OSTEOPOROSIS Marium Sheikh BS Foods MSPH Nutrition Sr

OSTEOPOROSIS Marium Sheikh BS Foods, MSPH Nutrition Sr. Dietitian, THI

CASE STUDY • Kulsoom is a 68 -year-old lady, married, with two children who are living separately. She resides in a peripheral area in Karachi with her husband who does the grocery for cooking. • Kulsoom was working in a factory as a Shift Supervisor but had to stop work because of her difficulty in mobility. • She attends the outpatient bone health and osteoporosis clinic in a teaching, non-for-profit hospital and has been referred to you for dietetic assessment and advice.

ASSESSMENT DOMAIN - Anthropometry, Body Composition And Functional • • • Current weight - 42. 5 kg Weight 4 months ago - 49 kg Stadiometer height -1. 53 m Knee heel height - 1. 59 m Demispan (left arm) -1. 58 m • BMI – 16. 9 kg/m 2 using knee heel height – 18. 2 kg/m 2 using stadiometer height

ASSESSMENT. . • • Triceps skinfold thickness 11. 9 mm 5 th Percentile (Normal 23 -36 mm) Mid arm muscle circumference (left) 18. 1 cm 5 th Percentile (Normal 22. 528. 1 cm) • Bioelectrical impedance analysis • Fat percentage 19. 5% (Normal 24 -36%) – Fat free mass 34. 2 kg (Normal 42. 3 kg-49. 8 kg) – Fat mass 8. 3 kg (Normal 23 kg-36. 3 kg)
 – Non-dominant arm 13.")
ASSESSMENT. . • Grip strength dynamometry (Normal 17 -23 kg) – Non-dominant arm 13. 3 kg • Physical activity – almost nil • Using Hukka for 40 years

ASSESSMENT DOMAIN – Biochemical & Hematological Significant Lab Results • • Serum albumin 0. 42 mmol/L = 2. 79 g/dl (Normal: 3. 5 -5. 5 mg/dl) C-terminal telopeptide of type 1 collagen (CTX) 0. 6 µg/L (Normal: <0. 5 µg/L) Serum 25 (OH)D 23 nmol/L (Normal: 35 -150 nmol/L) TG 1. 1 mmol/L (Normal: <1. 7 mmol/L)

ASSESSMENT DXA results • • • Total body BMD T-score - 3. 2 AP spine BMD T-score - 4. 3 Left femur BMD T-score - 2. 8

ASSESSMENT DOMAIN – Clinical Past Medical History: • Hypertension, hypercholesteremia, asthma, depression, osteoporosis – spinal fracture T 10, T 12, L 3 Medications: • Rosuvastatin, metoprolol, was on Fosamax for 4 years, but no improvement on recent DXA so switched to daily injection – parathyroid hormone • Calcichew D 3 Forte BD (non-compliant) • Ventolin etc.

ASSESSMENT DOMAIN – Diet 24 Hr Recall BREAKFAST • Small bowl dalya (made with water and drop of low-fat milk (110 g)) • Two slices white bread toasted (2× 27 g) with butter (20 g) and jam (2 × 15 g) • Cup of tea (190 m. L) with teaspoon sugar (5 g) and drop of low-fat milk (15 m. L)
 with butter")
ASSESSMENT 24 Hr Recall LUNCH • ½ white flour paratha (27 g) with butter (10 g) • Commercial Katakat (40 g) Scrambled egg (60 g) with low-fat milk (15 m. L) • Cup of tea (190 m. L) with teaspoon sugar (5 g) and drop of low-fat milk (15 m. L)
 with tomato")
ASSESSMENT 24 Hr Recall DINNER • 1 slice white bread (27 g) with tomato (17 g) and 1 kebab (street food, 40 g) • Cup of tea (190 m. L) with 1 tsp sugar (5 g) and a drop of low-fat milk (15 m. L) • 2– 3 glasses water during the day Note: Appetite has reduced significantly as a result of pain and she has experienced some nausea (possibly due to new medication)

Analysis of Daily Intake • • Estimated energy intake 1040 kcal Protein intake 39 g Total fat intake 55. 6 g – 48% total energy Saturated fat intake 28. 4 g – 25% total energy Fiber 4. 1 g Calcium from food 418 mg Sodium 3227 mg
 kcal (including weight gain • Estimated")
Estimated Requirements • Estimated energy requirements 1693 factor) kcal (including weight gain • Estimated protein requirements 41. 81 - 52. 3 g protein/day
 Nutrition")
QUESTION # 1 1. What is the nutrition and dietetic diagnosis? (PES statement) Nutrition & Dietetic Diagnosis
 related to reduced appetite and pain (etiology)")
ANSWER # 1 Inadequate energy intake (problem) related to reduced appetite and pain (etiology) characterized by 6. 5 kg weight loss over a period of 4 months (signs and symptoms).

QUESTION # 2 2. What are the main nutritional concerns for this lady?

ANSWER # 2 Kulsoom’s weight loss and her low BMI would be the first concern. She has lost 6. 5 kg in months, which is 13. 7% of her initial body weight. 6 Anything >10% in the last months is considered severe (Blackburn et al. , 1977). She is not meeting her energy needs, there is a deficit of >500 kcal. 4

ANSWER # 2 Her protein intake is low. Evidence suggests that protein intake > than the RDI can improve muscle mass, strength and function in the elderly and that it may improve bone health (Dawson-Hughes, 2003).

ANSWER # 2 Results are conflicting, with some studies suggesting a beneficial effect of protein on bone (Delmi et al. , 1990; Rizzoli et al. , 2001), and others showing a positive correlation between protein intake and bone loss (Huang et al. , 1996; Johnell et al. , 1995; Munger et al. , 1999). In some cases it appears that an intake of 1. 5 g protein per kg body weight per day may be required in elderly individuals to be beneficial for health and function (Wolfe et al. , 2008).

ANSWER # 2 • Kulsoom is not compliant with her calcium and vitamin D supplements and her dietary intake of calcium is low. Kulsoom’s serum 25 (OH)D is very low at 23 nmol/L.
 Saturated")
ANSWER # 2 Kulsoom’s fat intake is very high (48% total energy intake) Saturated fat intake is 25% of total energy intake
")
DO YOU KNOW? Sodium Content of Some Foods Chicken Yakhni Cube (4. 8 g) = 1152 mg Cheese 1 slice = 180 mg Soya Sauce 1 tbsp = ~1000 mg Salted Butter 1 tbsp = 91 mg Pudding (Dry Mix) 1 cup prepared = 720 mg Bottled Olives (6) = 680. 4 mg

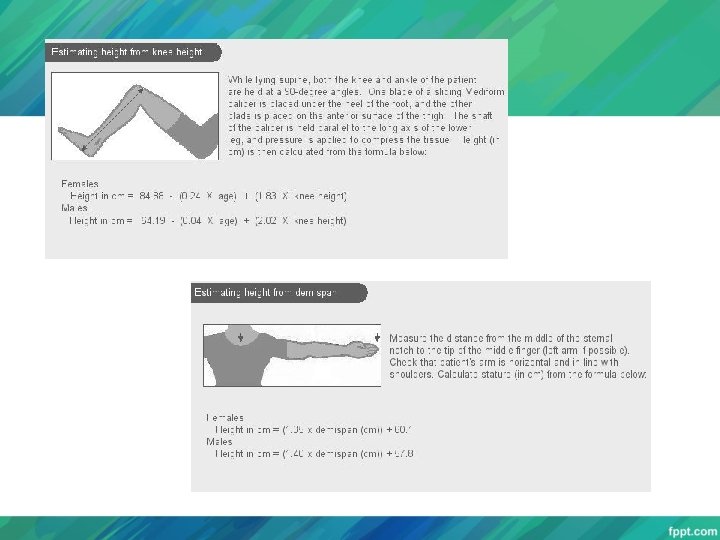
QUESTION # 3 3. Comment on the different methods used in this case to measure height to calculate BMI.
 = 16. 9 kg/m 2 Underweight BMI")
ANSWER # 3 BMI (knee heel height) = 16. 9 kg/m 2 Underweight BMI (stadiometer height) = 18. 2 kg/m 2 Significantly Higher Stadiometer height may NOT be the most accurate method (loss of height vertebral fractures) Patients recalled height must also be taken into consideration Other methods: knee to heel height, demi span, or ulna length

ANSWER # 3 The current literature does not allow a BMI cut-off value for osteoporosis risk. BMI<22– 24 kg/m 2 is associated with less bone density compared with a BMI>26– 28 kg/m 2. Increased body weight has NO advantage to skeletal health when this increase becomes excessive (BMI>30 kg/m 2) as this can → immobility, osteoarthritis and an increased risk of fall (Wardlaw, 1996).

QUESTION # 4 4. What are the aims and objectives of Kulsoom’s nutritional care plan?

ANSWER # 4 Energy and protein intake to promote weight gain by: ↑ portions of carbohydrate at lunch and dinner ↑ snacks between meals ↑ portion size of lean protein and choose healthy fats • Increase low-fat dairy products (yogurt, milky drinks, rice pudding etc. ) • Encourage to take calcium and vitamin D supplements

ANSWER # 4 • Encourage food sources of vitamin D, for example, oily fish, fortified milk. • Reduce saturated fat and salt content and encourage to eat unprocessed food with high fiber and vitamin and mineral content.

QUESTION # 5 5. What outcomes could you assess in order to monitor the success of your intervention?
D and urinary Ca")
ANSWER # 5 WEIGHT Serum 25 (OH)D and urinary Ca

QUESTION # 6 6. Comment on the bioelectrical impedance analysis and hand grip results for this lady?

ANSWER # 6 • Fat mass and FFM are both below 10 th percentile for healthy women of her age (Kyle et al. , 2001) indicating that loss of muscle mass is possibly a result of PEM • At risk of falls and possible fractures • The probability of PEM is confirmed by the results of the handgrip strength test. Her result of 13. 3 kg is significantly below 23 kg which is 85% of normal, which is indicative of PEM

QUESTION # 7 8. Discuss Kulsoom’s DXA results.
 and diminished BMD")
ANSWER # 7 • Significantly diminished total bone mineral density (BMD) and diminished BMD in the spine and femur. • This is diagnostic of osteoporosis; she is therefore at risk of fractures associated with osteoporosis.

QUESTION # 8 8. What other nutrients are important in patients with osteoporosis?

ANSWER # 8 • Besides protein, energy, calcium and vitamin D, phosphorus, magnesium, zinc and vitamins K and C are also important in osteoporosis.

QUESTION # 9 9. Would you advise her to see any other allied healthcare professionals? If so, who?

ANSWER # 9

QUESTION # 10 11. Describe the nutritional management when undergoing surgery for a broken head of femur.

ANSWER # 10 • The metabolic stress, and therefore increase in requirements, of such surgery is often underestimated. • A stress factor of 20% should be added to BMR to account for the increase in energy requirements. • A high protein, high energy diet, provided in small, frequent portions, should be prescribed.

- Slides: 42