Temporomandibular joint disorders DEFINTION of TMJ The temporomandibular

Temporomandibular joint disorders

DEFINTION of TMJ The temporomandibular joint is a synovial joint that connects the mandible—to the temporal bone. Because these joints are flexible, the jaw can move smoothly up and down and side to side, enabling us to talk, chew and yawn. Muscles attached to and surrounding the jaw joint control its position and movement.
 is a term § used to describe a group")
TMJ DISORDERS Tempromandibular disorders (TMD) is a term § used to describe a group of problems involving the TMJs , muscles, tendons, ligaments, blood vessles, and other tissues associated with them. It is the most common cause of facial pain after § toothache. The AAOP classification divides TMD broadly into 2 syndromes: (1) muscle-related TMD (myogenous. TMD), sometimes this is called TMD 2 ry to myofacial § pain and dysfunction (MPD) §. (2) joint-related (arthrogenous)TMD §

EVALUATION -History -Examination A. Extraorally 1. Symmetry 2. Deviation 3. Muscular hypertrophy 4. Masticatory muscles palpation 5. TMJ examination Tenderness Sounds Range of movement (ii 45 mm, LE 10 mm)

B-INTRA ORALLY Odontogenic source of pain § Wear facets § Mobility § Soreness § Dental & skeletal classification (Occlusion) §

INTRAAURICULER EXAM.

PREAURICULER EXAM.

MASSETER EXAM.

TEMPORALIS EXAM.
 § 2. tomograms § 3. transcranial § 4.")
Radiographic evaluation 1. panoramic radiography (DPT) § 2. tomograms § 3. transcranial § 4. TMJ arthrography § 5. MRI § 6. nuclear imaging § Psychological evaluation §

TRANSCRANIAL

MRI

TOMOGRAM CLOSED & OPEN
")
Classification of TMJ Disorders Developmental § Limitation of movement § Myofascial pain dyfunction (MPD) § Internal derangement § Degenerative Joint Diseases (DJD) § Systemic arthritis conditions § Effusion TMJ dislocation (open lock) § Neoplasia §
")
Developmental A-Condylar hypoplasia or aplasia § - unilateral § - bilateral (treacher Collins' syndrome) §

B-Condylar hyperplasia § - uncommon § - usually unilateral § - Asymmetry, deviation to the opposite side § - crossbite § - not painful § TTT: § - if diagnosed in active phase Intracapsular § condylectomy. - if growth ceased corrective osteotomy. § C- Hemifacial microstomia : (Pierre Robin's § Syndrome)

Condylar hyperplasia
 Causes: Inflammation in or near the joint §")
Limitation of movement Temporal limitation (trismus) Causes: Inflammation in or near the joint § Pericoronitis § Cellulitis § Abscess (submassetric) § osteomyelitis § Mandibular block injection …. . irritation , § infection or hematoma. Injuries § Tetanus and tetany § TMPDS §
 A-Intracapsular Ankylosis: - fusion of condyle, disk § and fossa compex")
Permanent limitation (Ankylosis) A-Intracapsular Ankylosis: - fusion of condyle, disk § and fossa compex as a result of fibrous tissue, bone or both. 1 -Fibrous Ankylosis (Adhesion): - § occures in superior joint cavity between disk and § eminence, it may occur in inferior space. D. D: anterior disk displacement without reduction § R/F: MRI shows fibrosis in disk space § C/F § - no pain § - deviation on opening § - limited mouth opening § - no joint sound §
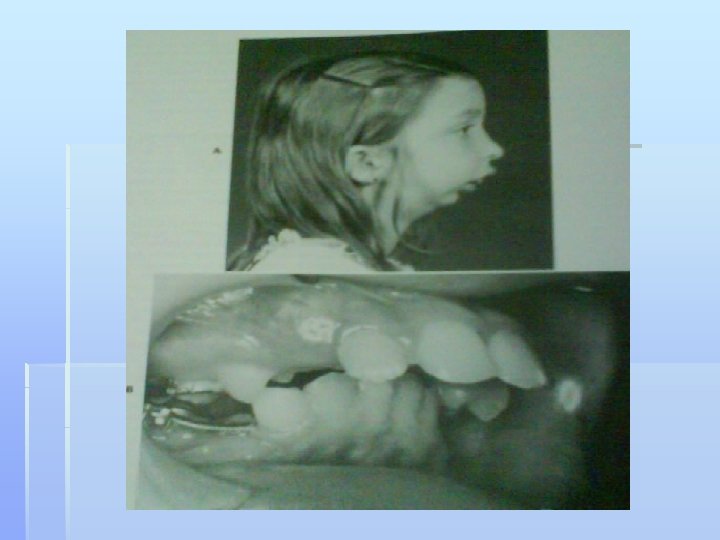
 Bony Ankylosis union of bones of TMJ -complete immobility § C/F § no")
2) Bony Ankylosis union of bones of TMJ -complete immobility § C/F § no pain § marked deviation to affected sides § marked limitation of mouth opening § no joint sounds § could be uni or bilateral (severe retrognathia ) § R/F: § bone proliferation §

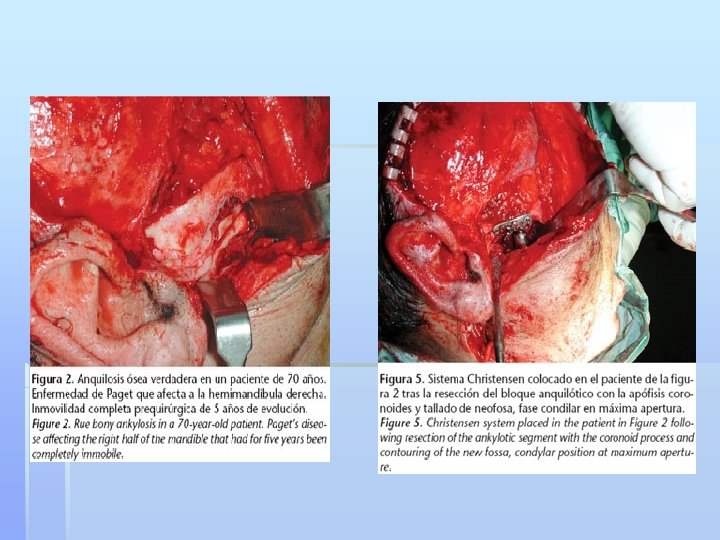
Etiology: Trauma: - § - intracapsular Communated # of condyle disorganization bone formation - penetrating wounds § - forceps delivery § Infection: § - otitis media § - osteomyelitis § - pyogenic arthritis § Juvenile arthritis § Neoplasm --- chondroma § Paget’s disease § bleeding §

Treatment: Mobilizing the existing joint, may need to § section the coronoid process and reshaping of condylar head. False joint lower down in the mandible § (condyler neck or ascending ramus) Total joint replacement by alloplastic or § autogenous implant (costochondral) Active physiotherapy following surgery §

B. Extracapsular Ankylosis - coronoid process hyperplasia § - trauma to zygomatic arch § - infection around temporalis muscle § - oral submucous fibrosis § - systemic sclerosis § - fibrosis due to burn or irradiation §

Myofascial pain dysfunction syndrome The most common cause of masticatory § pain & limited function. The source of pain is muscular. § Causes § Bruxism secondary to stress& anxiety § Occlusion, modifying or aggravating factor § May also be secondary to ID or DJD §
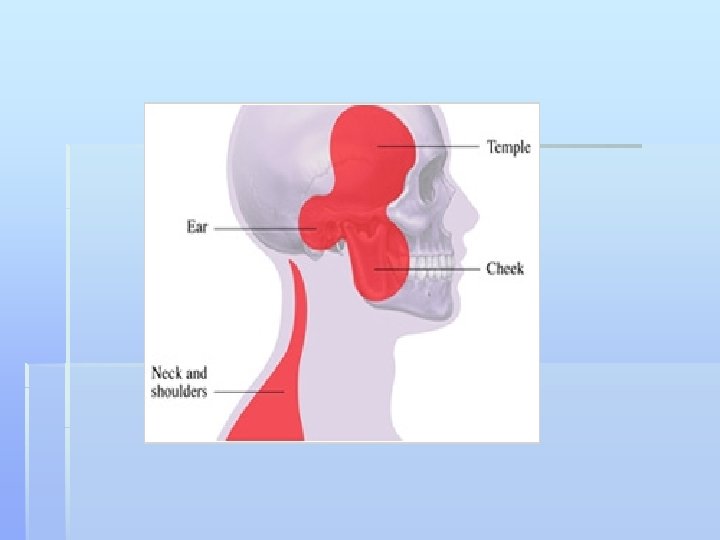
 § 2 nd - 3 rd decades §")
C/F: Females > males (4: 1) § 2 nd - 3 rd decades § Periauricular pain § - Diffuse, poorly localized § - Radiates to angle of mandible, or temporal regions § sifies at morning & peroids of tension & § anxiety Muscle tenderness § Absence of tenderness in the joint § Limited movement and deviation to affected side § Joint noise usually not present § Headache § Teeth may have wear facets §

R/F: normal unless there is ID or DJD § Management: § Reassuranse § Conservative treatment § Analgesics (NSAIDs) § Muscle relaxants § Physiotherapy § Correction of occlusal disharmony § splints § Psychological counselling §

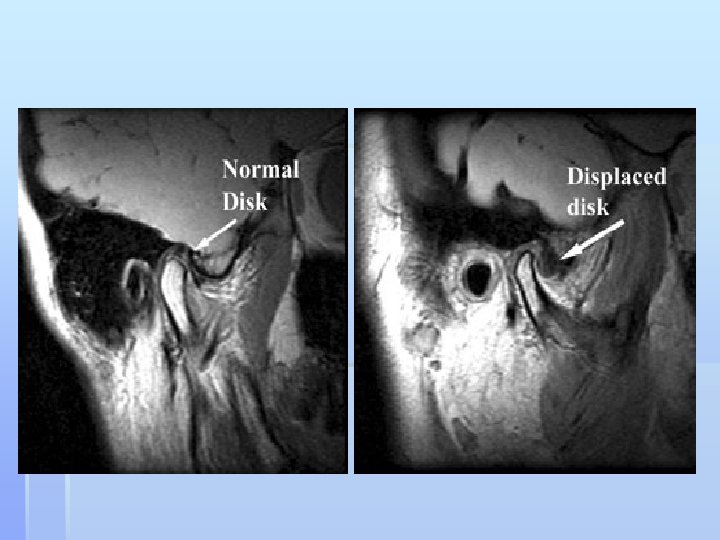
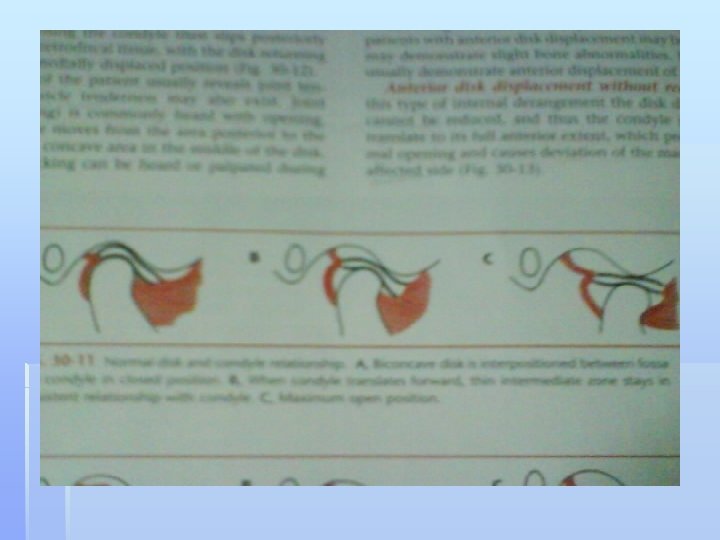
Internal derangement Definition: altered relationship of articular disc § to condyle , fossa and articular eminence § Anterior disc displacement with § reduction : Joint closed: disc ant. and medial to condyle § Joint open: disc return to normal condyle disc § relation---opening click
 Transient jaw deviation to side")
C/F: Clicking on opening and closing § (reciprocal click) Transient jaw deviation to side of clicks § then straightening forward. Joint tenderness may be present § Maximum opening is normal § R/F: § - Plain x-ray may be normal § - MRI shows Ant. displacement of disk §

Management § Reassurance and explanation § Occlusal splints, ant. repositioning splint § Physiotherapy § NSAIDS §
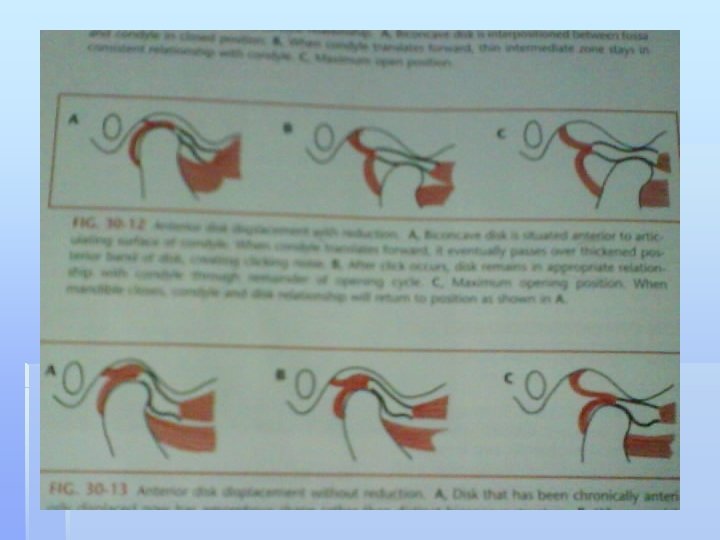

Anterior disc displacement without reduction Disc cannot be reduced to its normal position § Cause: continuous disc deformation with § elongation of disc ligament C/F: § limited mouth opening 20 -25 mm § limited lateral excursion to contralateral side § deviation on opening to affected side § may be painful § no click §

R/F: § plain x-ray may be normal or there is § signs of osteoarthrosis § MRI…abnormal disc position § Management § reassurance, explanation § muscle relaxant and physiotherapy § analgesics § manipulation under anesthetic +splint § Surgery: § arthrocentesis § menisectory and disc replacement § disc plication §

How to differentiate b/w ant. Disc displacement without reduction & MFP Sudden onset § History of click § Not possible to extend opening by finger pressure § Diagnostic anesthesia § MRI, arthrography §
 (Osteoarthrosis, osteoarthritis) Definition: - variety of anatomic findings § including")
Degenerative Joint Diseases (DJD) (Osteoarthrosis, osteoarthritis) Definition: - variety of anatomic findings § including irregular , perforated or severely damaged discs in association with articular surface abnormalities i. e. . Flattening, erosion, lipping…….

Mechanism: Direct mechanical trauma: excessive § mechanical loading ----free radicals----intracellular damage. Hypoxia perfusion theory: excessive § intracapsular hydrostatic pressure within the TMJ may exceed the blood level---hypoxia Neurogenic inflammation: - stretching of § nerve-rich retrodiscal tissue----cytokines Osteoarthritis differ from osteoarthrosis in § 2 ry inflammation

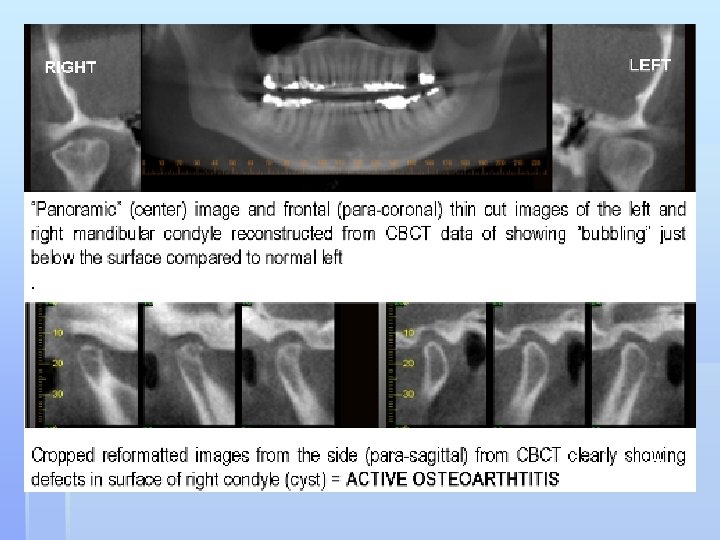
C/F: § elderly most affected § pain § crepitus § tender joint § limitation of mouth opening § Course of the disease § Painful inflammatory, erosive phase, lasts for § 3 yrs. Phase of resolution---- smooth out again § R/F § Bony changes: erosive, lipping, anvil shape § deformity , Ely’s cyst , irregularity in condylar head.
 Left")
ght (lipping) Left
--- § micrognathia")
Systemic Arthritis conditions RA § Ankylosing spondilitis § Juvenile arthritis (still's disease)--- § micrognathia and Ankylosis Reiter's syndrome (uveitis, urethritis and § oral ulcers) gout § Lyme disease §

Rheumatoid arthritis Clinical findings § Women 25 -40 § crepitus § Symmetrical ant, open bite § Pain, weakness, swelling may present § TMJ symptoms usually minor § Morning joint stiffness, limitations of opening § Serology: abnormal finding, RF+ve §

R/F: § may show changes , erosion, § osteophytes, traction spure, irregularity in condylar head. Management: - § Analgesics /anti-inflammatory drug § Steroids § Physiotherapy § Taking load off the joint awaiting natural § resolution Surgery §

Effusion Influx of fluid into the joint, usually either bleeding § following trauma or inflammatory exudates. C/F: § pain over joint § swelling over joint § limitation of movement § sensation of blocked ear § difficulty in occluding posterior teeth § R/F: widened joint space § Management: § Anti-inflammatory drugs § Rarely surgical drainage §
 Displacement of one component of the joint § beyond its")
TMJ dislocation (open lock) Displacement of one component of the joint § beyond its normal limits without spontaneous return to its normal position Subluxation: can be reduced by the pt § History § Maximum mouth opening § Trauma § Previous dislocation § Duration §

C/F Usually painful , if acute: sever pain § Inability to close the joint § Muscle spasm § Could be: § - unilateral-----deviation § - bilateral------prognathia § Eating and talking very difficult § Associated Subcondylar #. . . pain § Iatrogenic # from reduction of dislocation §
 Immediate cause: exaggerated opening § (yawning, singing), dental procedures under LA")
Causes § 1) Immediate cause: exaggerated opening § (yawning, singing), dental procedures under LA or GA, blow or partially opened mouth. 2) Trauma: condyle can be dislocated to middle § cranial fossa. 3) Congenitally shallow mandibular fossa or § underdeveloped condyle. 4) Rare: - Marfan's syndrome, Ehler-Danlos' § Syndrome, Malignancies, osteomyelitis , RA § 5) Drugs: - metoclopromide, phonithiazines § 6) psychotic: - dyskinesia §

Classification § acute dislocation § chronic recurrent dislocation § unilateral § Bilateral § subluxation § R/F: condyle will be anterior and superior to the articular eminence.

Emergence department care § conscious sedation, LA in TMJ or GA. § Reduction by exerting an inferior and posterior § pressure while holding the mandible firmly in the molar region. Redislocation is common within first 24 hours. § Complications of dislocation § # condyle § Infection : osteomyelitis § Massive edema § Injury to external carotid artery and facial nerve § Interposition of soft tissue § Complication of reduction § Iatrogenic condyle # § Human bite §

Surgery for recurrent dislocation Operation limits the condyle path: § Placing a block (bone, cartilage, alloplast i. e. L-shaped § stainless steel pins) on the articular eminence in front of the condyle. Dautrey's procedure (# zygomatic arch) § Tightening the capsule § Injection of sclerosing solution § Section of lateral pterygiod or temporalis (Myotomy) § Disc plication § operations free the condylar path § High condylar shaving § Eminectomy § Menisectomy §

A-Dautrey procedure B-CONDYLAR SHAVING

Neoplasia of the TMJ Usually rare § Occurs from any structural component of the TMJ § (condylar head, articular fossae, disc, capsule, etc …. Benign neoplasms of the TMJ § Osteochondroma § Osteotoma § Chondroma § Fibromyxoma § Giant cell lesions § Chondromatosis § Malignant neoplasms of the TMJ § Chondrosarcoma § Primary intrinsic malignant neoplasms § Synovial sarcoma § Fibrosarcoma § Metastatic lesions §

Aims of ttt Improving jaw function § Reducing pain & discomfort § Decreasing inflammation in muscles & joints § ? esthetic § Reversible ttt § Patient education § Medications § Physical therapy § splints §

Patient education Soft diet with gradual progression to normal diet over 6 -8 weeks, Avoiding large bites and clenching of teeth, § Keeping jaw relaxed, § Yawning against pressure, § Massage of jaw and temple muscles, § Use of moist heat, § Avoiding cradling the phone between ear and § shoulder, Good sleep posture with adequate neck support Passive or active range of motion exercises § § §
 § Analgesics § Acetaminophen §")
MEDICATIONS NSAIDS § Ibuprofen § Naproxen § Celcoxib (Celebrex) § Analgesics § Acetaminophen § Narcotics (morphine) § Muscle relaxent § Cyclobenzaprine, methocarbamol § TCA: Amitriptyline § Injection to muscles § Botuline toxin (BOTOX) § Steroids… can lead to further degeneration §

DRUGS doses & prescription Ibuprofen NSAID 200 -400 mg PO q 4 -6 h as long as symptoms persist; not to exceed 3. 2 g/d Naproxen NSAID 500 mg PO, followed by 250 mg q 6 -8 h; not to exceed 1. 25 g/d Celcoxib COX-2 inhibitor 100 mg twice daily Methocarbamol Muscle relaxant 1. 5 g PO qid for 2 -3 d, then increase to 44. 5 g/d in 3 -6 divided doses Cyclobenzaprine Muscle relaxant 20 -40 mg/d PO divided bid/qid; not to exceed 60 mg/d Morphine Narcotic 0. 1 mg/kg IV/IM/SC Amitiptyline TCA 25 -75 mg/day in divided doses Diazepam Anxiolytic , Muscle relaxant Mild spasms: 5 -10 mg PO q 4 -6 h prn Moderate spasms: 5 -10 mg IV prn Severe spasms: Mix 50 -100 mg in 500 cc

PHSIOTHERAPY Jaw exercising device § Relaxation training, EMG monitoring § Ultrasound § Spray & stretch § Friction massage § TENS § SPLINTS § Autorepositioning splint § Anterior repositioning splint §

physiotherapy exercise device § Spray & stretch § TENS §

Surgery of the TMJ Most disorders of masticatory apparatus do not § require surgical ttt. Surgery can range from closed manipulation to § major reconstruction of the joint. In some cases such as severe ankylosis or § severe degeneration surgery is initial phase of therapy.

Minimally invasive tech. § 1 -Injection into the joint: LA or steroids: 2 mm § -2 -Closed manipulation for adhesions § LA post. to the joint § NSAIDS b/f & a/f § Irrigation of the joint with saline & steroids § 3 -Arthroscopy: diagnostic & therapeutic…. sup. joint space § Indications § ID , DJD , Adhesions § 4 -Arthrocentesis § Flush out chemical mediators § Can release adhesions § Stretch of constricted capsule §

ARTHROCENTESIS

Surgical approach to the TMJ 1. Preauricular incision § 2. Temporal extension § 3. Question mark extension § 4. Submandibular incision § 5. Endaural approach §
 Indication: ID , recurrent dislocation § Soft diet")
Disc repositioning surgery (DISC § PLICATION) Indication: ID , recurrent dislocation § Soft diet 3 -6 months § Jaw exercise a/f 6 -8 weeks §

Disc repair or removal Ind : severely damaged or perforated discs § Menisectomy § Disc repair …. skin graft § Replacement of disc § 1 -Alloplastic …silastic § 2 -Autogenous. . . temporalis fascia § Auricular cartilage § Dermis §

Total joint replacement Ind : § severe DJD § Severe Ankylosis § Neoplasia § Multiple failed surgery § Types § Autogenous implant… costochondral bone graft § Stereolithic models & custom fabrication §

Costochondral alloplast

Complications of TMJ surgery Bleeding, wound infection, scars § Injury of adjacent structures: VII § branches, middle meningeal artery Occlusal disturbances § Frey's syndrome § §

Post surgical management Early mobilization to prevent scar § formation Feeding: soft or liquid diet § Regular exercise § Time scale for recovery: best level of jaw § movement about 2 months Follow up §

Problems Pt attend with 10 yrs history of painless click, ii opening is § 55 mm. A click was felt at early opening & late closing. diagnosis? Does she need surgery? Pt c/o pain in periauriculer area on both sides, limitation of § mouth opening for several months. ii opening is 29 but can be increased to 37 with pain. diagnosis? need surgery? Pt c/o pain in periauriculer area on both sides, limitation of § mouth opening for 4 weeks, have a history of click. ii opening is 23 mm, cannot be increased by pressure. opening not limited by pain. diagnosis? Does he need surgery? Pt c/o joint sounds, tender joint & sever limitation of joint § pain. What is most likely diagnosis?

- Slides: 75