!! It is in conjunction with clinical information and judgement
Alternative Tools: Peripheral DXA Should NOT be used for monitoring patient’s response to therapy Ease and availability Often used as a screening tool
Central DXA • Capable of measuring the spine and hip • “Gold Standard” • Used in most epidemiologic studies and clinical trials • Diagnosis is based on the lowest site
Contraindications for central DXA • Pregnancy • Recent contrast study or nuclear medicine scan (wait 72 hours) • Calcium supplements taken day of the study • Extensive orthopaedic instrumentation • Severe obesity
Lumbar Bone Mineral Density • Use L 1 -L 4 • Often falsely elevated due to osteoarthritis • May need to exclude arthritic segments, or, the entire study if necessary
Femoral (Hip) Bone Mineral Density • Use total hip or femoral neck, whichever is the lowest. • Do NOT use Ward’s area for diagnosis • Mean hip BMD can be used for monitoring (Total hip is preferred as ROI)
Medical Evaluation: Osteoporosis Labs • CBC • Intact PTH • CMP • Ionized calcium • TSH • SPEP/UPEP • Magnesium • Testosterone • Vitamin D 25 -OH • 24 hour creatine clearance • Bone turnover markers
Bone Turnover Markers • Product of bone remodeling • Noninvasive, easily repeated • NTX • Cannot be used to diagnose 733. 0 • CTX • Can be used to monitor response to treatment • Alkaline phosphatase • Expensive $$$$ • • Bone resorption markers Bone formation marker • Procollagen 1 -N terminal S
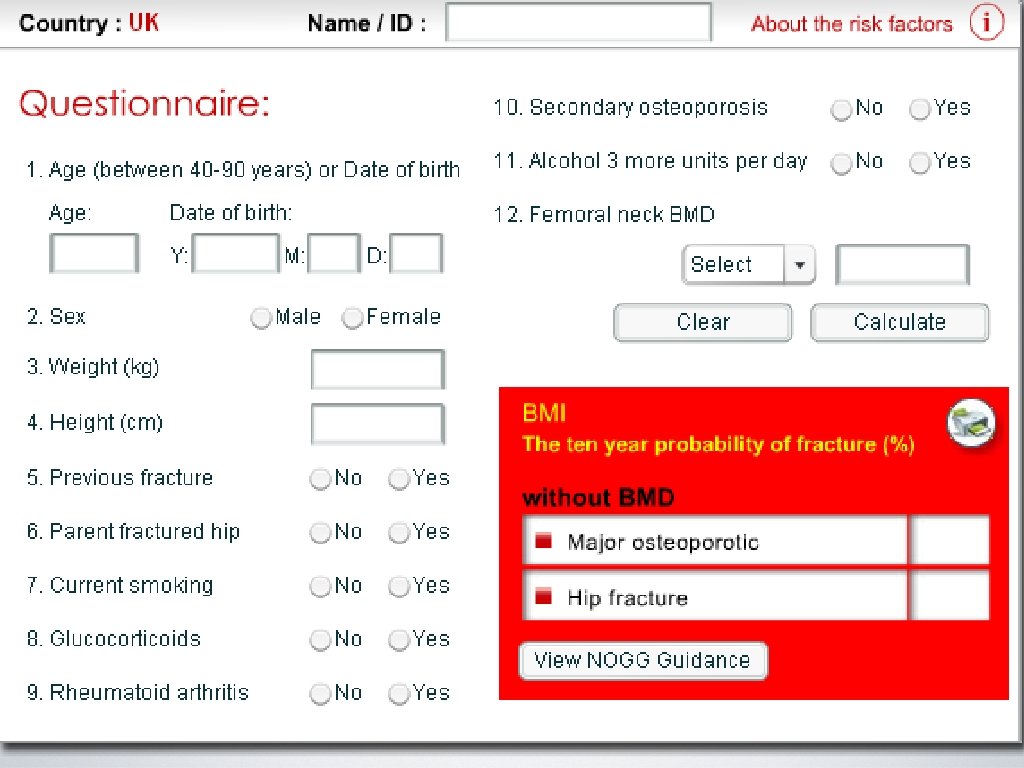
FRAX • Developed by WHO in 2008 • Prediction tool to assess an individual’s fracture risk • Risk factors + BMD (femoral neck only) = probability of osteoporosis fx in 10 yrs in untreated patients ages 4090. • Indication for treatment: Use clinical judgement!! • Low bone mass and a 10 year probability of a hip fx >3% or a 10 year probability of a major osteoporosis-related fx >20% (US-adapted WHO algorithm).
Osteoporosis Tools: DXA, labs, FRAX, clinical judgement
AACE Guidelines for treatment 2010 • Patients with a history of spine or hip fracture • Patients without a history of fractures but with a T-score of less than -2. 5 • Patients with a T-score between -1. 0 and -2. 5 if FRAX suggests a 10 year probability for major osteoporotic fracture is >20% or hip fracture > 3%.
“The skinny” on Calcium • Food is the best source! Read the label. • Food labels list calcium as a % of the DV (or 1000 mg) • i. e. 30% DV of calcium equals 300 mg • Supplement ONLY if needed. • Calcium is absorbed best when taken in amounts of 500 -600 mg or less. • Calcium carbonate is best absorbed with food • Calcium citrate is absorbed +/- food
The Sunshine Vitamin: Vitamin D • 3 Sources: Sunlight, Food, Supplements • Promotes calcium absorption • Maintains serum Ca and PO 4 (bone mineralization) • Needed for bone growth and remodeling
National Osteoporosis Foundation Calcium/Vit D recommendations • • • CALCIUM Women • • VITAMIN D Women and Men • <50 = 1000 mg • <50 = 400 -800 IU • >50 = 1200 mg • >50 = 800 -1000 IU Men • <70 = 1000 mg • >70 = 1200 mg
Supplements • Caltrate 600 + D: one tablet BID dosing w/ food • Citracal + D: 2 tablets BID dosing • Citracal Slow Release 1200: once daily • Citracal Petites
AACE 2010 Medication Recommendations • Use alendronate, risedronate, zoledronic acid or denosumab as first line therapy. • Use ibandronate as a second line agent. • Use raloxifene as a second or third line agent. • Use calcitonin as the last line of therapy. • Use teriparatide for patients with very high fracture risk or in patients who have failed bisphonate therapy. • Combination therapy is not advised.
Estrogen Replacement • Class: Hormone • MOA: anticatabolic (antiresorptive) • FDA approved for prevention of PMO • **NIH Recommendations 2002** • **Women should consult their doctor and weigh the benefits of HT against the risks for stroke, heart attack, blood clots, breast and colon cancer (WHI).
Calcitonin Nasal Spray • Class: Biologic agent • MOA: anticatabolic (antiresoprtive) • Administration: Nasal spray (Miacalcin) • FDA: Approved for women with 5+ yrs PMO • Side effects: Nasal irritation, possible analgesic effect, no known drug interactions. • Minimal increase spine BMD. No increase hip BMD.
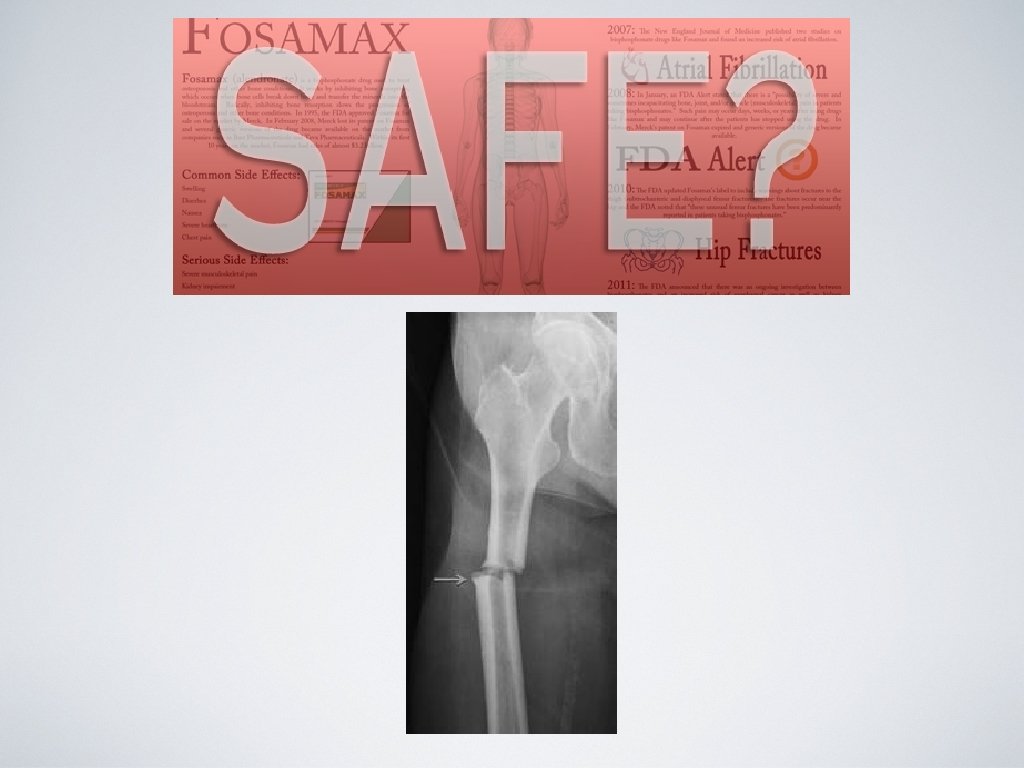
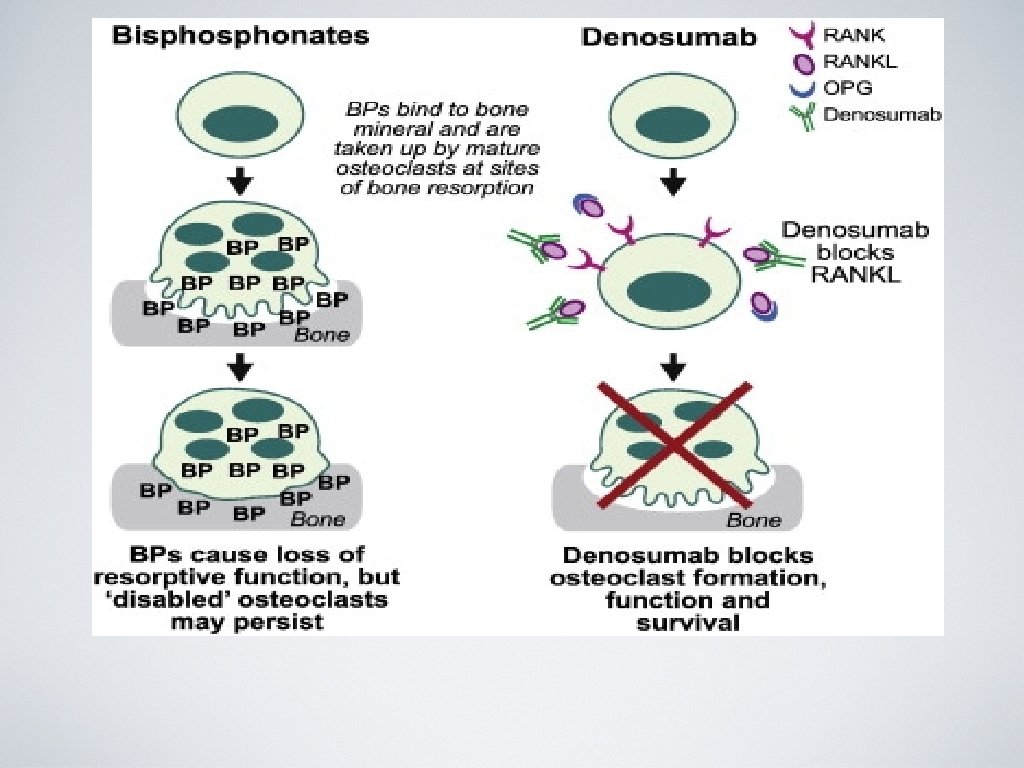
Bisphonates • MOA: anticatabolic (antiresorptive) • Administration: Oral, IV (Boniva and Reclast) • Side effects: • Avoid in renal patients (GFR <30 ml/min) • Osteonecrosis of the jaw (rare) • 15 min IV infusion may have an acute phase reaction (30 -40% have fever, myalgias)
Bisphonates • Fosamax (Alendronate) • Actonel (Risedronate) • Boniva (Ibandronate) • Reclast (Zolendronic Acid)
AACE Stance on Bisphonates 2010 • Consider a drug holiday after 4 -5 years of stability on bisphonate therapy. • Follow BMD and bone turnover markers during a drug holiday. • Reinitiate therapy if bone declines sustantially, bone turnover markers increase or fracture occurs.
Evista (Raloxifene) • Class: SERM (selective estrogen receptor modulator) • MOA: anticatabolic (antiresorptive) • FDA approved for prevention and tx of PMO • FDA approved as an agent to reduce breast cancer • Reduces spine fractures **hip and non vertebral fractures not proven** (2 nd or 3 rd line agent) • Side effects: Increased risk of DVT, does not alleviate hot flashes
PROLIA (denosumab) • Class: anticatabolic (antiresorptive) • MOA: RANK ligand inhibitor • Administration: 60 mg SQ every 6 months • FDA approved for prevention and tx of osteoporosis in PMO and osteoporosis tx in men. • Good option in pts who have failed or are intolerant to other available osteoporosis therapy • Side effects: hypocalcemia, infection, dermatologic rxn, ONJ
Forteo (teriparatide) • Class: Biologic agent • MOA: anabolic • Administration: 20 mcg injection SQ daily for max 2 years • FDA: approved for PMO women with osteoporosis at high risk of fracture and men with primary or hypogonadal osteoporosis at high risk of fracture • BLACK BOX WARNING: Osteosarcoma • DO NOT USE in pts with Paget’s, unexplained increase in alk phosphatase, kids, or prior skeletal XRT
Forteo Mechanism of Action
How is treatment monitored? • Baseline DXA with repeat DXA every 1 -2 years until findings are stable. Then repeat every 2 years. • Monitor changes in BMD of spine or total hip. • F/U patients should repeat DXA same facility, same machine. • Bone turnover markers
Defining successful treatment • BMD is stable or increasing and no fractures are present. • For patients on antiresorptive agents, bone turnover markers at or below the median value. • One fracture is NOT a sign of failure!! Consider alternate therapy, compliance, and reassess.
+Men >70
When to see the Bone Expert • Patient with normal BMD sustains a fracture without trauma. • Patients with recurrent fractures or continued bone loss despite therapy. • Severe osteoporosis. • When a patient has a condition that complicates management (ie. renal failure, hyperparathyroidism, malabsorption).
Thank you! Midwest Orthopaedic Institute Bone Health Center Michele T. Glasgow, MD Marie Rivers, PA-C