Radiotherapy Treatment Planning Treatment planning is the task









 = clinically demonstrated tumor")















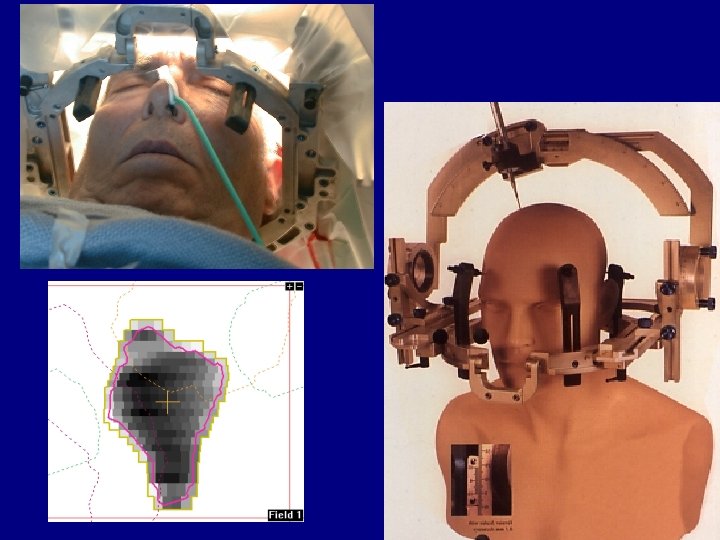
 Marking the Patient already during CT Moveable Lasers Isocenter")












")




 in(as above")












- Slides: 59
Radiotherapy Treatment Planning
Treatment planning is the task to make sure a prescription is put into practice in an optimized way Prescription Planning Treatment Anwar 2
Objectives l l Understand the general principles of radiotherapy treatment planning Appreciate different dose calculation algorithms Understand the need for testing the treatment plan against a set of measurements Be able to apply the concepts of optimization of medical exposure throughout the treatment planning process Anwar 3
Contents of the lecture A. Radiotherapy treatment planning concepts B. Computerized treatment planning Anwar 4
The need to understand treatment planning IAEA Safety Report Series 17 “Lessons learned from accidental exposures in radiotherapy “ (Vienna 2000): l About 1/3 of problems directly related to treatment planning! l May affect individual patient or cohort of patients l Anwar 5
A. Basic Radiotherapy Treatment Planning Concepts i. Planning process overview ii. Patient data required for planning iii. Machine data required for planning iv. Basic dose calculation Anwar 6
i. Planning process overview l l l Combine machine parameters and individual patient data to customize and optimize treatment Requires machine data, input of patient data, calculation algorithm Produces output of data in a form which can be used for treatment (the ‘treatment plan’) Patient information Treatment unit data Planning Treatment plan Anwar 7
ii. Patient information required l l Radiotherapy is a localized treatment of cancer - one needs to know not only the dose but also the accurate volume where it has been delivered to. This applies to tumor as well as normal structures - the irradiation of the latter can cause intolerable complications. Again, both volume and dose are important. Anwar 9
One needs to know Target location l Target volume and shape l Secondary targets - potential tumor spread l Location of critical structures l Volume and shape of critical structures l Radiobiology of structures l Anwar 10
Target delineation ICRU 50 & 62 Gross Tumor Volume (GTV) = clinically demonstrated tumor Clinical Target Volume = GTV + area at risk (eg. potentially involved lymph nodes) Anwar 11
It all comes down to the correct dose to the correct volume Comparison of three different treatment techniques (red, blue and green) in terms of dose to the target and a critical structure Critical organ Target dose Dose Volume Histograms are a way to summarize this information
The ideal DVH l Tumor: n n l High dose to all Homogenous dose 100% Critical organ n Low dose to most of the structure 100% dose Anwar 13
Need to keep in mind Always a 3 D problem l Different organs may respond differently to different dose patterns. l Question: Is a bit of dose to all the organ better than a high dose to a small part of the organ? l Anwar 15
In practice not always that clear cut l l l ICRU report 62 Need to understand anatomy and physiology A clinical decision Anwar 16
In many organs, dose and volume effects are linked - eg. Boersma* et al. , classified the following (Dose, Volume) regions to be regions of high risk for developing rectal bleeding: *Int. J. Radiat. Oncol. Biol. Phys. , 1998; 41: 84 -92. Anwar 17
In EBT practice l Need to know n where to direct beam to, and n how large the beam must be and how it should be shaped Anwar 18
Target design and reference images l In radiotherapy practice the target is localized using diagnostic tools: n Diagnostic procedures - palpation, X-ray, ultrasound n Diagnostic procedures - MRI, PET, SPECT n Diagnostic procedures - CT scan, simulator radiograph Anwar 19
Selection of treatment approach Requires training and experience l May differ from patient to patient l Requires good diagnostic tools l Requires accurate spatial information l May require information obtained from different modalities l Anwar 20
Minimum patient data required for external beam planning l l Target location Patient outline Anwar 21
Diagnostic tools which could be used for patient data acquisition l l l CT scanner, MRI, PET scanner, US, … Simulator including laser system, optical distance indicator (ODI) Many functions of the simulator are also available on treatment units as an alternative - simulator needs the same QA! Anwar 22
Note on the role of simulation l Simulator is often used twice in the radiotherapy process n Patient data acquisition - target localization, contours, outlines n Verification - can the plan be put into practice? Acquisition of reference images for verification. l Simulator may be replaced by other diagnostic equipment or virtual simulation Anwar 23
Virtual simulation All aspects of simulator work are performed on a 3 D data set of the patient l This requires high quality 3 D CT data of the patient in treatment position l Verification can be performed using digitally reconstructed radiographs (DRRs) l Anwar 24
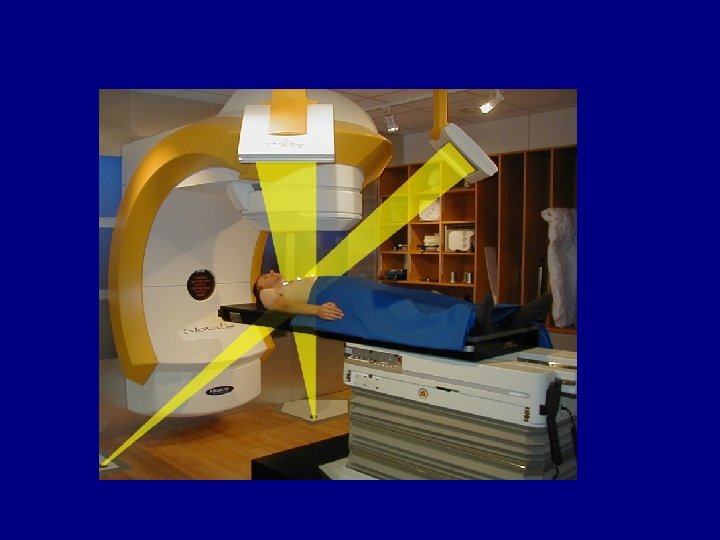
Virtual Simulation 3 D Model of the patient and the Treatment Devices Anwar 25
Simulator Rotating gantry Diagnostic X-ray tube Radiation beam defining system Simulator couch Nucletron/Oldelft Anwar Image intensifier and X-ray film holder 26
Radiotherapy simulator l Anwar Obtain images and mark beam entry points on the patient 27
CT Simulation (Thanks to ADAC) Marking the Patient already during CT Moveable Lasers Isocenter Position CT images Anwar Isocenter Projection 28
Patient marking Marks on shell l Create relation between patient coordinates and beam coordinates Tattoos Anwar Skin markers 29
Beam placement and shaping DRR with conformal shielding simulator film with block Anwar 42
Tools for optimization of the radiotherapy approach l l l l Choice of radiation quality Entry point Number of beams Field size Blocks Wedges Compensators Anwar 43
Optimization approaches Choice of best beam angle beam target patient wedge target Use of a beam modifier Anwar patient 44
Beam number and weighting beam Beam 1 100% 50% target patient Beam 2 patient 40% 30% 10% 20% Anwar 45
A note on weighting of beams Different approaches are possible: 1. Weighting of beams as to how much they contribute to the dose at the target 2. Weighting of beams as to how much dose is incident on the patient 25% 40% 25% 30% These are NOT the same 10% 25% Anwar 46
Use of wedges Wedged pair l Three field techniques l Isodose lines patient Typical isodose lines Anwar 47
Beam placement and shaping l l l Entry point Field size Blocks Wedges Compensators a two-dimensional approach? Anwar 48
Beam placement and shaping l l l Entry point Field size Blocks Wedges Compensators ü ü ü Multiple beams Dynamic delivery Non-coplanar Dose compensation (IMRT) not just missing tissue Biological planning This is actually a 3 D approach Anwar 49
Target Localization l l l Diagnostic procedures - palpation, X-ray, ultrasound Diagnostic procedures - MRI, PET, SPECT Diagnostic procedures - CT scan, simulator radiograph Allows the creation of Reference Images for Treatment Verification: Simulator Film, Digitally Reconstructed Radiograph Anwar 50
Simulator image l l Anwar During ‘verification session’ the treatment is set-up on the simulator exactly like it would be on the treatment unit. A verification film is taken in ‘treatment’ geometry 51
Simulator Film l l Field defining wires Anwar Shows relevant anatomy Indicates field placement and size Indicates shielding Can be used as reference image for treatment verification 52
iii. Machine data requirements for treatment planning l l l Beam description (quality, energy) Beam geometry (isocentre, gantry, table) Field definition (source collimator distance, applicators, collimators, blocks, MLC) Physical beam modifiers (wedges, compensator) Dynamic beam modifiers (dynamic wedge, arcs, MLC IMRT) Normalization of dose Anwar 57
Machine data required for planning l Depends on n n l l complexity of treatment approaches resources available for data acquisition May be from published data or can be acquired MUST be verified. . . Anwar 58
Quick Question: Who is responsible for the preparation of beam data for the planning process?
Acquisition of machine data l l …from vendor or publications (eg BJR 17 and 25) - this requires verification!!! Done by physicist Some dosimetric equipment must be available (water phantom, ion chambers, film, phantoms, …) Documentation essential Anwar 60
Machine data availability l l l Hardcopy (isodose charts, output factor tables, wedge factors, …) - for emergencies and computer break downs Treatment planning computer (as above or beam model) - as standard planning data Independent checking device (eg. mu checks) - should be a completely independent set of data Anwar 61
Machine data availability Hardcopy (isodose charts, output factor tables, wedge factors, …) in(as above d e i f i l Treatment planning computer r e , v d e t a d be e c t r s u u o s m t) ta or beam model) he The da tervals and t ponsible for i s in e r r a l n u o s g er re p l Independent checking device (eg. mu e h t g n i d d u nte e (incl m u c do checks) e b t s mu l Anwar 62
Machine data summary l l Need to include all beams and options (internal consistency ﺍﻟﻠﺰﻭﺟﺔ ، ﺍﻟﻘﻮﺍﻡ , conventions, collision ﺗﺼﺎﺩﻡ protection, physical limitations) Data can be made available for planning in installments as required Some data may be required for individual patients only (eg. special treatments) Only make available data which is verified Anwar 63
Quick Question: What data is available for physical wedges in your center? This should include at least: l. Wedge angle - and how it is defined l. Wedge output modification factor - and to which depth and field sizes it applies l. The field sizes for which the wedge can be used l. Beam hardening? Maybe a new beam must be defined by TMRs or percentage depth dose l. Profiles in both directions (wedged and un-wedged the latter is affected by divergence related profile changes) l. Weight (eg for OHS restrictions on lifting)
From single to multiple beams l Mainly an issue for megavoltage photons where we have significant contribution of dose to the target from many beams 1 3 2 60 Gy 4 Beam weighting must be factored in !!! Anwar 65
Compensators l Physical compensators n lead sheets n brass blocks n customized milling l Intensity modulation n multiple static fields n arcs n dynamic MLC Anwar 66
Intensity modulation Can be shown to allow optimization of the dose distribution l Make dose in the target homogenous l Minimize dose out of the target l Different techniques l n physical compensators n intensity modulation using multi leaf collimators Anwar 67
Intensity Modulation l l MLC pattern 1 MLC pattern 2 Achieved using a Multi Leaf Collimator (MLC) The field shape can be altered n n either step-by-step or dynamically while dose is delivered Anwar MLC pattern 3 Intensity map 68
iv. Basic dose calculation l Once one has the target volume, the beam orientation and shape one has to calculate how long a beam must be on (60 -Co or k. V X-ray units) or how many monitor units must be given (linear accelerator) to deliver the desired dose at the target. Anwar 69
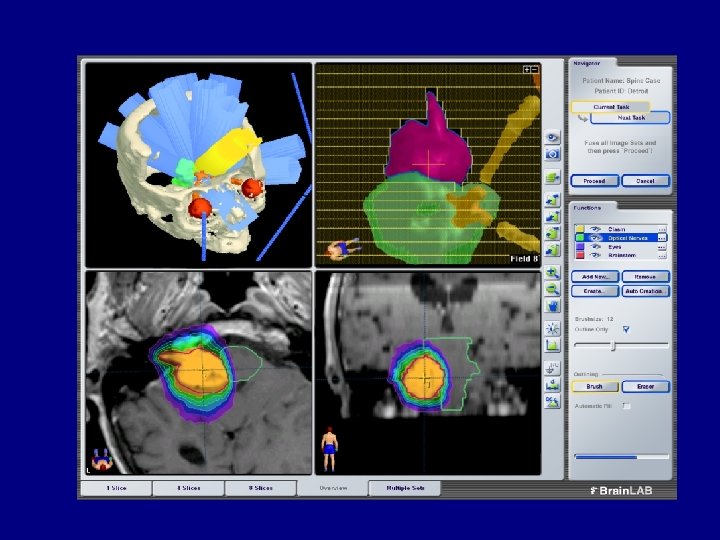
3 D display of beam placement may help to identify the structures in the field. Anwar 70
Dose calculation Anwar 71
Dose display options Color wash Isodose lines Anwar 72
Isodose display - can be complex and 3 D Anwar 73
Anwar 74