Tubulointerstitial disease Sangho Lee Dept of Nephrology Kyunghee

Tubulointerstitial disease Sangho Lee Dept. of Nephrology, Kyunghee University
, Cephalosporins, Cipro •")
Acute Interstitial Nephritis 70% Drug hypersensitivity • 30% Antibiotics: PCNs (Methicillin), Cephalosporins, Cipro • Sulfa drugs • NSAIDs • Allopurinol. . . 15% Infection • Strep, Legionella, CMV, other bact/viruses 8% Idiopathic 6% Autoimmune Dz (Sarcoidosis, Tubulointerstitial nephritis/Uveitis)

Drug Causes of AIN Antibiotics Cephalosporins, Ciprofloxacin, Ethambutol, Isoniazid, Macrolides, Penicillins, Rifampin, Sulfonamides, Tetracycline, Vancomycin NSAIDs Almost all agents, including selective COX-2 inhibitors Diuretics Furosemide, Thiazides, Triamterene Miscellaneous Acyclovir, Allopurinol, Amlodipine, Azathioprine, Captopril, Carbamazepine, Clofibrate, Cocaine, Diltiazem, Famotidine, Indinavir, Mesalazine, Omeprazole, Phenteramine, Phenytoin, Pranlukast, Propylthioruacil, Quinine, Ranitidine

AIN from Drugs Renal damage is NOT dose-dependent May take weeks after initial exposure to drug • More common is seen several months to a year after use But as early as 1 week after medication is begun • Fever (27%) • Serum Eosinophilia (23%) • Maculopapular rash (15%) • Bland sediment or WBCs, RBCs, non-nephrotic proteinuria • WBC Casts • Urine eosinophils on Wright’s or Hansel’s Stain – Also see urine eos in RPGN, renal atheroemboli – Leukocytoclastic vasculitis
 NSAIDs-induced ARF + Minimal change disease 2)")
Acute interstitial nephritis with nephrotic syndrome 1) NSAIDs-induced ARF + Minimal change disease 2) NSAIDs Ampicilin Rifampin Interferon ※ Full picture of an allergic reaction (fever, rash, eosinophilia, eosinophiliuria) was typically absent
 2. acute tubulointerstitial nephritis 3. interstitial")
NSAIDs and Kidney diseases 1. Hemodynamic ARF (vasoconstriction) 2. acute tubulointerstitial nephritis 3. interstitial nephritis with minimal-change disease 4. chronic tubulointerstitial disease 5. Renal papillary necrosis 6. Electrolyte abnormalities

Lab findings of AIN • Acute rise in plasma creatinine concentration • Eosinophilia and eosinophiluria • Urine sediment: WBC, RBC, white cell casts • Proteinuria (< 1 g/day) • Signs of tubulointerstitial damage

Renal biopsy in AIN Indications • Uncertainty of diagnosis • Advanced renal failure • Lack of spontaneous recovery following removal of offending drug

Treatment of AIN • Discontinuation of offending agent • Corticosteroids § Prednisone 1 mg/kg to a max of 40 -60 mg x 1 -2 weeks §IV Methylprednisolone 0. 5 – 1 g/day x 3 days

Infectious Causes of AIN Bacterial Corynebacterium diphtheriae, legionella, staphylococci, streptococci, yersinia Viral CMV, EBV, HIV, HCV, HSV, hantaviruses, mumps, polyoma virus Other Leptospira, mycobacterium, mycoplasma, rickettsia, syphilis, toxoplasmosis

Infiltrative/Autoimmune Causes of AIN • Sarcoidosis • Sjogren’s Syndrome • Leukemia • Lymphoma • Systemic lupus erythematosus

Analgesic abuse nephropathy • chronic interstitial nephritis • Result from excessive consumption (Phenacetin & Aspirin) • Dose dependent (at least 1 kg) • Past : 1% to 3% of ESRD cases

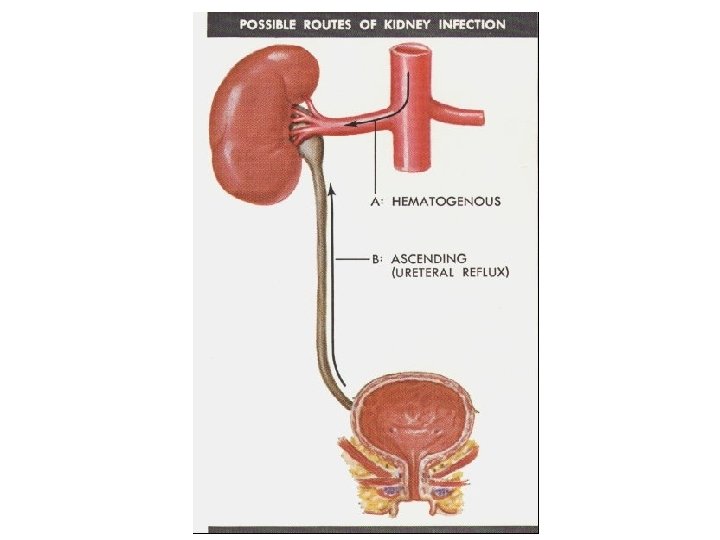
Bacterial infection • bacterial infection of the renal parenchyma causes interstitial nephritis • infection without anatomical abnormality seldom produces permanent damage • obstruction (stones, prostate etc) in combination with infection cause progressive disease • tuberculosis causes extensive destruction from granulomata, fibrosis and caseation

• The upper and lower poles with compound papilla in ascending infection • At first, interstitial edema and PMN infiltration, then formation of irregular abscesses and eventually scars • Risk factors: diabetes mellitus obstruction delayed antimicrobial therapy severe infection with ATN reflux nephropathy papillary necrosis

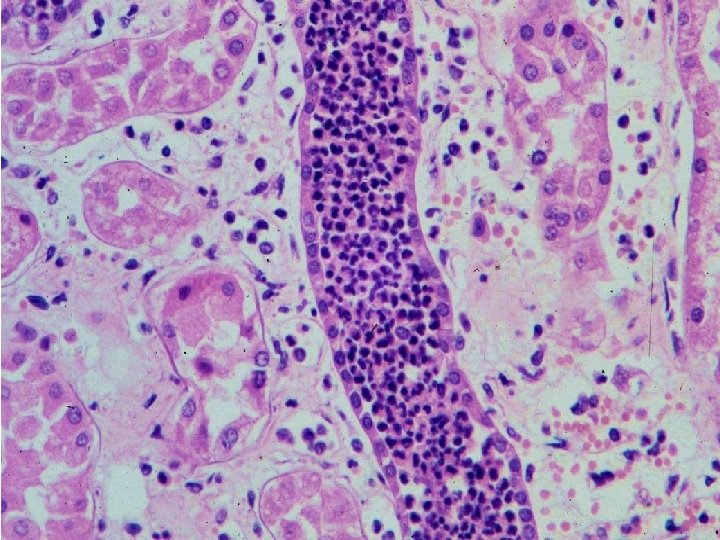
Acute pyelonephritis

Defenses against urinary tract infections • Emptying bladder • Washing action of micturition • Antibacterial properties of urothelium • Immunity

Etiology • Inflammation of the structures of the kidney: – the renal pelvis – renal tubules – interstitial tissue • Almost always caused by E. coli

Etiology • Usually seen in association with: – Pregnancy – diabetes mellitus – Polycystic – insult to the urinary tract from catheterization, infection, obstruction or trauma

What happens to the kidney? • The kidney becomes edematous and inflamed and the blood vessel are congested • The urine may be cloudy and contain pus, mucus and blood • Small abscesses may form in the kidney

Signs and Symptoms • acutely ill, fever, malaise and pain in the costovertebral angle (CVA) – CVA tenderness to percussion is a common finding • In the chronic phase the pt may show unremarkable symptoms such as nausea and general malaise
")
Costovertebral Angle (CVA)
 A clean-catch")
Diagnostic Tests • leukocytosis • WBC in uirne • Urine culture (+) A clean-catch or catheterized urinalysis with culture and sensitivity identifies the pathogen and determines appropriate antimicrobial therapy

Diagnostic Tests • US • IVP

Medical Management • Antibiotics • according to results of urinalysis culture and sensitivity

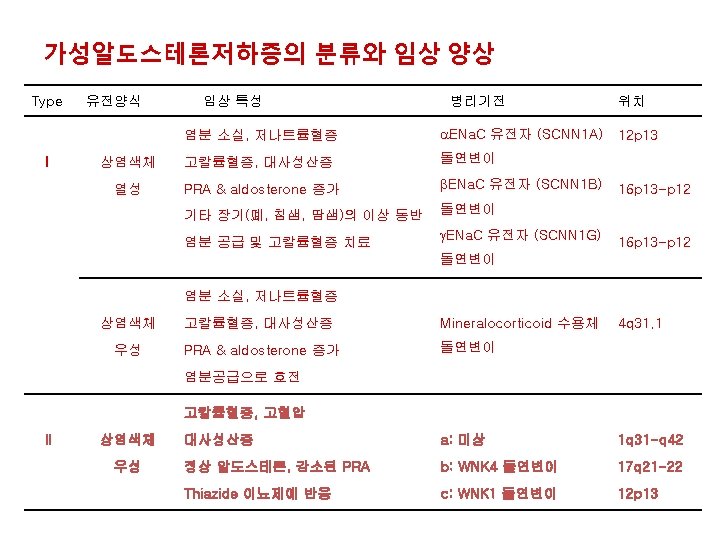
Tubular disorders in renal Na+ & K+ handling • Bartter’s syndrome • Gitelman’s syndrome • Liddle’s syndrome • Type I pseudohypoaldosteronism

Bartter’s syndrome - 1962 Bartter - hypokalemic, hypochloremic metabolic alkalosis in two children and a man - Other characteristics : urinary excretion of potassium and prostaglandins : normal or low BP despite increased PRA & high aldosterone : resistance to the pressor effects of exogenous angiotensin II : hyperplasia of the juxtaglomerular apparatus - In most pts, diagnosed in infancy, childhood, or early adolescence - no predilection with respect to race, ethnic group, or sex - sporadic Vs in families (AR)

Proposed primary defect of Bartter’s syndrome 1. juxtaglomerular hyperplasia 2. insensitivity to angiotensin II 3. overproduction of prostaglandins, kallikrein, and kinins 4. a defect in potassium transport resulting in excessive urinary potassium excretion 5. a defect in sodium chloride transport in the thick ascending limb of Henle's loop or the distal convoluted tubule

DDx for hypokalemia 1. Among the causes of hypokalemic metabolic alkalosis 2. absence of hypertension rules out primary mineralocorticoid excess 3. high urinary chloride rule out secondary hyperaldosteronism (due to extrarenal fluid loss)

Among the causes of hypokalemic metabolic alkalosis the absence of hypertension rules out primary mineralocorticoid excess the finding of high urinary chloride excretion rules out secondary hyperaldosteronism (vomiting) Bartter's syndrome Vs. long-term diuretic therapy furosemide
 KCNJ 1")
In mid 1990 s, NKCC 2 (15 q 15 -q 21. 1) KCNJ 1 (ROMK 1, 11 q 24) CLCNKB (1 p 36) Simon et al, 1996 Simon et al, 1997
 - 2 affected sisters, occasional mild episodes of")
Gitelman’s syndrome Gitelman et al. (1966) - 2 affected sisters, occasional mild episodes of muscle weakness - a variant of Bartter's syndrome - hypomagnesemia and hypocalciuria - subnormal natriuretic response to intravenous chlorothiazide - but a prompt natriuresis after the administration of furosemide Mutations : sodium–chloride transporter NCCT (? )

Mechanism of Gitelman’s syndrome Loss of function of this sodium–chloride transporter defective reabsorption of sodium chloride in the distal tubule increases solute delivery to the collecting tubule mild volume contraction and aldosterone-stimulated secretion of K+ & H+ mild hypokalemic metabolic alkalosis volume contraction, the stimulation of vasopressin and the renin–angiotensin–aldosterone axis, and the potassium depletion appear to be less marked than in Bartter's syndrome and are not sufficient to increase the production of renal and systemic prostaglandin E 2 substantially Urinary prostaglandin excretion remains normal in Gitelman's syndrome
 gene cloned in 1996 by Simon et al NCCT gene")
TSC (16 q 13) gene cloned in 1996 by Simon et al NCCT gene Simon et al, 1997

Comparison of clinical feaure between Bartter’s and Giteman’s syndorme Bartter’s syn Infancy/early childhood frequent present severe none Age of onset Symptoms Polyuria Severity of K+ depletion Dermatitis PRA & alosterone elevated Urine PGE 2 excretion increased JG hyperplasia present Urinary dilution impaired Mg wasting 20 -30% Calcium excretion hypercalciuric or normocalciuric Site of defect TAL Gitelman’s syn Adolescence/early adult occasional absent mild to moderate described elevated variable reports present impaired 100% of patients hypocalciuric distal tubule

Bartter’s syn Gitelman’s Site of defect Thick ascending loop distal tubule Molecular basis Na-K-2 Cl cotransporter Na-Cl cotransporter syn ROMK channel in TAL CLC-Kb channel in TAL Mutations in Genes NKCC 2 (15 q 15 -q 21. 1) KCNJ 1 (ROMK 1, 11 q 24) CLCNKB (1 p 36) TSC (16 q 13)

Monogenic diseases causing salt-sensitive hypertension or salt-losing syndrome 변이형 세뇨관질환 작용부위 표현형 기능 소실 Bartter syndrome Thick ascending limb Salt-resistant Gitelman syndrome Distal convoluted tubule Pseudohypoaldosteronism type I Distal CT, connecting tubule, collecting duct Pseudohypoaldosteronism type II Distal CT, connecting tubule, collecting duct Salt-sensitive Liddle syndrome Distal CT, connecting tubule, collecting duct hypertensive 기능항진 hypotensive

Liddle's and PHA-I mutations found in ENa. C. ▴, PHA-I mutation; ●, Liddle's mutation #, stop codon; ∗, frameshift.
 due to a primary")
Liddle Syndrome • Severe form of autosomal dominant salt-sensitive hypertension(early-onset) due to a primary increase in sodium balance. • Secondary hypokalemia, metabolic alkalosis • Specific mutations of the β or ν subunit of ENa. C which interferes ENa. C binding to ubiquitin ligases that normally downregulate channel activity by channel internalization and degradation.
- Slides: 43