Osteoporosis Osteopenia 2016 06 27 Osteoporosis Osteoporosis is



, 남성(10%) § Osteopenia:")


")



 agent § § §")


- Slides: 22
Osteoporosis/ Osteopenia 2016. 06. 27. 학생집담회
Osteoporosis § Osteoporosis is defined as a skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Normal bone Osteoporosis NIH Consensus Development Panel on Osteoporosis JAMA 285: 785 -95; 2001
Bone Strength § NIH Consensus Statement 2000 Bone Strength Bone Quality and Bone Mineral Density a. BMD (areal) = g/cm 2 v. BMD (volumetric) = g/cm 3 Microarchitecture Geometry Turnover Rate Damage Accumulation Degree of Mineralization Properties of the Collagen/mineral Matrix Sourced from NIH Consensus Development Panel on Osteoporosis. JAMA 285: 785 -95; 2001
Epidemiology of Osteoporosis in Korea § 50세 이상에서, § Osteoporosis: 여성(30%), 남성(10%) § Osteopenia: 여성(80%), 남성(50%) § Osteoporotic fracture: 여성(30%), 남성(10%) • 여성: – hip fracture (10%) – spine fracture ( 21%) • 남성: – hip fracture (3%) – spine fracture (7%)
Excessive Mortality of osteoporotic fractures
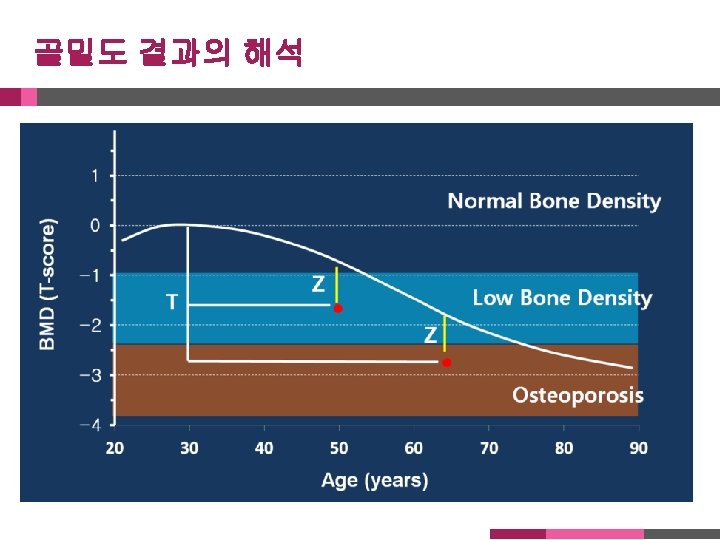
Diagnosis § Bone mineral density Dual Energy X-ray Absorptiometry
Medications associated with secondary osteoporosis 1. 당류코르티코이드 2. 헤파린 3. 항경련제 (carbamazepine, valproic acid) 4. 항우울제 (SSRIs) 5. 항암제 (methotrexate) 6. 면역억제제 (cyclosporin A) 7. Gonadotropin-releasing hormone agonists 8. Aromatase inhibitors 9. Glitazones 10. Proton pump inhibitors 11. Thyroxine 12. Loop diuretics
Clinical Risk factors for fractures § § § § Age BMD; 1 SD 2 fold increase of fracture risk BMI History of fragility fracture Family history of fragility fracture Cigarette smoking Glucocorticoids (>5 mg prednisolone daily or equivalent for 3 months or more) § Alcohol (≥ 3 units daily intake, dose-dependent increase in risk) § Rheumatoid arthritis
http: //www. shef. ac. uk/FRAX/tool. jsp? country=25
Pharmacologic therapy Who should be considered for treatment? § Postmenopausal women and men age 50 and older presenting with the following should be considered for treatment: § A hip or vertebral fracture (There is abundant data that patients with spine and hip fractures will have reduced fracture risk if treated with pharmacologic therapy) § T-score ≤ -2. 5 at the femoral neck, total hip or lumbar spine (There is abundant evidence that patients with osteoporosis by BMD have an elevated risk of fracture and reduced fracture risk with pharmacotherapy) § Low bone mass (T-score between -1. 0 and -2. 5 at the femoral neck or lumbar spine) and a 10 -year probability of a hip fracture ≥ 3% or a major osteoporosis-related fracture ≥ 20%)
Pharmacologic Intervention § Calcium & Vitamin D § Antiresorptive (anticatabolic) agent § § § Hormone therapy SERM (Raloxifene) Tibolon Calcitonin Bisphophonates (Alendronate, Risedronate, Ibandronate, Zoledronate) § Bone forming (Anabolic) agent § rh. PTH (Teriparatide)
Mechanism of Action 1. Osteoclast actively reabsorbs bone matrix 2. BISPHONATE ( bone mineral surface ) binds to 3. BISPHONATE is taken up by the osteoclast 4. Osteoclast is inactivated 5. Osteoclast becomes apoptotic (‘suicidal’) and dies Adapted from: Russell RG, Rogers MJ. Bone 1999; 25: 97– 106
Mechanism of Action