INFECTION INTRODUCTION Intact dentition periodontal structures and oral








 2. Lymphocytes monocytes found in blood")




 jugulodigastric group")










 •")



 POSTERIORS ( ROOT APEX BELOW")
 INFECTION")



 PRIME MUSCLES OF MASTICATION INFECTION TRISMUS ( USUALLY BECAUSE OF IMPACTED")

 ( DUMB-BELL")


 MEDIASTINITIS")
")
 swelling in")
 CONTROL INFECTION MEDICALLY SURGICALLY (SYSTEMIC ANTIBIOTIC)( TUBE DRAIN")

 ANTI COAGULANT THERAPY (")










 WELL DEVELOPED PERIOSTIUM , THICK")




 TRAUMA (COMPOUND FRACTURES OF THE JAWS) SPACE INFECTIONS (PERITONSILLAR")
 STREPTOCOCCUS PYOGENE SPIROCHETES ESCHERICHIA COLI (gram -ve) Mixed infection")
 Parasthesia of the")
")
















 TRAUMA TO TISSUE FOLLOWING EXTRACTION ATROPHIC")

 MUCOSITIS DECREASED")


 DEBRIDEMENT WITH H 2 O 2")


- Slides: 91
```` INFECTION
INTRODUCTION • Intact dentition, periodontal structures and oral mucous membrane constitutes the first line of resistance within the oral cavity against the invasion of microorganisms once it begins to dominate over the host response infection sets in. • They are classified into 1. acute – rapid onset. 2. chornic – prolonged duration.
FACTORS INFLUENCING THE SPREAD OF INFECTION 1. State of the oral microorganism. 2. Host & its environment. 3. Disturbance to the delicate balance between the oral micro flora and a host resistance. 4. Anatomical consideration.
State of the microorganism 1. Change in the oral environment: Results in the multiplication of microorganism in large nos. which may resist the virulence factors. 2. Virulence: Refers the quality of the microbes that is harmful to the host. Becomes cumulative effects of the parasites physiological & metabolic functions that favors the survival, multiply, growth & pathological changes in the host tissues.
Contd… 3. Mediators: Release toxins like fibrolysis, hyaluronidase which may aid in localizing the infection & formation of pus like coagulant. Gram +ve like coli & pseudomonas complicate the defense mechanism.
HOST & ITS ENVIORNMENT • Resistance varies between Ø Individuals. Ø Time in the some Individuals. Ø Age. Ø Sex. Ø Debilitating conditions (diabetes, malnutrition, chronic nephritis, hepatitis, aids & immunity status of the host) is directly proportional to onset & spread of infection.
Contd… The reserve resistance factors of the host can be consider under • Local defense: integrity of the primary line of defense like intact teeth, perio. Structures & oral mucosa in the salivary environment with efficient drainage system. Any alteration leads to penetration of microbes across the primary barrier. • Humoral & cellular component: components of humoral defence: * The complement system. * immunogloglobin.
Contd… • Hormonal defect is also called antigen-antibody reaction. • Important benefits derived by body are. vchemo taxis (mobilize polymorphs to the zone of infection) v. Bacteriolytic activity (control of the microbial multiplication) v. Phagocytosis(engulf the foreign body & digest) v. Neutralization of toxins. v. Activation of the complement. • The immunoglobins enhance the phagocytes by coating the bacteria, enhance the polymorphs to engulf more effectively & destroy them- ‘opsonization’
MAIN CELLULAR COMPONENTS OF DEFENSE 1. polymorphs (phagocytes) 2. Lymphocytes monocytes found in blood streams take over phagocytosis in late stage. similar cells derived from tissues are known as macrophages. polymorphs predominant in acute phase. monocytes & macrophages predominant in chronic phase. lymphocytes coordinates with monocytes during chronic stage.
Contd… Two types lymphocytes 1. B- lymphocytes. 2. T-lymphocytes. These have important function in resistance to infection, they differ in their location & certain function • Both regulate the action of phagocytosis. • Interferon enhance the lysis of bacteria by phagocytosis. • Macrophage inhibiting factors restrict the macrophages from moving away from the site on infection. • T-cells secrete mitogenic which stimulates B-cells, so that antibody response to antigenic stimulations occurs.
ANATOMICAL FACTORS. – Tissues of the head & neck are invested in facial planes separated by loose connective tissue. – Facial planes tends to localize the infection within their limits. – These planes communicate with each other – First barrier to infection from bone is the periosteum. – Pus traces along the least resistance & penetrate the various facial planes, blood vessels & lymphatics.
PRINCIPLES RELEVANT TO SPREAD OF INFECTION • Spread of infection within the dental structures: dental caries least resistance pulp inflammatory changes in pulp periapical tissue multiplication of micro. beyond periapical region
Spread into bones • Pathway: periapical region alveolar bone similar to pulp central marrow space cortical plate perialveolar soft tissue muscle plane
Contd… • Maxillary posterior tooth: maxillary sinus involved lymphatic channel (submandibular node) jugulodigastric group of lymph node venous channel venous drainage blocked
DIAGNOSTIC IMAGES OF MAXILLOFACIAL INFECTION 1. 2. 3. 4. 5. Plain film examination Computed tomography Magnetic resonance imaging Nuclear medicine Ultrography
PARANASAL SINUS PATHOLOGY Divided into two categories 1. Sinusitis a. infectious b. non-infectious 2. Granulamatous disorders
Sinusitis Acute infectious sinusitis : • Upper respiratory tract infection • Occurs after trauma • Excessive dryness • Allergic edema with occlusion of draining ostia • Nasal obstruction • Introduction of foreign bodies
Acute non infectious sinusitis • Allergic rhinitis • Allergic sinusitis - Acute sinusitis (periosteum become hyperplastic and grossly oedematous) - Chronic sinusitis (long duration of acute sinusitis, hypersecretion present)
Complications of sinusitis Divided under two categories one those limited to the sinus and those involving adjacent structures. First group: • Hypertrophic polyps • Mucous retention cyst (blockage of seromucous gland followed by cystic expansion) • Mucocele (blockage of draining ostia followed by continous secretion of fluid in obstructed sinus)
Contd… Second group: I. Includes number of inflammatory. Nasal , . Orbital and. Intracranial lesions. Or II. Osteomyelitis of sinus wall
Granulamatous disease 1. 2. 3. 4. 5. Affects nose and paranasal sinuses Heterogeneous group of pathological entities. Formation of soft tissue granulomata. Often indistinguishable from neoplastic process. Involving no of infectious disease -TB -leprosy -syphilis -yas -autoimmune disease wegeners granulomatosis idiopathic midline granuloma sarcoidosis foreign
Paediatric maxillofacial infection I. Tonsillar & peritonsillar infection Causes: • Infection • Adenoid hypertropy • Tonsillar hypertropy • Allergic reaction • Neoplasm Treatment: • Adenoidectomy • Tonsillectomy
Contd… II. Epiglottitis: • Acute bacterial inflammation or infection. • Caused by H. influenzae. Clinical features: • • • Severe pharyngitis High fever Inability to handle saliva Dysphagia Upper airway obstruction “Thumb sign” (thumb like epiglottis)
Contd… III. Croup: • As opposed to epiglottis, croup or laryngotracheobronchitis. • It is an viral infection caused by respiratory syncytial virus or para influenza. • Characterized by -inspiratory stridor. -hoarseness. -distinctive barking cough. -church steeple (steeple sign). or wine bottle (bottle sign). [due to sub-epiglottic narrowing because of mucosal or sub-mucosal edema].
COMMON MUSCLES INFLUENCING THE SPREAD OF INFECTION (Odontogenic Head and Neck infections ) • BUCCINATOR • MYLOHYOID • MUSCLES OF MASTICATION
POTENTIAL SPACES AND ITS ANATOMICAL IMPORTANCE MAXILLARY SPACES • Infra temporal • Parotid • Temporal • Buccal MANDIBULAR SPACES PHARYNGEAL SPACES • Sub mental • Sub mandibular • Sub masseteric • Sub lingual • Buccal
BUCCINATOR AND ODONTOGENIC INFECTION IN MAXILLA ABOVE THE ATTACHMENT ROOT APEX BELOW EXTRA ORAL THE ATTACHMENT INTRA ORAL SWELLING ( IN MANDIBLE IT IS VICE-VERSA)
MYLOHYOID AND ODONTOGENIC INFECTIONS ANTERIORS (ROOT APEX ABOVE ) POSTERIORS ( ROOT APEX BELOW ) M INTRA ORAL (FLOOR OF THE MOUTH ) EXTRA ORAL ( SUB MANDIBULAR )
SUB MASSETERIC SPACE 3 - LAYERS ( SUPERFICIAL , MIDDLE, AND DEEP ) INFECTION SPREADS IN BETWEEN THESE MASSETER AND ODONTOGENIC LAYERS INFECTION SWELLING LESS , PAIN MORE (INFECTION IS USUALLY CAUSED BY THE IMPACTED MANDIBULAR 3 RD MOLARS , ANY PULPALLY OR PERIODONTALLY INVOLVED MOLARS )
THE HIGH WAYS TO DANGER
PTERYGOID SPACE (PTERYGO-MANDIBULAR) PRIME MUSCLES OF MASTICATION INFECTION TRISMUS ( USUALLY BECAUSE OF IMPACTED TOOTH AND CONTAMINATED INJECTION INTO THE SPACE )
THE HIGH WAYS TO DANGER
TEMPORAL SPACE (SUPERFICIAL TEMPORAL AND DEEP TEMPORAL SPACE WITH BUCCAL SPACE ) ( DUMB-BELL SHAPED SWELLING ( TEMPORALIS FASCIA IS ATTACHED TO THE ZYGOMATIC ARCH) TRISMUS (USUALLY THROUGH PSA NERVE BLOCKS , INF FROM MAXILLARY MOLARS, SPREAD OF INFECTION FROM OTHER SPACES )
COMMON TREATMENT IN SPACE INFECTION * * * * EMPIRICAL ANTIBIOTIC THERAPY INCISION AND DRAINAGE CULTURE AND SENSITIVITY APPROPRIATE ANTIBIOTIC THERAPY REMOVAL OF THE CAUSE ( teeth if odontogenic ) SUPPORTIVE THERAPY PHYSIOTHERAPY (to improve mouth opening)
HIGH WAY TO DANGER • PTERYGOID PLEXUS • LINCOLN’S HIGH WAY • MULTI SPACE INFECTIONS
THE DANGER ZONES CAVERNOUS SINUS THROMBOSIS LUDWIG’S ANGINA (MULTI SPACE INFECTION) MEDIASTINITIS
ROOT CAUSE FOR THE DANGER BRAIN INFECTION RESPIRATORY OBSTRUCTION DESCENDING NECK INFECTION (MEDIASTINITIS, PERICARDITIS)
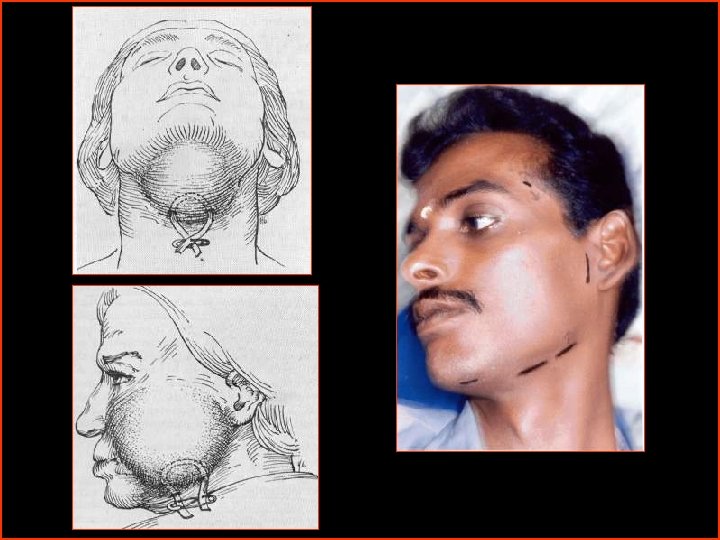
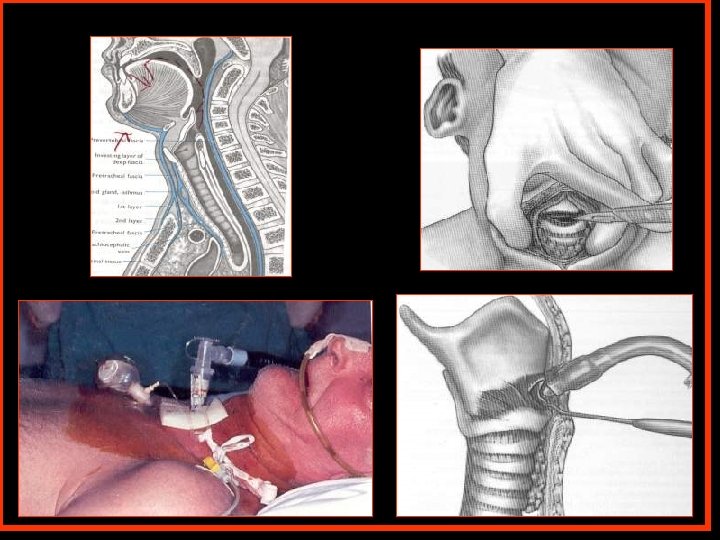
LUDWIGS ANGINA ( SUB LINGUAL, SUB MENTAL AND SUB MANDIBULAR SPACE ) swelling in the floor of the mouth lifting the tongue obstructing the air way creating an emergency situation
LUDWIG’S ANGINA MAINTAIN AIR WAY (TRACHEOSTOMY) CONTROL INFECTION MEDICALLY SURGICALLY (SYSTEMIC ANTIBIOTIC)( TUBE DRAIN )
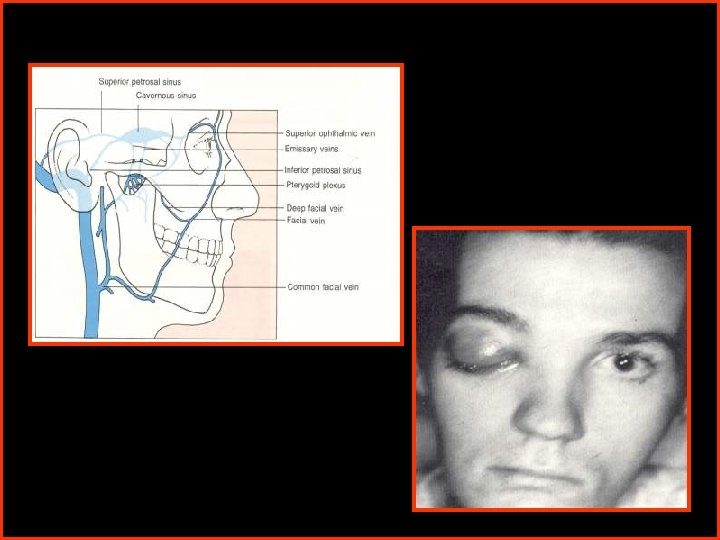
Cavernous sinus Thrombosis Pterygoid plexus Infra orbital fissure Terminal part of the inferior ophthalmic vein superior orbital fissure cavernous sinus ( THROMBOSIS)
MANAGEMENT ANTIBIOTIC CROSSING BLOOD BRAIN BARRIER ( CHLORAMPHENICOL. CIPROFLOXACIN ETC…) ANTI COAGULANT THERAPY ( TO PREVENT VENOUS THROMBOSIS )
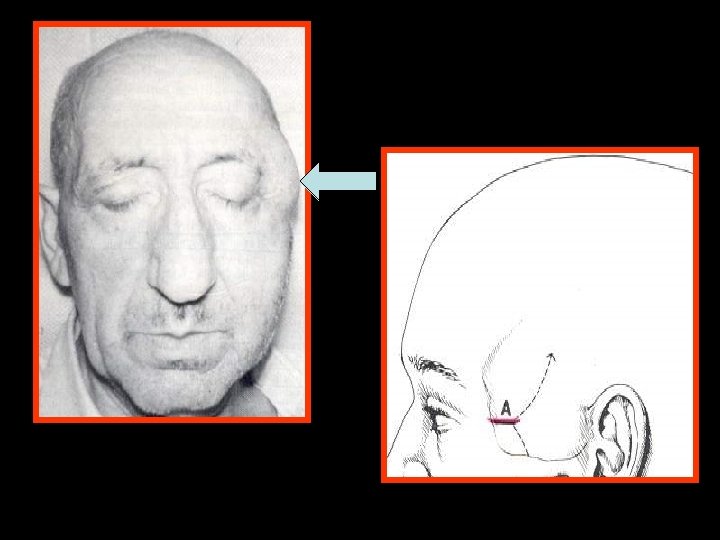
RETRO PHARYNGEAL SPACE DANGER SPACE ( SPACE BETWEEN ALAR AND THE PRE VERTEBRAL LAYER OF THE DEEP CERVICAL FASCIA ) MEDIASTINITIS / CAROTID SHEATH INFECTION (FATAL)
RETROPHARYNGEAL SPACE AND CAROTID SHEATH INFECTION MANAGEMENT INCISION AND DRAINAGE ( ALONG THE ANT BORDER OF THE STERNOCLEIDOMASTOID MUSCLE AT THE LEVEL OF THE HYOID BONE AND MIDDLE THIRD RESPECTIVELY )
DESCENDING NECK INFECTION SUPERFICIAL DEEP ACUTE NECROTISING FASCITIS MEDIASTINITIS ( MAL NOURISHED AND IMMUNO- PERICARDITIS COMPROMISED PATIENTS ) (STRIDOR-FATAL)
MANAGEMENT OF DESCENDING NECK INFECTION ACUTE NECROTISING FASCITIS DEEP CONTROL INFECTION APPROPRIATE SYSTEMIC ANTI BIOTICS DEBRIDEMENT , LOCAL ANTIBIOTIC DRESSING , RECONSTRUCTION OF THE NECROSED SKIN WITH GRAFT OR FLAP
MANAGEMENT OF INFECTION
PRINCIPLES OF INCISION AND DRAINAGE • INCISE IN HEALTHY SKIN AND MUCOSA • INCISION PLACED T THE SITE OF MAXIMUM FLUCTUATION • PLACE THE INCISION IN AN ESTHETICALLY ACCEPTABLE AREA • INCISION TO BE PLACED SUCH THAT IT SHOULD ENCOURAGE DRAINAGE BY GRAVITY • DISSECT BLUNTLY WITH A CLOSED SURGICAL CLAMP OR FINGER AND EXPLORE ALL THE PORTIONS OF THE ABSCESS CAVITY, SO THAT PUS ARE DISTURBED AND EXCAVATED.
CONTD… • EXTEND THE DISSECTION TO THE ROOT OF THE TEETH RESPONSIBLE FOR INFECTION • PLACE A DRAIN AND STABILIZE WITH SUTURE • CONSIDER THE USE OF THROUGH AND THROUGH DRAINS IN BILATERAL SUBMANDIBULAR SPACE INFECTION • REMOVE THE DRAIN AS SOON AS POSSIBLE (48 HOURS) • WOUND DEBRIDEMENT SHOULD BE DONE PERIODICALLY
ANTIBIOTIC THERAPY • PRINCIPLE FOR CHOOSING APPROPRIATE ANTIBIOTIC – – – IDENTIFICATION OF CAUSATIVE ORGANISM DETERMINATION OF ANTBIOTIC SENSITIVITY USE OF SPECIFIC NARROW SPECTRUM ANTIBIOTIC USE OF LEAST TOXIC ANTIBIOTIC PATIENT DRUG HISTORY USE OF BACTERIOCIDAL RATHER THAN BACTERIOSTATIC DRUG – USE OF ANTIBIOTIC – PROVEN HISTORY OF SUCCESS – COST OF ANTIBIOTIC – ENCOURAGE PATIENT COMPLAINTS
PRINCIPLE OF ANTIBIOTIC ADMINISTRATION • • • PROPER DOSAGE PROPER TIME INTERVAL PROPER ROOT OF ADMINISTRATION COMBINATION ANTIBIOTIC THERAPY PATIENT MONITORING – RESPONSE TO TREATMENT – DEVELOPMENT OF ADVERSE REACTION – SUPERINFECTION AND RECURRENT INFECTION
THERAPEUTIC USE OF ANTIBIOTIC IN MAXILLOFACIAL INFECTION • ACUTE DENTOALVEOLAR CELLULITIS AND ABSCESS - PENCILLLIN IS THE DRUG OF CHOICE • ACUTE PERICORONITIS - PENCILLLIN IS THE DRUG OF CHOICE • OSTEOMYELITIS - CULTURE SENSITIVITY - ANTIBIOTIC THERAPY IS FOR LONGER PERIOD • INFECTED SOFT TISSUE WOUNDS - WOUND DEBRIDEMENT WITH TOPICAL ANTIBIOTIC - AMOXYCILLIN WITH CLAVULANIC ACID - METRONIDAZOLE FOR ANAEROBIC INFECTION
OSTEOMYELITIS LIMITED MEDULLARY BONE THIN CORTEX ( MAXILLA ) WELL DEVELOPED PERIOSTIUM , THICK CORTEX AND EXTENSIVE SPONGIOSA (MANDIBLE ) PERIOSTITIS OSTEOMYLITIS
PERIOSTITIS ACUTE Exudates separates the periostium over an infected tooth Usually localized but it may spread to involve a large area CHRONIC ( GARRE S OSTEOMYLITIS , PEROSTITIS OSSIFICANS )
OSTEITIS ACUTE – SUPPURATIVE DENTO ALVEOLAR ABSCESS CHRONIC – SCLEROSING CONDENSING Well circumscribed osteolytic area with out a defined cortical border (STIMULATES BONE FORMATION INSTEAD OF DESTROYING BONE Can be totally radio opaque Decreases blood supply completely Induces pressure on the nerve and causes neuralgia )
OSTEOMYLITIS EXTENSIVE INFLAMATION OF THE BONE INVOLVING CORTICAL BONE , MARROW , AND THE PERIOSTIUM ACUTE Immediate onset SUBACUTE Chronic with acute symptoms CHRONIC
CLASSIFICATION SUPPURATIVE ACUTE CHRONIC NON SUPPURATIVE FOCAL SCLEROSING DIFFUSE SCLEROSING OSTEOMYLITIS ASSOCIATED WITH SYSTEMIC DISEASES TB, ACTINOMYCOSIS, SYPHILIS
ETIOLOGY ODONTOGENIC INFECTION (COMMON ) TRAUMA (COMPOUND FRACTURES OF THE JAWS) SPACE INFECTIONS (PERITONSILLAR ABSCESS ) FURUNCULOSIS (OTHER SKIN INFECTON ) HEMATOGENOUS SPREAD (RARE)
MICROBIOLOGY STAPHYLOCOCUS AUREUS (Common) STREPTOCOCCUS PYOGENE SPIROCHETES ESCHERICHIA COLI (gram -ve) Mixed infection
Acute Osteomylitis – Clinical features Local painful tooth (if Odontogenic ) Parasthesia of the lip (mandible ) Swelling in the effected area Difficulty in mouth opening General raise In temperature Rapid pulse & respiration Nausea & vomiting Dehydration, acidosis, albuminuria leukocytosis
Radiographic Features Enlargement of the marrow space Sequestrum (Dead bone surrounded by osteolytic channels) Involucrum (Reactive bone formation)
SCINTIGRAPHY – BONE SCAN IN EARLY DETECTION OF OSTEOMYLITIS
CHRONIC OSTEOMYLITIS CLINICAL FEATURE PAIN IN THE EFFECTED TOOTH SWELLING SINUS DISCHARGE ( EXTRA ORAL ) LESS SYSTEMIC SYMPTOMS DIFFICULTY IN MOUTH OPENING
RADIOLOGICAL FEATURE CHRONIC OSTEOMYLITIS MORE OF RADIO OPAQUE OR MIXED RADIO OPAQUE&RADIOLUCENT (CLASSICAL MOTH - EATTEN APPEARANCE)
PROTOCOL OF MANAGEMENT EMPERICAL ANTIBIOTIC CONTROL OF TOXIC SYMPTOMS INCISION & DRAINAGE CULTURE & SENSITIVITY APPROPRIATE ANTIBIOTICS REMOVAL OF THE CAUSE LATERAL TRIPHINATION CURRETAGE SEQUESTRECTOMY SAUCERIZATION DECORTICATION SEGMENTAL RESSECTION HBO
I&D ONLY IF IT IS FLUCTUENT SEND FOR CULTURE AND SENSITIVITY
SAUCERIZATION CREATES A UNIFORM BED HELPS IN COMPLETE DRAINAGE IMPROVE THE BLOOD SUPPLY
DECORTICATION IMPROVES BLOOD SUPPLY TO THE BONE
Antibiotic irrigation
SINUS DISCHARGE – SINUS EXCISION AND REPAIR
OSTEOMYELITIS IN CHILDRENS COMPLICATED BY PRESENCE OF TOOTH GERM IN CONDYLE MAY LEAD TO TMJ ANKYLOSIS AND SECONDARY FACIAL DEFORMITY
GARRE S OSTEOMYLITIS NON SUPPURATIVE TYPE CARLE GARRE 1893 PELL 1955 - IN MANDIBLE CHILDRENS AND YOUNG ADULT GENERALLY IN THE MANDIBLE PHERIPHERAL SUB PERIOSTEAL BONE DEPOTISION DUE TO MILD IRRITATION & INFECTION RADIOGRAPHICALLY - OCCLUSAL VIEW - CORTICAL THICKENING DD- INFANTILE CORTICAL HYPEROSTOSIS (CAFFEY’S DISEASES ) REMOVE THE CAUSE - WAIT & WATCH OCCATIONALLY - RECONTOURING IS PERFORMED
PERIOSTITIS THICKENING OF THE OUTER CORTEX REACTIVE BONE FORMATION
HYPER BARIC OXYGEN ADJUVENT THERAPY 100% OXYGEN UNDER PRESSURE TO THE CHAMBER – DIVE HYPOXIC HYPOCELLULAR HYPOVASCULARITY taken care by HBO
90 MTS DIVE – IN MONO PLACE CHAMBER
OSTEORADIONECROSIS POTENTIAL SEQUELAE FOLLOWING IRRADIATION OF ORAL CAVITY FOR TREATING MALIGNANCY RESULTING IN DEGENERATIVE BONE CHANGES
PATHOGENESIS IRRADIATION FIBROSIS CONSTRICTION OF BLOOD VESSELS DECREASED SALIVARY FLOW POOR ORAL HYGIENE DEVELOPMENT OF DENTAL CARIES
CONTD … DENTAL CARIES SPREAD OF INFECTION (OR) TRAUMA TO TISSUE FOLLOWING EXTRACTION ATROPHIC CHANGES ASEPTIC OSTEORADIONECROSIS OF THE BONE SUPERADDED SEPSIS OSTEOCLASTS) (OSTEOBLASTS ARE MORE RADIOSENSITIVE THAN OSTEORADIONECROSIS
OSTEORADIONECROSIS complication after irradiation IRRADIATION TRAUMA INFECTION
CLINICAL FEATURE PAIN & SWELLING RADIATION CARIES (DEMINERALIZATION OF THE TOOTH STRUCTURES) MUCOSITIS DECREASED SALIVARY SECREATIONS SEQUESTRATION OF THE BONE CHRONIC SINUS DISCHARGE SKIN INFECTION
PREVENTION PREPARE THE ORAL CAVITY FOR IRRADIATION MAINTAIN GOOD ORAL HYGEINE EXTRACT ALL INFECTED AND NON VITAL TOOTH EXTRACT PERIODONTALLY WEEK TOOTH TOTAL EXTRACTION CAN BE PERFORMED IN CASE OF HEAVY IRRADIATION PRE & POST IRRADIATION ANTI BIOTICS FLOURIDE THERAPY TO PREVENT IRRADIATION CARIES SUFFICIENT TIME FORIRRADIATION AFTER EXTRACTION
PREVENTION IS THE CURE FOR ORN
MANAGEMENT OF ORN PAR ENTRAL ANTIBIOTICS ( FLAGYL) DEBRIDEMENT WITH H 2 O 2 ( ANTIBIOTICS ) ANTIBIOTIC DRESSING HBO SURGICAL RESECTION OF THE AFFECTED PART
RESECTION & RECONTRUCTION RIM RESECTION / SEGMENTAL INTRA ORAL / EXTRA ORAL LA / GA
THANK U • THAN