Temporomandibular Disorders Course Textbook Manual of Temporomandibular Disorders

Temporomandibular Disorders Course Textbook: Manual of Temporomandibular Disorders by Edward F. Wright Copyright 2005 Blackwell Munksgaard

Overview • Introduction • Part I Initial Evaluation • Part II Common Acute TMD Conditions and Treatments • Part III Occlusal Appliance Therapy • Part IV Multidisciplinary Treatment Approach • Part V Case Scenarios
 • Encompass medical and dental conditions affecting the temporomandibular joint (TMJ),")
Temporomandibular Disorders (TMD) • Encompass medical and dental conditions affecting the temporomandibular joint (TMJ), masticatory muscles, and adjoining structures • These conditions are linked by their common signs and symptoms

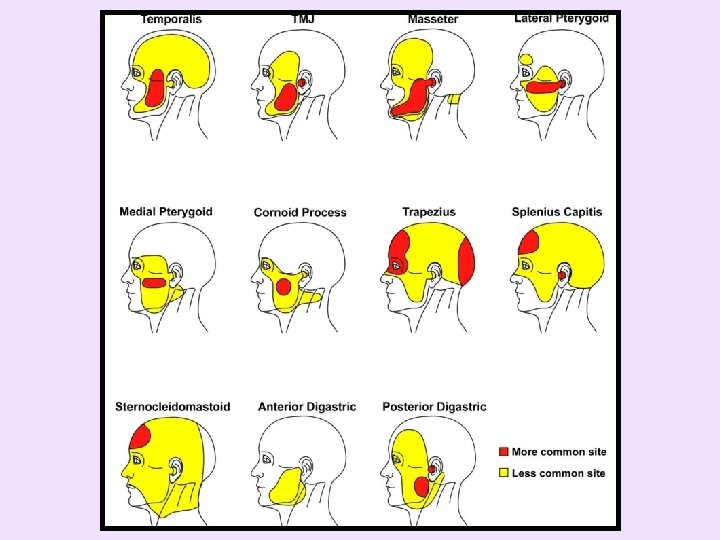
Cardinal TMD Signs and Symptoms • Masseter muscle pain • TMJ pain • Temporalis muscle pain • Mouth-opening limitations • TMJ sounds Pain is by far the most common reason patients seek treatment

TMD is Extremely Common • Most often reported between ages of 20 and 40 • Approximately 33% of population has at least one TMD symptom • 3. 6 to 7% of population has TMD with sufficient severity to seek treatment

TMD Symptoms Generally • Fluctuate over time • Correlate with – Parafunctional habits • Masticatory muscle tension • Tooth clenching and/or grinding • Other oral parafunctional habits

– Psychosocial factors • Worry • Stress • Irritation • Frustration • Depression – TMD patients with poor psychosocial adaptation have significantly greater symptom improvement when the dentist’s therapy is combined with cognitive behavioral intervention

TMD Can Also Cause • Non-otologic otalgia • Dizziness • Tinnitus • Neck pain • Toothache

TMD Can Contribute to • Migraine and tension headaches • Muscle pain in region • Many other pain complaints

TMD Greater Problem for Females • Request treatment more often • Symptoms less likely to resolve – Female: male patient ratio between 3: 1 and 9: 1 • Many hypotheses for gender disparity – Underlying reason remains unclear

TMD is a Multifactorial Disorder • Many therapies may benefit a TMD patient’s symptoms • May benefit from – Treating the muscles and/or cervical region • • Physicians Physical therapists Chiropractors Massage therapists

– Providing relaxation, stress management, cognitive-behavioral therapy, and other psychological aspects • Psychologists • Psychiatrist – Improving occlusal stability • Orthodontists • Prosthodontists • General dentists – Similar efficacy from different appliance forms

– Decreasing TMJ inflammatory mediators • Oral surgeons • Anti-inflammatory medications – Medications • Generally provide only temporary improvement – Self-management strategies • As used for other muscles and joints in the body

From Patient Interview and Clinical Exam • Determine most cost-effective therapies with greatest potential for long-term symptom relief – Often reduce the patient’s contributing factors – Often facilitates the patient’s natural healing capacity – Are similar concepts to orthopedic and rheumatologic disorder management • No one treatment has been shown to be best for all TMD patients

Generally Recommend TMD Therapy if Patient has Significant • • Temporal headaches Preauricular pain Jaw pain TMJ catching or locking Loud TMJ noises Restricted opening Difficulty eating, due to TMD Non-otologic otalgia, due to TMD

Part I Initial Evaluation Chapter 1 Patient Interview Chapter 2 Review of “Initial Patient Questionnaire” Chapter 3 Clinical Examination Chapter 4 Imaging Chapter 5 TMD Diagnostic Categories Chapter 6 Contributing Factors

Part I Initial Evaluation • Goals are to identify the patient’s – Primary diagnosis – Secondary, tertiary, etc. , diagnoses – Contributing factors – Symptom patterns

Primary Diagnosis • Diagnosis for disorder most responsible for patient’s chief complaint – Can be of TMD origin – Can be from non-TMD source, e. g. , • Pulpal pathosis • Sinusitis • Cervicogenic headache

Secondary, Tertiary, etc. , Diagnoses • Other TMD diagnoses that generally contribute to patients’ TMD symptoms • When non-TMD disorders (e. g. , fibromyalgia) contribute to patient’s primary TMD diagnosis symptoms, are designated as contributing factors and not as secondary or tertiary diagnosis
,")
Perpetuating Contributing Factors • Elements that perpetuate the disorder (not allowing it to resolve), e. g. , – Nighttime parafunctional habits – Gum chewing – Daytime clenching – Stress – Neck pain

Symptom Patterns • Period of the day in which the symptoms occur or are most intense, e. g. , – Worse upon awaking • Location pattern, e. g. , – Begins in neck and then moves to jaw

Non-TMD Example: Wrist Pain • Palpation identified – Wrist joint most tender and most reproduced the pain (diagnosis is primary diagnosis) – Muscles in area less tender and reproduced the pain to lesser degree (diagnosis is secondary diagnosis)

• If symptom pattern – Pain begins ½ hour after starts using computer and continues as long as uses computer • Contributing factor – Use of computer • Treatment – Refer to therapist to teach computer keyboard and mouse ergonomics – Prescribe NSAID short-term

• If symptom pattern – Pain only occurs upon awakening and lasts ½ hour • Contributing factor – Nocturnal wrist activity • Treatment – Prescribe a wrist splint to wear at night to hold wrist in neutral position

Chapter 1 Patient Interview • Recommend using: – Customary medical history – Initial Patient Questionnaire (Chapter 2) • Speeds acquiring information • Less likely to miss information • Need to review these answers with patient – Medical and dental insurance information, etc.

Inconsistencies? • Pain and disability – Minimal pain and/or palpation tenderness, but unable to work • Pain and activities – Reports tremendous pain, but minimally restricts activities • Secondary gain? – Benefits from having disorder – May not want to improve from treatment – Relatively uncommon among TMD patients

Pain Quality • Ache, pressure, or dull – TMD’s most common pain qualities • Throbbing – TMD, usually occurs when TMD worse – Migraine headache – Referred pain, most commonly from tooth • • Throbbing pain Wakes patient up at night Increases when patient lays down Increases when patient drinks hot or cold liquids • TMJ or muscle palpation may reproduce pain complaint
: 436 -40.")
Convergence Sensitization ↑ EMG Activity J Am Dent Assoc 2008; 139(4): 436 -40.

• Burning – Minimal and combined with ache, pressure, or dull – TMD – Major component or not resolved from TMD therapy – may be neuropathic pain • Consider referring patient • Others, e. g. , electrical – Consider referring patient

Pain Parameters • Intensity – 1 -10, e. g. , 4/10 • Frequency – Constant – Daily – Weekly – Monthly • Duration

Headaches • New severe headache – Refer patient to physician to evaluate for potentially serious causes • Chronic headaches – Treatment of TMD and the cervical region can be beneficial for tension type, migraine without aura, and migraine with aura headaches • Degree of headache improvement quite varied • No clinical characteristics have been identified for which patients are more likely to obtain headache improvement from TMD or cervical therapies

When to Treat Chronic Headache • Recommend – If has significant TMD, treat TMD and may obtain significant headache improvement – If has significant neck pain, treat neck and may obtain significant headache improvement – If physicians cannot adequately control headaches with medications and has masticatory or neck tenderness, obtain treatment for the more tender area and may obtain significant headache improvement

Non-masticatory Contributors to TMD • Cervical pain – One study found 51% of TMD patients had cervical pain – May refer pain to masticatory region or cause compensatory masticatory muscle tightness • Post traumatic stress disorder (PTSD) • Fibromyalgia – 18 to 23% of TMD patients – 4% of general population • Pts with these disorders do not respond as well to TMD therapies

TMJ Noises and Inability to Open or Close Mouth • “TMJ Disc Displacements” diagram (Appendix 3) helpful for explaining these – Appendices can be copied, personalized, and reprinted • www. dentistry. blackwellmunksgaard. com/wright • select "view sample pages"

TMD Anatomy Appendix 3 Use to explain: TMJ dislocation Lateral pterygoid myospasm Myofascial pain TMJ inflammation Normal disc TMJ DD with reduction Acute TMJ DD w/o reduction Chronic TMJ DD w/o reduction

Inability to Open Wide • May be due to TMJ or muscle disorder • Determining onset and history beneficial – If intermittent • With rapid onset and resolution, probably acute disc displacement without reduction • With slow onset, probably myofascial pain and/or TMJ inflammation • Stretch mouth wider to identify limiting source – Palpate to confirm limiting source

Inability to Close • TMJ dislocation: 45 mm or greater • TMJ disc displacement with reduction: 10 -35 mm • Lateral pterygoid myospasm: a few mm or less and first contact normally with contralateral canines

Commonly Identified Contributing Factors • Some not asked in questionnaire – Identified with TMD Self-management Therapies • Appendix 4 • Neck pain and fibromyalgia • Poor sleep – May benefit from amitriptyline or nortriptyline • Tension, aggravation, or frustrations • Depression • Parafunctional habits
 Arteritis • Can mimic mild TMD symptoms • Patients over 50")
Giant Cell (Temporal) Arteritis • Can mimic mild TMD symptoms • Patients over 50 years old • Reduces blood flow to head and neck – Muscles tire within 1 -2 minutes from use – Can cause blindness • May want to refer to physician for evaluation – Immediate or routine referral

Summary True or False • TMD is most prevalent for individuals between the ages of 20 and 40. • A patient's primary diagnosis is the diagnosis for the disorder that is most responsible for the patient’s chief complaint.

• Nocturnal parafunctional habits are one of many potential perpetuating contributing factors. • It is rare for a TMD patient to have cervical pain. • If a patient is unable to open wide, the practitioner may desire to stretch the mouth beyond this limitation to help identify the location of the restriction.

Chapter 2 Review of “Initial Patient Questionnaire” • Reveals – Symptom characteristics – Many potential TMD contributing factors – Potential non-TMD causes and contributors • Review patient answers • Appendix 2 is the questionnaire

Chapter 3 Clinical Exam • From Initial Questionnaire, know which structures are concerns – TMD generally due to many structures – Determine impact from potential sources • Stimulating influence (e. g. , palpations, cold to tooth) reproduces or exacerbates pain • Alleviating influence (e. g. , anesthetic blocks) decreases symptoms

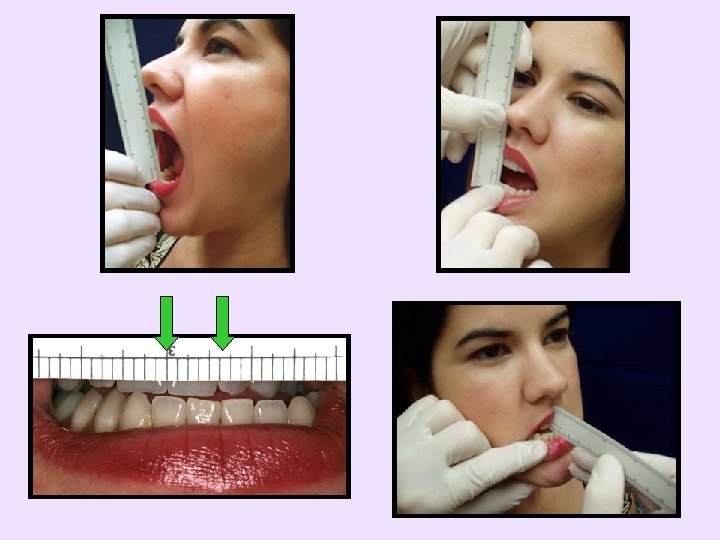
Range of Motion • Perform prior to palpating • Use consistent phrase – “Open as wide as you can” • Add overlap of teeth to incisor-toincisor opening measurement • Minimum of normal – 40 mm opening – 7 mm lateral – 6 mm protrusive

TMJ Noise • Perceive with – Fingers, stethoscope, Doppler • TMJ clicks and pops – Very prevalent among TMD and normal population – Commonly related to disc displacement with reduction • Crepitus - grating or crackling – Roughness on articular surface(s) – Could be secondary to osteoarthritis, chronic displacement without reduction, or polyarthritides • Rarely changes treatment plan

TMD Palpations • Stimulate structures to reproduce or exacerbate pain complaint • Recommend tiered approach – Initially palpate predetermined locations – Palpate over trigger point or nodule of spot tenderness – Apply firm, sustained pressure on these spots

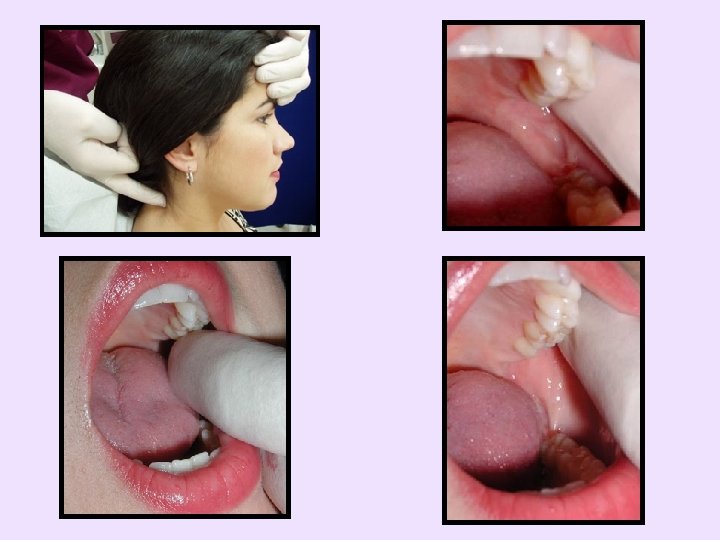
Initial TMD Palpations • Temporalis muscle, TMJ, and masseter muscle – Start with light pressure and slowly increase until create discomfort • You will see this in their eyes – Ask whether reproduce or exacerbate pain complaint • Carotid arteries, thyroid, suboccipital protuberance area – Rule out symptom contribution from these

Specifics written in handout Reproduce or exacerbate pain complaint

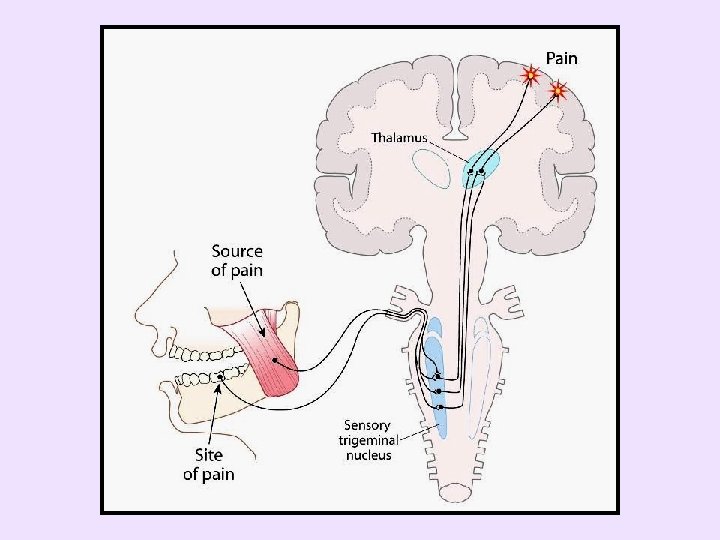
• Rule out referred pain – In spite that pain may be located where TMD pain commonly occurs, the primary source may be elsewhere

Identify referred pain

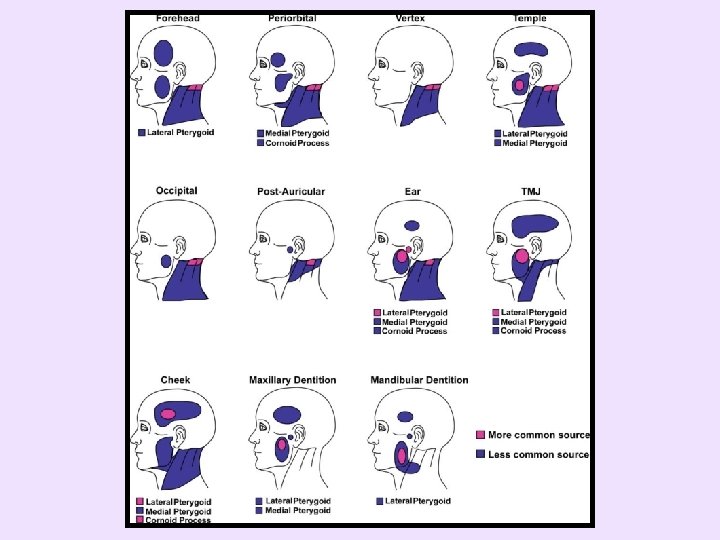
• If pain complaint reproduced or exacerbated – Palpation evaluation complete • If pain complaint not reproduced or exacerbated – Palpate the temporalis, TMJ, and masseter more intensely and/or palpate other structures • Decision varies with suspicions and clinical experience • If need help, see drawings of referred pain patterns and palpation techniques titled “Additional Palpations” in handout

• Tooth pain can be due to – Excessive forces on a tooth or the teeth • If multiple teeth tender, consider a parafunctional etiology – Referred pain from a masticatory structure • Masseter muscle trigger points are commonly involved • Do not perform endodontic procedure if pain is not eliminated once tooth anesthetized

Additional Palpations Locations • See “Additional Palpations” table


To palpate more intensely • Find and load trigger point or nodule of spot tenderness – Feel like firm knots within the muscle and more tender than surrounding muscle – Apply pressure to nodules • May refer pain to distant locations – Firm, sustained pressure to these spots • Use when attempting to refer pain to distant locations • Apply pressure up to patient tolerance for at least 5 seconds or until desired effect

Intraoral Examination • Initial Patient Questionnaire – Alerts practitioner to concerns • General oral screening – Swelling, need for restorations, etc. – Consider odontogenic pain as TMD source • Percussion and thermal tests to identify tooth • If tooth hyperresponsive, ligamentary injection to determine impact on pain complaint – If dramatically reduces or eliminates pain, determine if reversible or nonreversible disorder

Additional Evaluations • Sinus congestion – If significantly related to pain complaint • Refer to physician • Can perform medication trial to determine contribution – Sudafed (pseudoephedrine HCl) 60 mg 4 -6 h – Afrin (oxymetazoline HCl) 0. 05%, 2 sprays per nostril q 12 h – Augmentin (amoxicillin/clavulanate) 500 mg b. i. d. for 10 days • Widespread pain – Refer to primary care provider, internist, or rheumatologist

Additional Evaluations • Non-reproduced TMD type pain – – – Sustained clenching may reproduce pain Can provide trial TMD therapy Many other disorders can produce this pain

Summary True or False • The primary purpose of the clinical exam is to determine the impact potential sources may be having on the patient's complaints. • Any opening less than 45 mm would be considered restricted.

• A stethoscope or Doppler should be used to determine whether a patient has TMJ noise. • If a tooth is causing TMD symptoms, it will need to have a root canal or be extracted • TMD can also cause tooth symptoms by pain referred from the masticatory structures.

Chapter 4 Imaging • Osseous portion of TMJ often assessed with – Plain radiograph – Panoramic radiograph – Axially corrected sagittal tomography – Computed tomography (CT) – Cone beam computed tomography (CBCT)

• Osseous demineralization – Common among TMD patients – Begins on condyle’s lateral pole – Primarily caused by TMJ inflammation • Commonly secondary to parafunctional habits • Identified through TMJ tenderness – Stops when TMJ inflammation resolves – Radiographic changes lag by as much as 6 months behind clinical findings • Therefore TMD treatment directed towards symptoms, not toward radiographic findings
")
• Soft-tissue portion of TMJ generally assessed with – Magnetic resonance imaging (MRI) • Attention often directed at disc position when mouth closed and maximally opened • Plain radiographs – Screens for gross changes • Transcranial can be made with standard dental X-ray unit

– Screens for gross changes, tumors, etc. – Generally the most advanced imaging needed – Condyle pseudocysts common • Lateral pterygoid muscle fovea Condylar pseudocyst

Lateral pterygoid muscle fovea

• Axially corrected sagittal tomography – True lateral projection • Can view osseous changes of the articular surface • Evaluate condylar translation • Computed tomography (CT) – Sections enable entire TMJ to be evaluated – Good for viewing TMJ ankylosis, neoplastic conditions, anomalies, etc.
 – High quality TMJ images with low")
• Cone beam computed tomography (CBCT) – High quality TMJ images with low radiation from comparatively small inexpensive unit – Currently only provides view of hard-tissues – Allows for 3 -demensional viewing Courtesy of Dr. Bill Moore, UTHSCSA
 – Used to identify disc position • May")
• Magnetic resonance imaging (MRI) – Used to identify disc position • May reach 95% accurate – Disc displacement alone not cause for TMD • 9 to 31% of asymptomatic TMJs have a disc displacement • 26 to 31% of TMD patients have a disc displacement Disc

• Arthrography – Displays contrast media injected into TMJ – Rarely used • Due to significant pain and radiation exposure • High-resolution ultrasound – Can view TMJ's hard- and soft-tissues – Hard-tissue image inferior to CBCT • If referring patient for hard-tissue image, recommend obtaining CBCT – Soft-tissues image inferior to MRI • If referring patient for soft-tissue image, recommend obtaining MRI

Imaging Strategy • Image only if reasonable expectation that information will influence patient’s treatment • Other than imaging for suspected odontogenic pathology, imaging rarely changes treatment approach

Recommendations 1. Take dental radiographs as needed 2. Take screening radiograph if suspect patient may have pathology 3. Take screening radiograph if TMJ is primary cause for patient's complaint – Unless TMJ complaint is only noise that does not need to be treated

4. Take panoramic radiograph if TMD began with or greatly worsened from trauma 5. Take panoramic radiograph if patient has pain and taking a bisphonate – i. e. , Boniva, Fosamax, Actonel, Zometa, etc. 6. Take screening radiograph if patient relates progressively increasing open bite of anterior teeth – Someone with expertise in this area should probably evaluate patient

7. May desire screening radiograph for patient with progressively increasing open bite of posterior teeth, midline deviation, or preauricular swelling – If patient does not respond to initial therapy, recommended someone with expertise in this area evaluate patient 8. Use imaging protocol if patient had Teflon-Proplast or Silastic TMJ implants placed

9. Take panoramic radiograph, if patient does not respond to TMD therapy 10. If referring patient, let receiving practitioner choose which images to request 11. Take images requested by thirdparty payer or for medicolegal reasons to document status

Summary True or False • The primary cause for condylar demineralization is TMJ inflammation • Radiographic changes lag as much as 1 month behind clinical findings • MRI is the best image to view the soft-tissue portion of TMJ

Chapter 5 TMD Diagnostic Categories • Many TMD patients have muscle pain, TMJ pain, and TMJ noise – Each finding may have a different TMD diagnosis – Therefore TMD patients often have multiple TMD diagnoses

TMD Diagnoses • Primary diagnosis – Disorder most responsible for chief complaint – If multiple structures reproduce chief complaint, the structure that most readily reproduces it • Secondary diagnosis, tertiary diagnosis, etc. – Responsible for complaint(s) to a lesser degree(s) than the primary diagnosis

Diagnostic Categories • Clinical Diagnoses – Based on patient’s history and clinical exam • Most widely accepted categories – American Academy of Orofacial Pain – Hampered by limited knowledge about TMD and limited tests • TMJ Synovitis and/or capsulitis is TMJ inflammation

TMJ Articular Disorders • Will first look at situations in which the TMJ’s disc is displaced anterior and/or medial – Adaptive changes often form pseudodisc in retrodiscal tissue • Comparatively withstands TMJ loading – Diagnoses can be • Disc displacement with reduction • Acute disc displacement without reduction • Chronic displacement without reduction

TMD Anatomy Appendix 3 Use to review: TMJ DD with reduction

• TMJ disc displacement with reduction – Most common disorder for patients with click or pop – Clinical criteria used for this diagnosis: • Palpable click or pop • If not palpable, then recent history of click or pop • If opening and closing click or pop present, the opening noise occurs at a wider opening – MRI provides more accurate diagnosis • Not 100% accurate – Does not progress unless patient has pain – Noise does not respond as well to TMD therapy as pain responds

TMD Anatomy Appendix 3 Use to review: Acute TMJ DD w/o reduction
 – Patient has sudden onset")
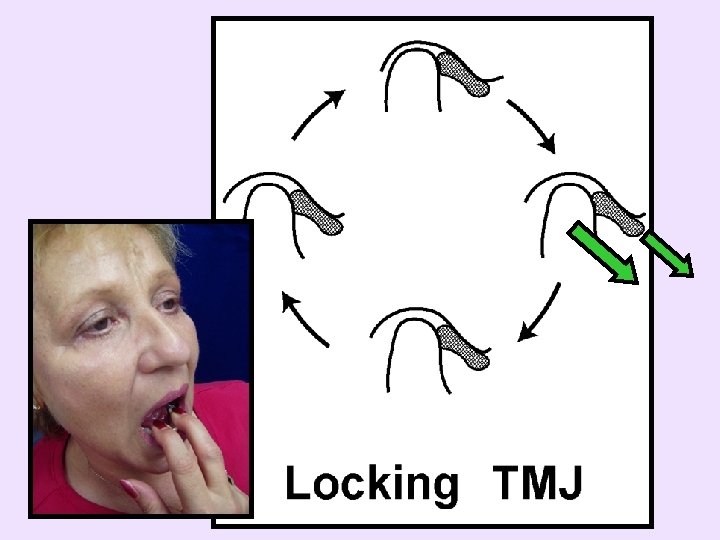
• Acute disc displacement without reduction (closed lock) – Patient has sudden onset of limited opening (less than 35 mm) • Often aware that the TMJ is blocked at the opening where it normally clicks or pops – If stretch beyond limitation, aggravates TMJ • Often have history of occurring intermittently – Suddenly occurs and suddenly releases – Time of day this generally occurs helps suggest more effective treatment options
")
– Limited opening can be due to closure muscle (e. g. , masseter muscle) disorder • Would typically exhibit a gradual onset and release • Stretching mouth beyond limitation aggravates masseter muscle – Limited opening could be due to a lateral pterygoid myospasm • Often unable to translate, providing limited opening • Generally have – A significant increase in pain when closing into MI – Teeth do not occlude into normal position • While patients with acute disc displacement without reduction have – No increase in pain when closing into MI – Teeth occlude into normal position

• Chronic displacement without reduction – Generally, patients have history of acute disc displacement without reduction (less than 35 mm opening) and gradually regain their opening (greater than 35 mm) over time (few weeks to months) – Opening increase due to stretching of the retrodiscal tissue, moving the disc anterior, enabling greater condylar translation – Course crepitus is most common noise
 – Inability to close from maximal opening – Can be")
• Dislocation (Subluxation) – Inability to close from maximal opening – Can be due to the articular eminence and/or the disc obstructing posterior movement – Conservative TMD therapies generally beneficial

• Inflammatory disorders – Identified by TMJ palpation tenderness – TMJ Inflammation • Synovitis, capsulitis, or both • Second most common diagnosis for TMD pain (first is myofascial pain) – Polyarthritides • Systemic condition (e. g. , rheumatoid arthritis) causing the TMJ as well as other joints to be tender

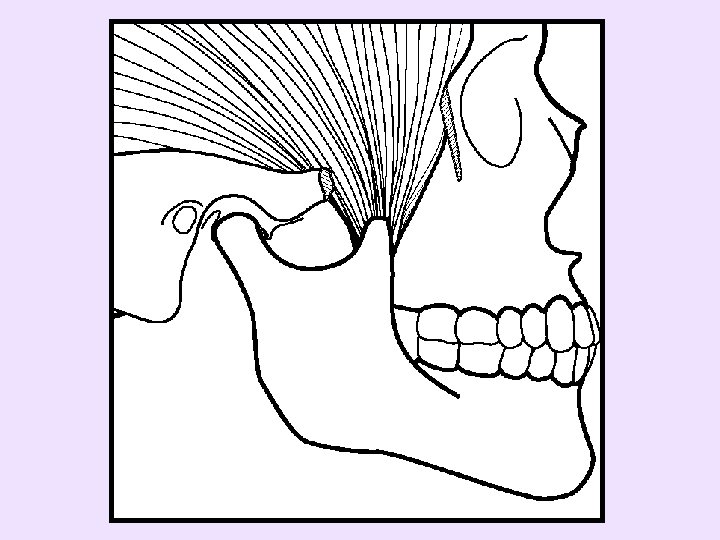
1. Inflammation may force condyle forward 2. Lateral pterygoid may contract to protect inflamed tissue

• Osteoarthritis – Diagnosed when TMJ tender to palpation and hard-tissue imaging reveals bony changes • TMJ inflammation causes articular tissue and bone degeneration; radiographic changes lag as much as 6 months behind clinical findings • Can cause condylar height collapse – Subcategories: • Primary osteoarthritis - when due to TMJ overloading (e. g. , clenching) • Secondary osteoarthritis - when due to direct trauma

• Ankylosis – Very limited opening, generally not associated with pain – Can attempt to force mouth open wider to determine restrictive structure – Conservative TMD therapies not beneficial and patient will need TMJ surgery – Subcategories: • Fibrous ankylosis • Bony ankylosis

• Fracture • Congenital or developmental disorders – Aplasia – Hypoplasia – Hyperplasia – Dysplasia – Neoplasia

Masticatory Muscle Disorders • Myofascial Pain – Most common diagnosis for TMD pain – Muscles have localized firm nodules more tender than surrounding muscle called trigger points or nodules of spot tenderness • Palpation cause local pain, pain at distant locations (referred pain), and/or autonomic symptoms – Sustained nodule palpation maximizes these effects – Aggravated by muscle use, stress, cold, etc.

• Myofascial Pain, continued – Temporarily relieved by trigger point therapies – Regional involvement of muscle and/or fascia • While fibromyalgia is systemic disorder causing widespread aching or stiffness in all quadrants of body and tenderness of at least 11 of 18 fibromyalgia tender points – If muscle is tender to palpation and none of the other muscle diagnoses better describe the patient’s condition, recommend be diagnosed as myofascial pain – Traditional TMD therapies have been shown to reduce masticatory myofascial pain

• Myositis – Muscle inflammation due to spreading infection, external muscle trauma, or muscle strain – If due to infection, must treat the infection to resolve the condition – Additionally, condition can be treated with nonsteroidal anti-inflammatory drugs (NSAIDs), limiting muscle use, and possibly ice within first 48 hrs after trauma or muscle strain • TMD Self-management Therapies handout (Appendix 4) may be helpful

• Myospasm – Involuntary contracture of muscle • e. g. , awaking with calf muscle cramp – Painful or unable to move foot up or down; foot stuck in middle of ROM position – Inferior lateral pterygoid myospasm • Painful or unable to move mandible from partially translated position – Painful or unable to occlude teeth into MI – Contralateral canines usually first to occlude – Painful or unable to open wide • Will discuss in Chapter 9, “Lateral Pterygoid Myospasm”


• Myospasm, continued – Closure muscle myospasm, e. g. , medial pterygoid myospasm secondary to inferior alveolar nerve block • Treat in a tiered approach – TMD Self-management Therapies (Appendix 4) – Stretch muscle to tolerance, 30 to 60 seconds – Ibuprofen and diazepam – Appliance therapy

• Myofibrotic Contracture – Fibrous adhesions within muscle causes muscle to not be able to stretch to full length • Painless unless combined with other painful muscle disorder – If due to closure muscle • Causes limited opening • Practitioner can forcibly stretch mouth to determine if restriction of muscle or TMJ origin – Can occur with inferior lateral pterygoid muscle • From continuous wear of anterior positioning appliance – Traditional TMD therapy not beneficial

• Local Myalgia – Other painful muscle disorders without distinguishing clinical characteristics, e. g. , protective muscle splinting, delayed onset muscle soreness, etc. • Neoplasia

Summary True or False • TMD patients generally have only one diagnosis. • A pseudodisc can form in the TMJ’s retrodiscal tissue. • TMJ disc displacement with reduction is the most common diagnosis for a patient with a TMJ click or pop.

• A patient diagnosed with an acute disc displacement without reduction has an opening less than 35 mm. • TMJ inflammation is the most common TMD diagnosis. • Stress does not aggravate myofascial pain. • Fibromyalgia and myofascial pain are the same disorders.

Chapter 6 Contributing Factors • TMD Contributing Factors – Directly or indirectly contribute to TMD – Types • Predisposing contributing factors • Initiating contributing factors • Perpetuating contributing factors

Predisposing Contributing Factors • Elements making individual more susceptible to develop TMD – Fingernail biting, nocturnal parafunctional habits, daytime parafunctional habits, etc. • Cause individuals to be predisposed to TMD

Initiating Contributing Factors • Event that caused TMD to develop – – – Trauma to jaw, placement of crown, etc. 61% unknown cause 7% dental treatment • Perform cursory TMD evaluation prior to dental treatment – – – Suggests patient’s TMD propensity Documents preexisting condition Cursory evaluation and preventing aggravation discussed in Chapter 8 "TMD Secondary to Dental Treatment"

Perpetuating Contributing Factors • Directly or indirectly aggravate masticatory system and prevent TMD symptoms from resolving • Determine these factors and degree contributing to symptoms • Will first alter those that are easiest to change and provide greatest impact on symptoms

Daily Symptom Pattern Provides Indications When Contributing Factors Occur • Awakes with symptoms that rapidly resolve – Primary contributing factors occur at night, e. g. , nocturnal parafunctional habits, stomach sleeping, etc.

• Awakes without symptoms and develop as day progresses – Primary contributing factors occur during day – Generally due to excessive muscle activity • Holding excessive tension in masticatory muscles • Performing excessive parafunctional activities – Generally increase when individual busy, frustrated, concentrating, e. g. , using computer, driving, etc. – Daytime contributing factors under patient’s control to change

• Some residual effect carries over to other portion of day • Awakes with symptoms and has symptoms throughout day – Suggests patient has daytime and nocturnal contributing factors – May have daily severity pattern suggesting one is more prominent, but generally both need to be addressed

Contributing Factors are a Broad Continuum • For ease of understanding, presented in categories of biological, behavioral, emotional, cognitive, social, and environmental

Biological • Mechanically or biologically contribute to TMD – Neck pain – Poor posture – Malocclusion – Insomnia – Systemic Diseases • Fibromyalgia • Rheumatoid arthritis

Behavioral • Frequent habits that contribute to TMD – Holding excessive tension in the masticatory muscles – Clenching – Fingernail biting – Stomach sleeping – Telephone cradling

Percent of Nonfunctional Tooth Contacts Daytime Oral Habits Alerted subjects every 20 minutes Chen CY et al. J Orofac Pain 21(3): 185 -93.

Emotional • Prolonged negative emotions – Depression – Worry – Anxiety – Anger

Muscle Activity / Hour of Sleep Nocturnal Masseter Muscle Activity 120 100 School exam Skipped exam, upset Sick 80 60 40 20 0 0 5 10 15 20 Days Rugh JD, Robbins JW. Oral Habits Disorder. 25 30 35

Muscle Activity / Hour of Sleep Nocturnal Masseter Muscle Activity 300 Job interview 250 Quit job Fight with father 200 150 100 Vacation in Hawaii 50 0 0 5 10 15 20 Days Rugh JD, Robbins JW. Oral Habits Disorder. 25 30 35

Cognitive • Harmful thought processes or low cognitive skills – Negative self-statements – Poor reasoning skills making it difficult for patient to work with self-management or other instructions

Social • Interactions with others that contribute to TMD symptoms or poor therapeutic response – Coworker difficulties – Lack of social support – Secondary gain • Benefit from disorder

Environmental • Usually difficult to identify, so infrequently explored among TMD patients – Food additive causing migraine headaches – Seasonal affective disorder causing depression

TMD Therapies Generally • Not directed at physically changing diagnosis – For example, myofascial pain • Directed at reducing perpetuating contributing factors – Body then able to heal itself – Similar to treatment of mild generalized periodontal disease • Increase oral hygiene, improve nutrition, etc.

Identifying Perpetuating Contributing Factors • Use daily symptom pattern • For daytime symptoms, may need to ask patient to hourly record pain and activity so can identify associations – Then patient needs to identify the perpetuating contributing factor, e. g. , clenching, etc.

Summary • Why should a cursory TMD evaluation be performed prior to providing dental treatment? • What is the difference between predisposing, initiating and perpetuating contributing factors? • Why are TMD therapies generally directed at reducing the perpetuating contributing factors?
- Slides: 128