Chapter 3 CBT Assessment Case Formulation and Treatment

+ Chapter 3 CBT Assessment, Case Formulation, and Treatment Planning

CBT Assessment, Case + Formulation and Treatment Planning

CBT Assessment, Case + Formulation, and Treatment Planning n CBT requires a purposeful process in determining the most effective treatment approach n Stated differently, before developing a formal case formulation, there needs to be an assessment process through a CBT lens n True CBT treatment planning needs to be based off of a working and malleable CBT case formulation n Four interconnected parts: Intake interview basics n CBT assessment n CBT case formulation n CBT treatment plan n

+ Intake Interview Basics

+ Intake Interview Basics n The initial, formal assessment process is often referred to as an “intake” in most agencies Collaborative empiricism begins here n Typically semistructured n Includes specific questions that must be asked based on agency (and perhaps managed care) expectations and follow-up questions that you ask at your own discretion based on information provided by the client n n Table n 3. 1 – Common Intake Information Gathered Presenting problems and symptoms will be addressed in the next section “CBT Assessment”

May influence core belief development

+ CBT Assessment

+ CBT Assessment n Key focus should be on the presenting problems for each client (go beyond formal DSM diagnosis) n Important to understand the precipitating and maintaining mechanisms of these problems n. A well-done CBT assessment will set the stage for developing a working cognitive-behavioral case formulation n A detailed and accurate case formulation allows the best chance for ameliorating client distress CBT treatment plan

+ CBT Assessment n When clients arrive for their intake session they often do not truly know “what’s wrong” with them n They just know that they are experiencing some type of distress beyond their level of comfort and ability to cope, and there may be external indicators that something is not right n It is up to therapist to help clients develop an understanding of their problems n The CBT assessment process provides a clearer understanding of what precipitates and maintains clients’ presenting distress and problems

+ CBT Assessment n Table n 3. 2 – Specific CBT Assessment Information The following slides explains each of these key content areas in more detail

+ CBT Assessment Compatibility with CBT

+ Compatibility with CBT n. A common myth is that only high-cognitive-functioning individuals can benefit from CBT n You are not being selective of who can receive CBT; this is contraindicative of CBT n Look at compatibility with CBT on a continuum (i. e. , low to high) to help inform your approach to psychoeducation and interventions n Consider the following: Ability to establish a therapeutic alliance n Ability to identify automatic thoughts and associated emotions n Ability to work within a goal- and problem-oriented focus n

+ Ability to Establish a Therapeutic Alliance n Having at least a basic sense of your clients’ expectations can inform your approach in providing: Psychoeducation – e. g. , explicitness, details, examples, and follow-ups n Therapeutic relationship development – e. g. , empathy with language conveying client autonomy, eliciting feedback, and proposing that the client engage in a mutual task n n The n issue is often not with clients It is up to you to make sure that your clients feel comfortable with CBT and have a clear understanding of therapeutic expectations

+ Ability to Identify Automatic Thoughts and Associated Emotions n Look at this ability more as a potential strength than as a possible weakness n This is a skill that can be improved on over the course of therapy n It would be ironic to consider potential clients not suitable for CBT if their thought and emotion identification skills were poor and/or they had extreme negative thoughts n This is probably the very reason they need therapy!

+ Ability to Work Within a Goal- and Problem-Oriented Focus n This ability should also be viewed as a potential strength rather than a weakness n Explaining the expectation of goal- and problem-oriented focused therapy early, along with a collaborative approach during the treatment planning process, can dramatically improve therapeutic outcomes

+ CBT Assessment Presenting Problems

+ Problem Identification, Frequency, Duration, and Intensity n Identification, frequency (e. g. , number of panic attacks), duration (e. g. , few minutes and quick recovery or 15 minutes and disoriented afterwards), and intensity (e. g. , severity rating on a 0 -10 scale) n Not all problems can be assessed in this manner, but, when possible, this information can be the beginning of establishing baselines for specific problems

+ Impact on Daily Life n Consider the following: Interpersonal relationships (e. g. , friends, colleagues, family, romantic partner) n Work/school productivity n Ability to initiate and complete daily tasks n n This information can also be helpful in establishing current baselines n As much as decreasing symptom distress is important for treatment goals, so is improving quality of life through interpersonal relationships, work/school productivity, and daily tasks
 n This can range from a single")
+ Precipitating Factors n Initiate/start the problem(s) n This can range from a single life event (e. g. , traumatic accident) to a series of daily stressors that “added up” over time (e. g. , multiple work deadlines and constant arguing with partner) n Each problem my have its own trigger mechanisms n In some cases, the precipitating factors for the presenting problems may be intertwined n Knowing how clients’ distress and impairment began can offer initial insight into how they perceive life events and correspondingly respond and cope
 n Consider: what has not")
+ Maintaining Factors n Continue or exacerbate the problem(s) n Consider: what has not worked or made things worse and what has worked (at least in part) to cope with their distress and impairment n General examples of client maintaining factors include cognitive distortions, escape/avoidance behaviors, and poor problem-solving skills

+ Maintaining Factors n There may also be other factors that are more external to the client that are maintaining the problem (e. g. , being laid off from work or recent death in the family) n. A deeper understanding of clients’ maintaining factors provides initial insight into their automatic thoughts and associated behavioral tendencies and coping skills

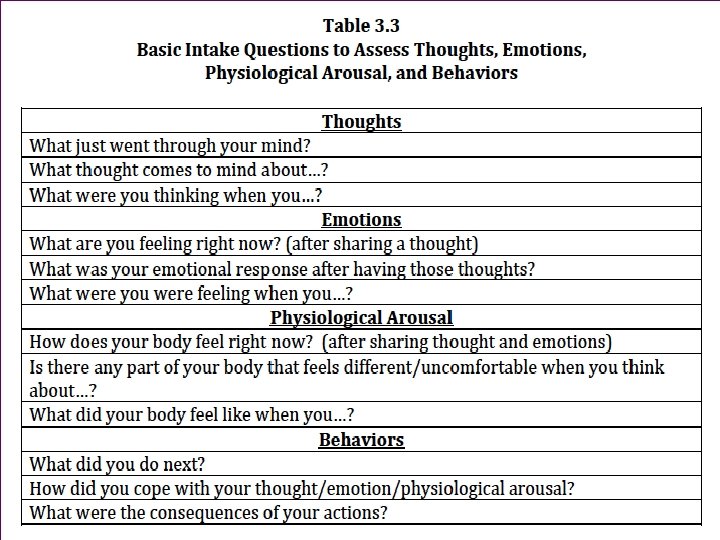
+ Automatic Thoughts, Emotions, and Associated Behavioral Responses n The fundamental focus during assessment is to at least ascertain a few common automatic thoughts that occur immediately after an event n It is often too early to accurately identify core beliefs during the intake, but it does not hurt to take any notes if they are observed n Focus on a specific event and ask clients what they are thinking n Ask for any associated emotions related to the event-thought n You can also ask clients how their body feels when distressed n Follow-up with assessing how clients behave during and after the event n Ask about the outcomes or consequences of their behaviors

+ Automatic Thoughts, Emotions, and Associated Behavioral Responses n Table 3. 3 – Basic Intake Questions to Assess Thoughts, Emotions, Physiological Arousal, and Behaviors n When gathering information about presenting problems, especially within the context of automatic thoughts, it is best to use specific examples n Especially examples that are prominent in the client’s mind – tend to be more emotional in content n Examples that are emotionally laden are often ideal because they bring past events more into the present (i. e. , in-the-moment distress)
 n PDA-1: CBT Assessment—Presenting")
+ Presenting Problems n Video Vignette 3. 1 (p. 42) n PDA-1: CBT Assessment—Presenting Problems n *Focuses on problem identification, frequency, duration and intensity; impact on daily life n Discussion Questions 3. 1 (p. 45) n Video Vignette 3. 2 (p. 45) n MDD-1: CBT Assessment—Presenting Problems n *Focuses on precipitating and maintaining factors; automatic thoughts, emotions, and behaviors n Discussion Questions 3. 2 (p. 48) n Activity 3. 1: CBT Assessment—Presenting Problems (p. 48)

+ CBT Assessment Motivation and Responsibility for Change

+ Motivation and Responsibility for Change n Research consistently shows that the more clients are motivated to change, including hope and optimism, the better therapeutic outcomes they have relative to clients who are not motivated to change n Consider these four domains: How much does the client actually want to change (i. e. , motivation)? n What does the client expect to get out of therapy? n What is the client’s own perception of responsibility for change (i. e. , internal vs. external)? n Does the client have any hope or optimism that therapy will help? n

+ Motivation and Responsibility for Change n Video n PDA-2: CBT Assessment—Motivation to Change n Video n Vignette 3. 3 (p. 50) Vignette 3. 4 (p. 50) MDD-2: CBT Assessment—Motivation to Change n Discussion Questions 3. 3 (p. 53)

+ CBT Assessment Formal Symptom Measures and Formative Assessment

+ Formal Symptom Measures and Formative Assessment n Assessment is a formative process where monitoring client progress is continuous with ongoing feedback Assessment in therapy is not a “one-shot” event at the beginning and end of therapy n Therapists who continuously assess client symptom distress have better client outcomes compared to therapists who do not n n Formative assessment provides feedback to make any necessary therapeutic modifications that need to be made during therapy instead of finding out at the end of therapy (which is often too late)

+ Formal Symptom Measures and Formative Assessment n Assessment can provide information that might not be stated verbally n Sometimes it is helpful to review responses to individual assessment questions – information can be used for sensitive follow-up inquires for clarification n It is often best to administer formal assessments right before the intake session starts n Most symptom assessments are client self-report (or caregiver) measures that typically do not take much time to complete n n They are also relatively easy to score and interpret Can provide client immediate feedback while in session

+ Formal Symptom Measures and Formative Assessment n Video n PDA-3: CBT Assessment—Measures n Video n Vignette 3. 5 (p. 54) Vignette 3. 6 (p. 55) MDD-3: CBT Assessment—Measures n Discussion n Activity Questions 3. 4 (p. 56) 3. 2: CBT Assessment—Measures (p. 57)

+ CBT Case Formulation

+ CBT Case Formulation n CBT case formulation is vital for purposeful, efficient, and effective treatment planning n It is a cognitive-behavioral conceptualization of the presenting problems, associated symptoms, and contributing factors n Case formulations should be modified throughout treatment as new information is gathered and clients make progress towards their goals

+ CBT Case Formulation n There should always be some level of input and involvement from clients when developing your case formulation and treatment plan n Models CBT collaboration and can increase motivation and hope for change

+ CBT Case Formulation n The following are the key components that should be included in a CBT case formulation n Based on guidelines established by the Academy of Cognitive Therapy: n n n Precipitating and maintaining factors summary Cross-sectional view of cognitions, emotions, and behaviors Longitudinal view of cognitions, emotions, and behaviors Working hypothesis DSM diagnosis

+ Precipitating and Maintaining Factors Summary n Precipitants are considered significant life events that have contributed to the development of the client’s current distress n Activating situations are small-scale events (i. e. , typical dayto-day activities) that incite clients’ preexisting dysfunctional thoughts, emotions, and behaviors n Maintaining factors are key actions or events that continue or exacerbate the effect of the precipitants n Focus on what the client has done to cope when experiencing distress – effective and ineffective strategies
 patterns")
+ Cross-Sectional View of Cognitions, Emotions, and Behaviors n Current (“here and now”) patterns of precipitants and activating situations that incite negative automatic thoughts, emotions, physiological sensations, and behaviors n Focuses on the automatic thought patterns typically identified during the intake and early sessions n Early in therapy, the cross-sectional view will have the most practical utility

+ Longitudinal View of Cognitions, Emotions, and Behaviors n Takes into account developmental events and other possible life-shaping influences n Develops more fully as therapy proceeds as underlying core beliefs become more salient and understood n Includes enduring patterns of maladaptive behaviors that have mostly been reinforcing and/or maintaining distress n Initially information may be minimal soon after the client intake, but will evolve over time with more in-depth knowledge of your client

+ Working Hypothesis n Look at this as a “CBT story” of how clients came to their current distress n Primary focus is on the development of clients’ present problems and symptoms n Whenever possible, integrate clients’ strengths/assets and any relevant sociocultural factors n If possible, hypothesize on how clients see themselves, others, the world, and their future

+ Working Hypothesis n Your working hypothesis will have a direct influence on the development of your treatment goals and interventions This is truly a working hypothesis – it is a tentative understanding of your clients’ symptoms and distress n It should be well informed by current client information but also flexible enough to be modified when new and/or contradicting information is presented n n *The quality of your treatment plan is only as good as the quality of your CBT case formulation, and the working hypothesis is its driving force

+ DSM Diagnosis n. A formal diagnosis has its value Required by agency and reimbursement from managed care n Provides clarity for sources of distress through consolidating multiple symptoms n It can provide general guidance for treatment direction n n Ultimately, the focus of your treatment should go beyond formal diagnostic symptoms n Considering symptoms, problems, and levels of distress negatively impacting daily functioning is most pragmatic for clinical reasons

+ CBT Case Formulation n Sample Form 3. 1 – CBT Case Formulation and Treatment Plan Template (p. 60) Note that in addition to CBT-related information from assessment, common intake information (case history) should also be included n The CBT treatment plan portion will be discussed next n

+ CBT Treatment Plan

+ CBT Treatment Plan n The information gathered from your CBT assessment and integrated into your CBT case formulation becomes the foundation and driving force for you CBT treatment plan n Naturally, modifications will be made to the treatment plan over the course of therapy n Modifications should be based on clients making therapeutic progress and an evolving case formulation n Overall, it is essential to have consistency across your case formulation and treatment plan while integrating empirically based interventions

+ CBT Treatment Plan n The information gathered from your CBT assessment and integrated into your CBT case formulation becomes the foundation and driving force for you CBT treatment plan n Naturally, modifications will be made to the treatment plan over the course of therapy n Modifications should be based on clients making therapeutic progress and an evolving case formulation n Overall, it is essential to have consistency across your case formulation and treatment plan while integrating empirically based interventions

+ CBT Treatment Plan n The following are the key components of a CBT treatment plan: Problem list n Treatment goals and interventions n Anticipated obstacles n

+ Problem List n Brief description of any significant problems identified by you and your client to be of primary focus during treatment n There n is no ideal minimum or maximum number Depends on clients’ distress and needs – typically 3 -6 problems n Should act as an anchor for your proceeding treatment goals and interventions

+ Treatment Goals and Interventions n There should be a logical connection between each treatment goal, the problem list, and the case formulation n Treatment n goals are desired client outcomes Indicators of therapeutic progress by way of reduced symptom distress and improved quality of life n Goals are therapeutic indicators – should be objective and measureable n Allows for accurate tracking of treatment progress for both therapist and client (and managed care) n Table 3. 4 – Treatment Goals: Poor Versus Better

+ Treatment Goals and Interventions

+ Treatment Goals and Interventions n If goals are desired client outcomes, then interventions are the processes to achieve the outcomes n Interventions indicate what needs to be done in order to meet each goal n Effectiveness and clarity is improved when interventions are linked to each goal n There needs to be at least one intervention per goal, but there is no maximum (generally 2 -4 interventions per goal) n Interventions should be client specific and describe the process n Table 3. 5 – Treatment Interventions: Poor Versus Better

+ Treatment Goals and Interventions

+ Anticipated Obstacles n The purpose of this section is to prepare for and anticipate potential factors that might impede therapeutic process n Largely a preventative approach n Therapeutic Relationship Considerations There may be times when there are current or potential problems that could hinder therapeutic relationship n If possible, you can indicate possible problem-focused and/or interpersonal approaches that can be used to help repair the relationship or avoid future damage to the relationship n

+ Anticipated Obstacles n Client-Specific n There may be particular elements of client distress that may require additional attention than typically necessary n e. g. , a client who has generalized anxiety disorder may have an exceptionally perfectionistic personality trait n External n Factors Sometimes there are external factors that are outside of control of therapist-client therapeutic relationship n The external nature of such factors does not preclude you from taking the necessary steps to minimize the impact of these factors through problem-solving and coping skills

+ CBT Treatment Plan n Sample Form 3. 1 – CBT Case Formulation and Treatment Plan Template (p. 60) n Review again and note the integration of the CBT treatment plan n Activity 3. 3: CBT Case Formulation and Treatment Plan (p. 67)

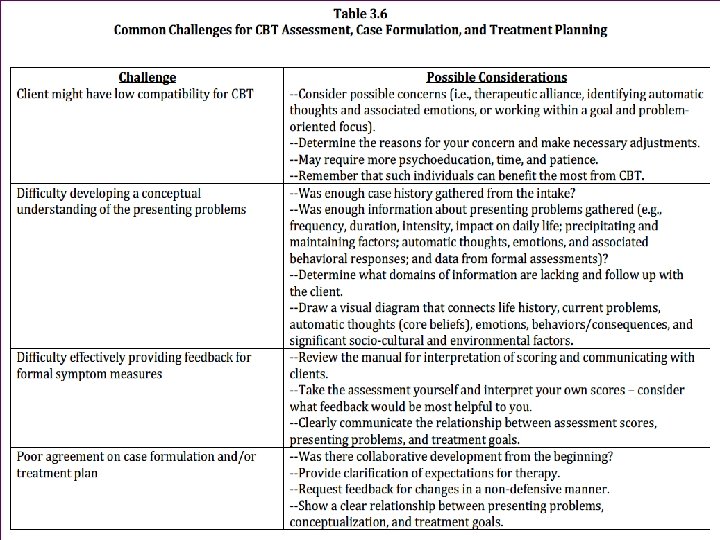
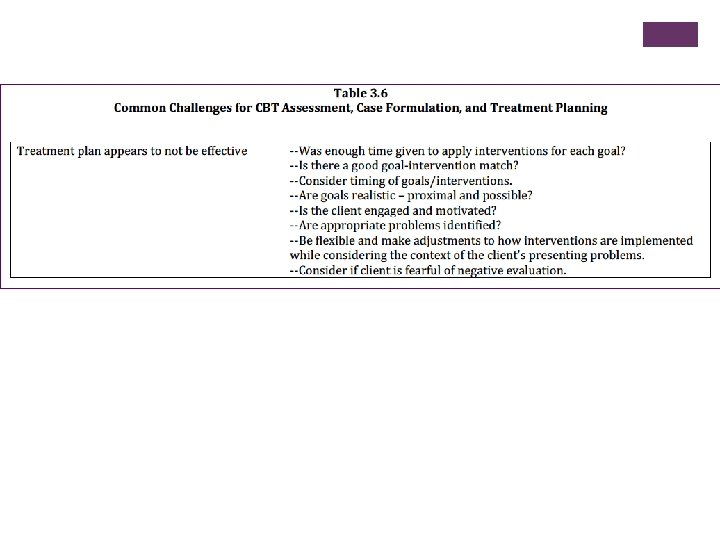
Common Challenges for CBT Assessment, Case + Formulation, and Treatment Planning
- Slides: 58