Noninfectious Erythematous Papular and Squamous Diseases Dr Alireza








 Primigravid 3 th trimester Rash starts on")










 : Ø Granular deposition of C 3")



















 involvment as: marked")





 has role in the")


 mounds of parakeratosis with neutrophils at their")
 a) acanthosis with")



 Early pustular lesions spongiform macropustule in the upper epidermis parakeratosis and")

 Large plaque parapsoriasis and parapsoriasis variegata : early stages of cutaneous T-cell")
 The small plaque focal epidermal involvement e. g. slight spongiosis, exocytosis of lymphocytes,")


 The patches of the disseminated eruption ü superficial perivascular dermal")
 is suspected Cell-mediated immunity (may")
 nonpruritic, symmetrical eruption of")
 q superficial and mid-dermal perivascular infiltrate of lymphocytes and histiocytes")
 T-lymphocytes")
 mucocutaneous lymph node syndrome children under 5 years")

 sparse perivascular infiltrate of lymphocytes and histiocytes marked papillary dermal edema,")
 ü more")
 at the same time, skin lesions with clinical, histological,")


: Typical papules (a) compact orthokeratosis (b) wedge-shaped hypergranulosis (c) irregular acanthosis (d) vacuolar")












 Ø the basal keratinocytes with their desmosomes and hemidesmosomes, show degenerative")

 Ø fibrinogen deposition demonstrated as shaggy deposits at the")
 Ø deposition of Ig. M and/or Ig. A, Ig. G, and,")





















 that express CD 7")
- Slides: 115
Noninfectious Erythematous, Papular, and Squamous Diseases Dr. Alireza zeynadini Meymand Resident of Dermatology Kerman medical University of science
HISTOPATHOLOGY v. Acute Urticaria : Ø Interestitial edema Ø Dilated venules Ø Endothelial sowelling Ø Paucity of inflammatory cells
HISTOPATHOLOGY v. Chronic urticaria : Ø Interestitial edema Ø Perivascular & interestitial Mixed – cell infiltrtation Ø Lymphocytes , Eosinophils , Neutrophils (variable)
HISTOPATHOLOGY v. Angioedema : Ø Edema & infiltration into subcutaneous tissue v. Hereditory angioedema : Ø Subcutaneous & submucosal edema without infiltration of inflamatory cells
HISTOPATHOLOGY Urticarial vasculitis : Ø Infiltration around the walls of small blood vessels ( leuckocytoclysis ) Ø Low or no deposits of fibrin in vessel walls Ø Slight to moderate extravasation erythrocytes
PATHOGENESIS q Electron microscop : Degranulation mast cell & eosinophil § Chronic Urticaria : Ig. G cross link to alpha chain of receptor Ig. E RELEASE OF HISTAMIN Ø C 5 RELEASE O HISTAMIN Ø Chemotactic mediatores from mast cell induce Pselectin , Eelastin , ICAM 1 , VCAM 1 , Beta 2 integrin on leuckocytes
Hereditary Angioedema v Deficit in C 1 esteras inhibitor : activation C 1 v activation C 1 : activation C 2 & C 4 v activation C 2 & C 4 : generation of C 2 fragment + kinin like activity & finally increased vascular permeability
IF Urticarial vasculitis : circulating immune complex in ½ patients DIF : Strong granula deposits in dermoepidermel junction & perivascular areas Positive IF : in hypocomlementemic form Renal biopsy : GN
PRURITIC URTICARIAL PAPULES AND PLAQUES OF PREGNANCY(PUPPP) Primigravid 3 th trimester Rash starts on the abdomen Pruritic papules, erythematous, maybe vesicle Proximal part of the extremities Usually involutes after delivery Fetal : unaffected
HISTOPATHOLOGY PUPPP Superficial & mid-dermal perivascular lymphohistiocytic infiltration Eosinophil, neutrophil , edema of superficial dermis Focal spongiosis , parakeratosis , mild acanthosis
PATHOGENESIS v Correlation between PUPPP and increased weight and Twin/triple v positive PR (Progestron Receptor) by RT-PCR v Nonlesional epiderm : not PR positivity v Placenta expresses : paternal factor as cause of PUPPP v DIF : negative or non specific
ERYTHEMA ANNULARE CENTRIFUGUM Arcuate & polycyclic area of erythema 2 variant : superficial & deep Deep form : palpable erythema + central clearing + absence of surface changes Superficial form : trailing scale , delicate annular rim of scale May up to 10 cm and over a several weeks Mildly pruritic Trunk and proximal extremities Most resolve within 6 w May persist or recur for years
PHOTO
HISTOPATHOLOGY EAC q. Superficial : Ø superficial privascular tightly cuff lymphohitiocytositic infiltration Ø Endothelial cell swelling Ø Focal extravasatinon of RBC Ø Spongiosis Ø parakeratosis
HISTOPATHOLOGY q. Deep : Ø Superficial and deep perivascular tightly cuff lymphohistiocytic infiltration striking coat Sleeve like pattern
PATHOGENESIS q. Exactly not clear q. Associated with : Ø Occult infections, dermatophytosis, candidiasis, medications, r arely malignancy ( lymphoma) Ø Rash has poor response to topical steroids
Differential Diagnosis q. Secondary syphilis : Ø neumerous plasma cell & histiocytes Ø Intima & endothelial cells are swollen q. Tumid LE : Ø Increased deposits of connective tissue mucin
ERYTHEMA GYRATUM REPENS v. Very rare but highly characteristic v. Paraneoplastic syndrom, associated with internal malignancy(lung-bronchial, esophageal, breast) v. Eruption typically very pruritic, cocenteric & parallel bands of erythema & scale …. wood-grain pattern v. Trunk & extremities v. Rashes migrate rapidly : up to 1 cm per day v. Ichthiosis & palmar/plantar hyperkeratosis
Histopathology EGR v. Mild acanthosis, spongiosis, parakeratosis v. Superficial perivascular lymphohistiocytic infiltration include : eosinophils, neutrophils, melanophages
Pathogenesis EGR v. DIF In lamina densa(BMZ) : Ø Granular deposition of C 3 , C 4 , Ig. G Ø SO : IMMUNOGENIC BASIS
ERYTHEMA DYSCHROMICUM PERSTANS v. Synonym : Ashy dermatosis v. Extensive asymptomatic eruption v. Disseminated macules , red active border v. Coalescence : large patch with a polycyclic outline v. At first erythematous then blue – gray v. Trunk , arms , face
Histopathology EDP q. Early active stage : Ø Vacoular alteration of the basal layer Ø In papillary dermis : mild to mod. Perivascular infiltration of lymphocytes, histiocytes, melanophages Ø Exocytosis of lymphocytes into basal layer Ø Necrotic keratinocytes Ø Colloid bodies q. Late stage : Ø Aggregation of melanophages in the papillary dermis
Pathogenesis v. Many vacoules v. Widenig of intercellular spaces & retraction of desmosomes v. Discountinuing of subepidermal BM v. Melanophages in dermis v. Pigmentary incontinence & formation of colloid bodies (vacoular alteration)
Pathogenesis EDP v. DIF : Ø Ig. G on necrotic keratinocytes at dermo epidermal junction v. Immunohistochemical stain : Ø Tcells CD 4+ & CD 8+ Ø ICAM 1 & HLA-DR on basal layer Ø Activation AIM/CD 69 & CD 94
PRURIGO SIMPLEX v. Erythematous urticarial papules v. Symmetric distribution v. Trunk , extensor of extremities v. Middle age v. PH : DA or dermographism v. Similar to DH but no grouping of lesions
PHOTO
Histopathology PRURIGO SIMPLEX q. Early papules : Ø mild acanthosis , spongiosis with spongiotiv vesicles , parakeratosis Ø Perivascular lymphocytes infiltration Ø Eosinophils in some cases q. Excoriated papules : Ø Absence of epiderm with crust Ø Histologic change around hair follicles q DD : DH microabscesses of the tips of dermal papilla & neutrophils + eosinophils + nuclear dust
PRURIGO NODULARIS v A chronic dermatitis , discrete, raised, firm hyperkeratotic papulonodules v 5 – 12 mm or larger v Extensores of extremities v Intensly pruritic v Middle age v Women more v May coexist with LSC v Cause unknown but maybe : Ø Truma, insect bites, atopic background, metabolic or systemic diseases
PHOTO
Histopathology PRURIGO NODULARIS v Hyperkeratosis, acanthosis v Papillomatosis & irregular downward proliferation v Psudoepitheliomatosis hyperplasia v Lymphocytic infiltration & vertically collagen bondles in papillary dermis v Neural hyperplasia v Silver or cholinesterase stain : number of cutaneous nerve v langerhans cells v Enlarged dendritic mast cells
Pathogenesis q first theory : Ø Chronic truma by scratching neural proliferation q. Second theory : Ø dermal nerves extreme pruritis ü Over expression NGF & it’s receptpres ü Neural proliferation both axon & schwann cells
Pathogenesis q Demonestration of nerve fiber by immunostain for : Ø S – 100 Protein Ø Nerofilament Ø Myelin basic protein q Immunohistochemical : Ø Sensory nerves + sensory neuropeptides ü Meckel cells in basal layer ü DD : LSC , Kerathoacanthoma
PSORIASIS q divided to : A. Vulgaris B. Generalized pustular C. Localized pustular
Psoriasis Vulgaris Histopathology q. Early psoriasis : v Mounds of parakeratosis with neutrophils v thin granular layer v moderate acanthosis v focal spongiosis v increased mitotic figures v dilated blood vessels at the tip of the dermal papillae v Perivascular infiltrate of lymphocytes and a few neutrophils
Psoriasis Vulgaris Histopathology q well-developed plaque : velongated rete ridges vabsent granular layer v. Parakeratosis with neutrophils vdilated tortuous vessels in the dermal papillae v. Suprabasal mitoses vthin suprapapillary epidermal plates vpallor of the upper epidermis
Kogoj & Munro microabscess q neutrophilic collections : Ø within the parakeratotic cornified layer: Monro Ø within the spinous and granular layer : Kogoj
Section 7 part 2 R. Ahmadi
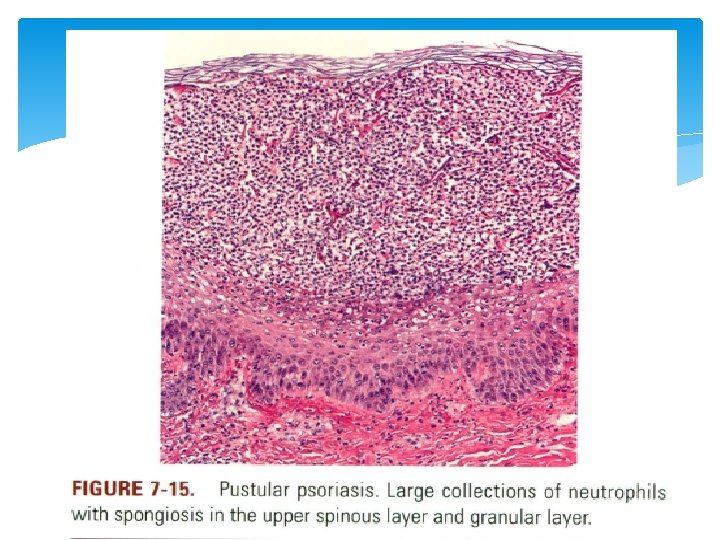
Generalized Pustular Psoriasis Histopathology: ü Spongiform pustule of kogoj: as a macropustule in all variants of GPP ( characteristic) ü 1 st : neutrophils migrate upper layer of epidermis Then aggregate in songlike network of degenerated & thin epidermal cells ü 2 nd : ↑ size of pustule then complete cytolysis of epidermal cell & finally large single cavity forms with thin epidermal cell at periphery ü Neutrophils move of cornified layer become pyknotic ( appearance of large munro abscess) ü Parakeratosis & elongation of rete ridges ( as seen in all forms) ü Upper dermis: lymphocytes & neutrophils infiltrates ü Oral lesios: the same as skin ü Healing stage: the same as ordinary psoriasis
Localized Pustular Psoriasis Histopathology: ü Histologic picture in localized pustular & localized annular pustular: the same as generalized pustular psoriasis ü Very early lesion: § 1 st : spongiosis + exocytosis of lymphocyets in lower epidermis ( tips of dermal papilla ) 2 nd ( maybe ) : intarepidermal vesicles contain lymphocytes inside & neutrophils in wall § 3 rd massive exocytosis of neutrophils penetrate wall of vesicule § § Acute form: leukocytoclastic vasculitis
ü localized acrodermatitis continua of Hallopeau: nail bed ( matrix occationally) involvment as: marked epithelial hyperplasia with variable numbers of spongiform pustules orthokeratosis with mounds of parakeratosis with neutrophils. ü pustulosis palmaris et plantaris: i. 1) fully developed large intraepidermal unilocular pustule ii. 2) many neutrophils inside pusule iii. 3) small spongiform pustules in epidermal wall of bigger pustule
Psoriasis and AIDS Histopathology: Most cases: the same as psoriasis Others: ü acanthosis without thinning of the suprapapillary epidermis ü slight spongiosis, rare necrotic keratinocyte ü a superficial perivascular infiltrate of lymphocytes and Histiocytes ü eosinophils may be present
Pathogenesis of Psoriasis Vulgaris complex interaction of: altered keratinocytic proliferation and differentiation, inflammation, and immune dysregulation Electron Microscopy: ü Relapse: early: 1. swelling and intercellular widening of endothelial cells 2. activated macrophages migrate into the lower epidermis 3. then lymphocytes and neutrophils are seen ü Ultrastructurally( well developed active lesion) a) tonofilaments are decreased b) size and number of keratohyaline granules are greatly reduced c) cornified cells possess thin tonofilaments and often retain organelles and a nucleus as parakeratotic cells
ü The intercellular spaces between all epidermal cells are widened due to deficiency in the glycoprotein-rich cell surface ü intercellular adhesion is limited to the desmosomes ü increased rate of mitosis related parakeratosis spongiform pustule of Kogoj A)located in the uppermost portion of the spinous and granular layers B) multilocular & composed of degenerated and flattened keratinocytes & neutrophils Capillary a) wider lumen b) bridged fenestrations and gaps c) edematous areas in the cytoplasm of endothelial cells pericytes myocytes d) extravasation of RBC , inflamatory cells e) thickened multilayered basement membrane
Epidermal Cell-Cycle Kinetics ü rate of epidermal cell replication is markedly accelerated in active lesions ü The mitotic activity correlate with the degree of parakeratosis ( vary in even in same lesion) ü alternating layers of orthokeratosis and parakeratosis (epidermal growth activity fluctuates in the lesions ) ü germinative cell cycle is shortened from 311 to 36 hours (keratinocytes proliferate 8 fold faster than nl) ü aberrant expression of apoptosis-related molecules representing suppressed apoptotic process ( maybe related to ↑ proliferation in psoriasis)
Keratinocyte Differentiation In psoriatic skin: ü basal keratinocytes continue to express K 5/K 14 ü keratins K 1/K 10 are replaced by hyperproliferation-associated keratins K 6 and K 16 ü involucrin is expressed prematurely ü Keratin 17: in upper suprabasal keratinocytes ( normaly in deep outer root sheet) Immunopathology ü T cell mediated disorder ü CD 8+ T-lymphocytes dominant in the epidermis ( key event) (Nonlesional skin not show) ü clonal expansion of epidermal T-lymphocytes ü The activation of T-lymphocytes may be due to bacterial superantigens( such as group A beta-hemolytic streptococci)
ü Group A streptococcal-reactive CD 8+ ( CD 4 lesser) has role in the pathogenesis of both poststreptococcal guttate psoriasis and chronic plaque psoriasis üActivated CD 4+ T-lymphocytes produce: 1. interleukin-2 2. tumor necrosis factor-alpha (TNF) stimulate keratinocyte that cause interleukin-8 production then chemotaxsis of neutrophils & lymphocytes 3. gamma-interferon (CD 8+ also produce this) a) initiation of psoriatic lesions b) expression of ICAM-1 in keratinocytes then trafficking of lymphocytes into the epidermis c) IP-10 overexpression d) decreased responsiveness of keratinocytes to IFN may cause hyperproliferation of epidermal cells
Pathogenesis of Localized Pustular Psoriasis pustulosis palmaris et plantaris with psoriasis generally not related but 1) occurrence of psoriasis in patients with pustulosis palmaris et plantaris, reported in 19% to 48% of the patients 2) common presence of spongiform pustules in the walls of the pustules of pustulosis palmaris et plantaris 3) leukotactic factor identical to that noted in psoriasis found in pustulosis palmaris et plantaris
Pathogenesis of Psoriasis and AIDS ü Paradoxically, as T-helper lymphocyte counts decline, psoriatic lesions exacerbate ü preterminal stage dermatitis improves ( due to decreased local production of alpha-IFN ) ü IFN serum levels were much higher in HIV+ psoriatic patients than non psoriatc ü The immunodysregulation resulting from HIV infection may trigger psoriasis in those genetically predisposed by carrying HLA-Cw*0602 allele ü Human retrovirus-5 has been implicated in the pathogenesis of psoriatic arthropathy but not psoriasis ü cellular immune reactions involved in the pathogenesis of psoriasis may be similar in AIDS and non-AIDS patients
Differential Diagnosis of Psoriasis Key diagnosis (a) mounds of parakeratosis with neutrophils at their summits (Munro microabscesses) (b) spongiform micropustules of Kogoj in the uppermost layers of the spinous layer Helpful: Dilatation and tortuosity of capillaries in the papillae
chronic eczematous dermatitis (atopic dermatitis, nummular dermatitis, or allergic contact dermatitis) a) acanthosis with elongation of the rete ridges and parakeratosis = psoriasis b) elongation of rete ridges is uneven c) marked spongiosis and especially of coagulated serum are features speaking against psoriasis ( except volar type) a) Eosinophils (found in allergic contact dermatitis and mainly in HIV+ patients) are rarely seen in the psoriatic infiltrate
Lichen simplex chronicus v. s. fully developed psoriatic plaques I. prominent granular layer II. more irregular acanthosis, and fibrosis of the papillary dermis III. collagen bundles aligned perpendicularly to the skin surface Seborrheic dermatitis ( esp. overlap) Accentuated spongiosis, mounds of parakeratosis with neutrophils predominantly at the follicular ostia, and more irregular acanthosis Pityriasis rubra pilaris v. s. well developed lesions thick suprapapillary plates, broader and shorter ridges, preserved granular layer and alternating ortho and parakeratosis lacks Munro microabscesses and neutrophils in the infiltrate
pustular dermatophytosis, bacterial impetigo, pustular drug eruptions, and candidiasis ü PAS and Gram stains are useful to identify the infectious microorganisms ü aggregates of neutrophils with pyknotic nuclei within areas of parakeratosis may occur in conditions the same as psoriasis ü the Kogoj spongiform pustule the same psoriasis
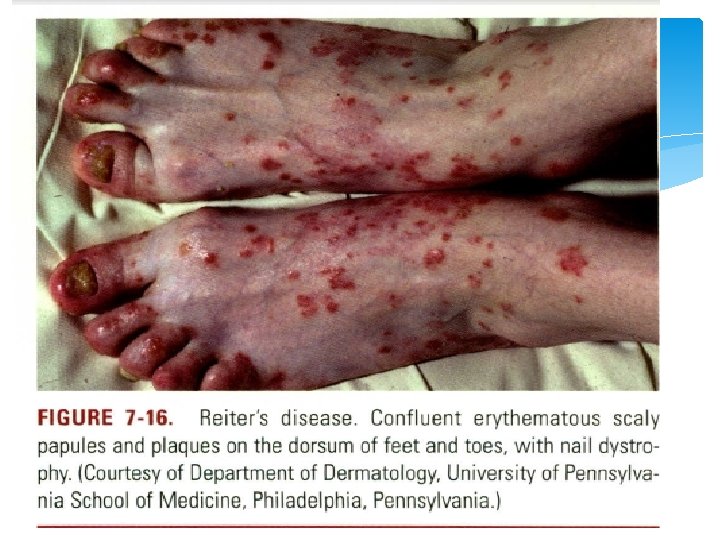
REITER'S DISEASE § triad of urethritis, arthritis, and conjunctivitis § Young men § a rule the arthritis occurs in attacks and is followed by recovery ( some cases maycause permanent damage to the affected joints) § Cutaneous lesions occur in about half of affected patients § predilection for i. glans penis (balanitis circinata), ii. the palms and soles (keratoderma blennorrhagicum): erythematous, mollusk-like plaques with central keratotic excrescences iii. the subungual areas; hyperkeratosis with opacification of the nail plate and eventual shedding of the nail plate may occur
Histopathology (REITER'S DISEASE) Early pustular lesions spongiform macropustule in the upper epidermis parakeratosis and elongation of the rete ridges Aged lesions The parakeratotic cornified layer thickened considerably with the pyknotic nuclei of neutrophils Old lesions ( resemble psoriasis) spongiform pustules are no longer seen acanthosis and orthokeratosis with only a few areas of parakeratosis
Pathogenesis ü urogenital or gastrointestinal infections such as Chlamydia trachomatis, Ureaplasma urealyticum, Shigella, Salmonella, Campylobacter, Cyclospora, and Yersinia species ü Chlamydia trachomatis has been cultured from urethral samples in nearly half of the patients ü Eighty percent of Reiter's disease patients are HLA-B 27 positive Differential Diagnosis Ø The early spongiform pustule v. s. pustular psoriasis Ø Slightly older lesions differ from psoriasis by markedly thickened cornified layer
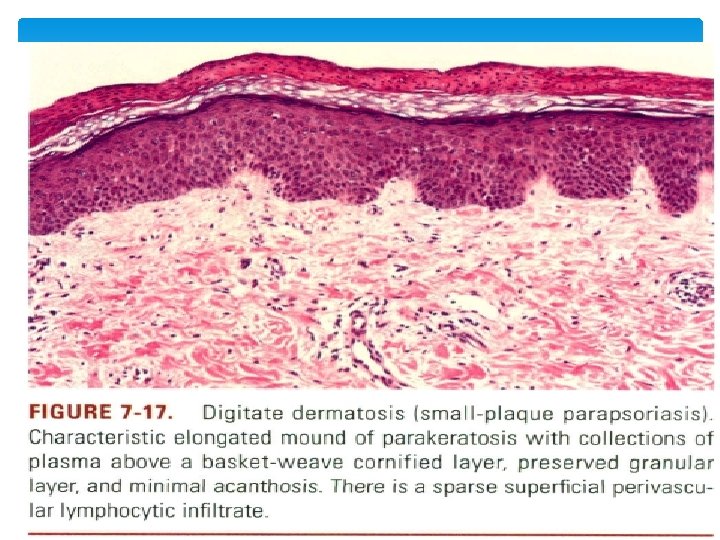
PARAPSORIASIS 1) Large plaque parapsoriasis and parapsoriasis variegata : early stages of cutaneous T-cell lymphoma 2) The small plaque parapsoriasis (digitate dermatosis ) Pink to yellow, slightly scaly, oval or elongated, often finger print-like patches 1 to 5 cm in diameter, the plaques are symmetrically distributed over the trunk and the proximal portions of the extremities following the tension lines of the skin The eruption is usually asymptomatic, has a chronic course, and tends to persist
Histopathology(PARAPSORIASIS) The small plaque focal epidermal involvement e. g. slight spongiosis, exocytosis of lymphocytes, mild acanthosis, and parakeratosis characteristic finding: Elongated mounds of parakeratosis with collections of plasma above a basket-weave cornified layer large plaque papillary dermis: superficial perivascular lymphocytic infiltrate Differentiation between small & large plaque is difficult Pathogenesis CD 4+ T-lymphocytes with a small proportion of the CD 8+
Relationship to Lymphoma small plaque parapsoriasis: benign disorder without the potential of transformation into mycosis fungoides but some cases there is a dominant clonal rearrangement of the infiltrating T-lymphocytes So disorder is not related to mycosis fungoides where there is clonal T-cell proliferation in both peripheral blood and skin
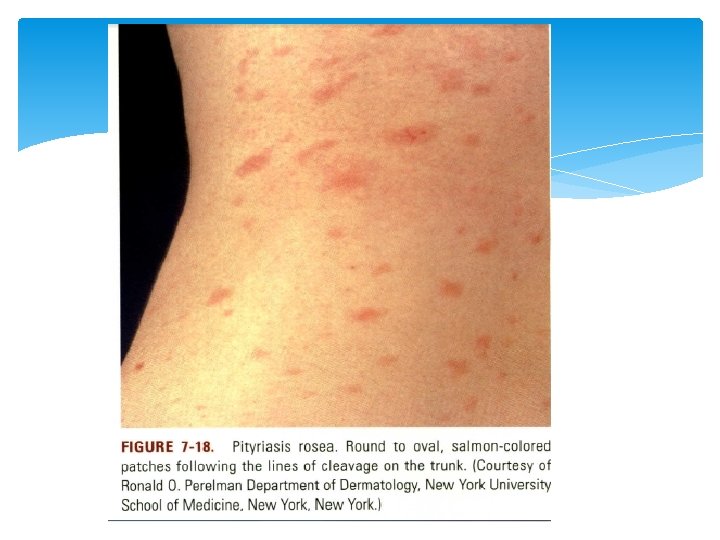
PITYRIASIS ROSEA ü self-limited dermatitis lasting from 4 to 7 weeks ü starts with a herald patch followed by a disseminated eruption. The lesions, found chiefly on the trunk, neck, and proximal extremities ü round to oval salmon-colored patches following the lines of cleavage and showing peripherally attached, thin, cigarette paper-like scales ü Several typical and atypical clinical variants have been described including papular, vesicular, urticarial, purpuric, and recurrent forms
Histopathology(PITYRIASIS ROSEA ) The patches of the disseminated eruption ü superficial perivascular dermal infiltrate (lymphocytes, with occasional eosinophils and histiocytes) ü exocytosis( lymph) ü spongiosis, intracellular edema, mild to moderate acanthosis, areas of decreased to absent granular layer, and focal parakeratosis ü Intraepidermal spongiotic vesicles ü presence of extravasated erythrocytes in the papillary dermis ü Late lesions: more likely to have a psoriasiform pattern The herald patch more pronounced acanthosis, deeper and denser perivascular inflammatory infiltrate, and papillary dermal edema
Pathogenesis The cause still unknown human herpesvirus 7 (HHV-7) is suspected Cell-mediated immunity (may be ) due to ü the presence of activated helper-inducer T-lymphocytes (CD 4+/HLA-DR+) in the epidermal and dermal infiltrate ü highly increased number of Langerhans cells (CD 1 a+) Differential Diagnosis superficial gyrate erythem (milder forms of pityriasis rosea. ) small plaque parapsoriasis Elongated mounds of parakeratosis with plasma, sparse superficial perivascular lymphocytic infiltrate, minimal exocytosis and spongiosis
GIANOTTI-CROSTI SYNDROME (PAPULAR ACRODERMATITIS OF CHILDHOOD AND PAPULOVESICULAR ACROLOCATED SYNDROME) nonpruritic, symmetrical eruption of monomorphic erythematous papules on the face, extremities, and buttocks lasting about 3 weeks lymphadenopathy and hepatitis B viral infection (link) & several other viruses ( eg EBV)
Histopathology(GIANOTTI-CROSTI SYNDROME ) q superficial and mid-dermal perivascular infiltrate of lymphocytes and histiocytes with some lymphocytes extending to the overlying epidermis where there is focal spongiosis and parakeratosis q. In some instances true lymphocytic vasculitis has been described Gianotti-Crosti sx ( Epstein-Barr virus link) ü marked papillary dermal edema with minimal spongiosis and rare eosinophils in the dermal infiltrate ü The inflammatory pattern may also present as a lichenoid interface dermatitis
Pathogenesis CD 4+ T-lymphocytes and about 20% of CD 8+ (suppressor -cytotoxic) T-lymphocytes increased number of Langerhans cells in the epidermis. surface antigen of the hepatitis B virus is detectable in the sera of all cases of papular acrodermatitis of childhood hepatitis B virus a negative : studies for other viruses by means of throat swabs and stool samples and by testing for antibodies
MUCOCUTANEOUS LYMPH NODE SYNDROME (KAWASAKI DISEASE) mucocutaneous lymph node syndrome children under 5 years of age unexplained fever lasting 5 or more days and of at least four out of five clinical criteria: (a) bilateral conjunctivitis; (b) erythematous oral mucosa, injected or dry fissured lips, and strawberry tongue (c) erythema and indurated edema of hands and feet often followed by periungual desquamation (d) polymorphous skin rash (e) cervical nonsuppurative lymphadenopathy
three clinical phases: acute, subacute, and convalescent. The first phase is the febrile period in which all the diagnostic signs may be seen The rash appears around the third to fifth day of illness and may have different morphologic patterns such as maculopapular, morbilliform, scarlatiniform, or urticarial cardiovascular complications account for the death of 2% of the children Twenty percent of untreated patients may develop coronary artery aneurysms
Histopathology( KAWASAKI DISEASE) sparse perivascular infiltrate of lymphocytes and histiocytes marked papillary dermal edema, and dilatation of blood vessels Mild exocytosis of lymphocytes can be seen An uncommon pustular variant shows sterile intraepidermal spongiform pustules with neutrophils Pathogenesis ü Predominancy of CD 4+ T-lymphocytes and CD 14+ macrophages, with only a few CD 8+ T-lymphocytes and no CD 20+ B-lymphocytes ü expression of HLA-DR
Lichen planus actinicus, or pigmentosus: ü mainly in Middle Eastern countries(20 -30%) ü more common in children or young adults ü spring and summer on sun-exposed areas, especially face Types: I. annular (the most common type) II. pigmented (resembling melasma) III. dyschromic ü Description: annular plaques with central slate blue to light brown pigmentation and well-defined, slightly raised, hypopigmented borders ü Pruritus is minimal or absent
The overlap syndrome(lichen planus/lupus erythematosus) at the same time, skin lesions with clinical, histological, and/or immunological features typical of both diseases Skin üerythematous to purplish scaly patches and plaques, some of them with central atrophy ü predilection for photodistributed areas or acral portions of extremities
Twenty-nail dystrophy ü adults as well as children. ü nails: I. longitudinal ridging and distal notching and splitting II. With time they become thin and roughened ü Other manifestations of lichen planus are usually absent ü In children, the nail changes tend to involute spontaneously after a few years ü In familial cases: unremitting course ü Congenital cases have been described ü idiopathic or associated with alopecia areata, atopic dermatitis, lichen planus, or psoriasis.
Malignant transformation q cutaneous lichen planus occurs in less than 1% of cases q. In hypertrophic lichen planus of the leg (squamous cell carcinoma or keratoacanthoma) : exceptional occurrence q squamous cell carcinoma : on long-standing lesions of lichen planus situated on mucous membranes or the vermillion border q. The incidence of carcinoma evolving in oral lichen planus is about 0. 5% with a range of 0. 3% to 3% q Development of carcinoma in ulcers of the feet rare ( lesions that had not been previously grafted)
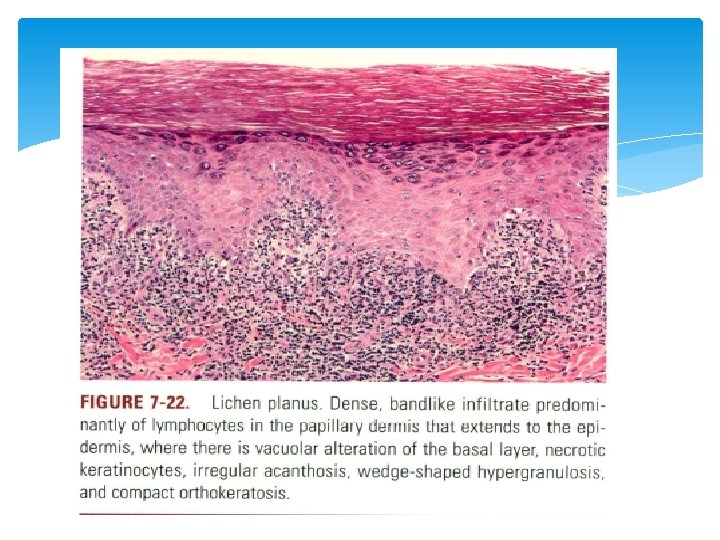
Histopathology(LP): Typical papules (a) compact orthokeratosis (b) wedge-shaped hypergranulosis (c) irregular acanthosis (d) vacuolar alteration of the basal layer (e) a band-like dermal lymphocytic infiltrate in close approximation to the epidermis
The cornified layer: ü compact orthokeratosis ü very few, if any, parakeratotic cells ( important) The granular cells qappear increased in size q. With coarse and more abundant keratohyaline granules. q. Wickham's striae : caused by a focal increase in the thickness of the granular layer and of the total epidermis
The acanthosis irregular and affects the spinous layer of the rete ridges as well as the suprapapillary plates keratinocytes of the spinous layer often appear larger and eosinophilic rete ridges: show irregular lengthening, and some of them are pointed at their lower end, giving them a sawtoothed appearance dermal papillae between elongated rete ridges are often dome shaped
The infiltrate in the upper dermis band-like and sharply demarcated at its lower border and is composed almost entirely of lymphocytes intermingled with macrophages. Melanophages ü seen in the upper dermis, often in considerable number ü old lesions, the cellular infiltrate decreases in density, but the number of melanophages increases
Oral Lp Ø parakeratosis rather than orthokeratosis Ø alternating areas of both types of keratinization with the presence of a granular layer Ø the epithelium often is atrophic Ø Ulcerations through the rupture of vesicles or as a result of necrosis of the atrophic epithelium.
lichen planopilaris Early lesions : Ø focally dense, band-like perifollicular lymphocytic infiltrate at the level of the infundibulum and the isthmus Ø vacuolar changes of the basal layer of the outer root sheath and necrotic keratinocytes Ø orthokeratosis, follicular plugging, and wedgeshaped hypergranulosis of the infundibulum Developed lesions: Ø perifollicular fibrosis and epithelial atrophy at the level of the infundibulum and isthmus (
Pseudopelade of Brocq : end-stage scarring alopecia in which no visible hair follicles remain Ø The hyperkeratotic follicular papules seen on glabrous skin with lichen planopilaris of the scalp exhibit similar changes; however, perifollicular fibrosis is slight and the does not eventuate in scarring
Ulcerative lichen planus In ulcerative lichen planus, specimens taken from skin adjacent to the ulcer generally show active lichen planus
Lichen planus actinicus The histology is similar to the typical lichen planus but with : Ø thinning of the epidermis at the center of the lesion Ø more evident pigmentary incontinence in the upper dermis.
Overlap syndrome _lichen planus/lupus erythematosus In some cases histologic features and direct immunofluorescence findings are more consistent with lichen planus in others favors lupus erythematosus and in another lesions of lichen planus that coexist, rather than overlap, with those of lupus erythematosus
Twenty-nail dystrophy manifestation of diverse underlying processes; therefore, its histology will vary. Biopsies show typical lichen planus involving the nail matrix However, spongiosis be prominent as in cases with atopic dermatitis.
Lichen planus pemphigoides biopsies taken from bullae from uninvolved skin show subepidermal bullae with an infiltrate that not band-like and contains eosinophils.
direct immunofluorescence of perilesional skin : Ig. G and C 3 in a linear arrangement along the basement membrane zone immunoelectron microscopy : C 3 is seen to be localized within the lamina lucida, analogous to its location in bullous pemphigoid. circulating Ig. G autoantibodies directed against the bullous pemphigoid antigen 180 (BP 180, type XVII collagen), a transmembrane hemidesmosomal glycoprotein of the basal keratinocytes spans the
Electron microscopy (LP) Ø the basal keratinocytes with their desmosomes and hemidesmosomes, show degenerative changes Ø the tonofilaments in the basal cells are decreased in early lesions, they are increased in later lesions Ø The dermal infiltrate, extending to the epidermis, causes damage to the lamina densa Ø The use of antikeratin immune sera has resulted in their intense staining Ø Necrotic keratinocytes often still contain cell organelles, such as melanosomes and mitochondria
electron microscopic in the vesicular lesions of lichen planus: Ø cytolysis of basal keratinocytes Ø the blister cavity situated below the spinous layer.
Immunofluorescence ( lichen planus ) Ø fibrinogen deposition demonstrated as shaggy deposits at the dermal-epidermal junction Ø occasionally are there granular deposits of Ig. M or linear deposits of C 3 or both Ig. G and C 3 in the basement membrane zone.
Immunofluorescence (lichen planopilaris) Ø deposition of Ig. M and/or Ig. A, Ig. G, and, rarely, C 3 at the level of the infundibulum and isthmus Ø deposition of fibrinogen in a shaggy pattern surrounding the affected follicles. Ø The dermal-epidermal junction is virtually always negative for deposition of immunoreactants.
Immunohistochemistry Ø The infiltrating cells in lichen planus are Tlymphocytes with few B-lymphocytes. Ø 90% are activated T-lymphocytes expressing HLA-DR antigen and some interleukin-2 receptor. Ø in older lesions of oral lichen planus the suppressor T-lymphocytes predominate
In the epidermis adjacent to the infiltrate, basal keratinocytes express HLA-DR surface antigen and intercellular adhesion molecule-1 (ICAM-1) Specific conjugations between CD 4+ (helper-inducer) Tlymphocytes and dendritic (HLA-DR+) cells and between CD 8+ (cytotoxic-suppressor) T-lymphocytes and degenerated basal keratinocytes have been observed in lesional epithelium of oral mucosa. These cell-to-cell interactions suggest a cell-mediated immune mechanism is operative.
DDX : Lichenoid drug eruptions differentiated from lichen planus by Ø the presence of focal parakeratosis with concomitant absence of the granular layer Ø necrotic keratinocytes in the basal and spinous layers Ø exocytosis of lymphocytes to the upper layers of the epidermis Ø deeper inflammatory infiltrate with numerous eosinophils
Differentiation from lichenoid lupus erythematosus is based on: Ø atrophy of the epidermis in addition to acanthosis Ø absence of eosinophilia of the keratinocytes in the spinous layer Ø a superficial band-like infiltrate with a superficial and deep perivascular and periadnexal infiltrate Ø the presence of a thickened PAS-positive basement membrane Ø dermal mucin deposits
Lichen planus _ like keratosis Ø It is a common lesion that occurs on the trunk and upper extremities of adults between the fifth and seventh decades. Ø LPLK consists of a nonpruritic papule or slightly indurated plaque that is nearly always solitary, although cases with more than one skin lesion have been reported. Ø its color varies from bright red to violaceous to brown. Ø Its surface may be smooth or slightly verrucous
a lichenoid pattern that may be indistinguishable from lichen planus. Ø there is vacuolar alteration of the basal cell layer and a band-like lymphocytic infiltrate that obscures the dermal-epidermal junction. Ø Necrotic keratinocytes are commonly seen and may be numerous Ø the epidermis often shows increased eosinophilia, hypergranulosis, and hyperkeratosis.
In contrast to lichen planus Ø parakeratosis is fairly common Although usually focal. Ø eosinophils and plasma cells in the infiltrate found in LPLK as opposed to lichen planus. Ø A residual solar lentigo at the edge of the lesion supports LPLK. Ø In lichen planus, CD 20+ B cells were fewer than in LPLK. Ø Memory T cells express a skin-homing receptor called cutaneous lymphocyte-associated antigen (CLA). This antigen is strongly expressed in lichen planus but not in LPLK.
KERATOSIS LICHENOIDES CHRONICA Ø begins in adulthood between 20 and 50 years of age Ø an extensive eruption, symmetrically distributed, predominantly on dorsal aspects of extremities and trunk consisting of red to violaceous papulonodules covered with a thick, adherent scale and arranged often in a characteristic linear and occasionally reticular pattern Ø associated seborrheic dermatitis-like eruption of the face, palmoplantar hyperkeratosis and nail changes with warty hypertrophy of the
Ø KERATOSIS LICHENOIDES CHRONICA Ø lichenoid inflammatory pattern with vacuolar alteration of the basal cell layer, necrotic keratinocytes, and a band-like inflammatory infiltrate of lymphocytes, histiocytes, and numerous plasma cells that obscures the dermal-epidermal junction Ø acanthosis &atrophy covered by a hyperkeratotic cornified layer showing focal parakeratosis and follicular plugging Prominent Ø dilated dermal capillaries are seen in cases with associated telangiectasias
LICHEN NITIDUS Ø Each papule of lichen nitidus consists mixed-cell granulomatous infiltrate that attached to the lower surface of the epidermis and confined to a widened dermal papilla. Ø The infiltrate composed of lymphocytes, mono- and a few multinucleated epithelioid histiocytes. Ø The dermal infiltrate extends into the overlying epidermis is flattened and shows vacuolar alteration of the basal cell layer, focal subepidermal clefting, diminished granular layer, and focal parakeratosis. Ø Transepidermal perforation of the infiltrate through the thinned epidermis occur Follicular involvement in lichen nitidus
Relationship Between Lichen Planus and Lichen Nitidus lichen nitidus : Ø parakeratosis and epidermal flattening Ø Occasional deposits of fibrinogen Ø significantly smaller proportion of CD 4+ (helperinducer) and HECA-452+ (skin-homing receptor) Tlymphocytes, compared to lichen planus : Ø acanthosis and hyperkeratosis Ø globular deposits of immunoglobulins at the dermalepidermal junction
LICHEN STRIATUS Ø fairly uncommon dermatitis occurs in children from 5 to 15 years of age Ø It usually manifests itself as a unilateral eruption along Blaschko's lines on the extremities, trunk, or neck as either a continuous or an interrupted band composed of minute, slightly raised, erythematous papules, which may have a scaly surface
LICHEN STRIATUS Ø superficial perivascular inflammatory infiltrate of lymphocytes admixed with histiocytes Ø in the papillary dermis the infiltrate may have a bandlike distribution with extension into the lower portion of the epidermis, where vacuolar alteration of the basal layer and necrotic keratinocytes Ø the papillary dermis occasionally contains melanophages Ø spongiosis and intracellular edema often associated with exocytosis of lymphocytes and focal parakeratosis
A very distinctive feature : presence of inflammatory infiltrate in the reticular dermis around hair follicles and eccrine glands Pathogenesis: the inflammatory cells reaching the epidermis are CD 8+ (suppressorcytotoxic) T-lymphocytes with the Langerhans cells population in the epidermis either decreased or increased Differential Diagnosis: In contrast to lichen striatus, the inflammatory infiltrate of lichen nitidus is only focally present in widened dermal papillae and contains more histiocytes. The presence of epidermal spongiosis and a deeper dermal inflammatory infiltrate around adnexal structures are features rarely in lichen planus.
INFLAMMATORY LINEAR VERRUCOUS EPIDERMAL NEVUS Ø persistent, linear, intensely pruritic lesion composed of erythematous, slightly verrucous, scaly papules arranged in one or several lines Ø Although the usual time of onset is early childhood, the disease may arise in adults ( The most common location is on a lower extremity. Ø ILVEN in association with arthritis and lichen amyloidosus has been reported. Ø ILVEN is considered to be a variant of epidermal
ILVEN: Øhyperkeratosis with foci of parakeratosis, moderate acanthosis, elongation and thickening of the rete ridges with a psoriasiform appearance, papillomatosis, and, occasionally, slight spongiosis with exocytosis of lymphocytes Øsharply demarcated alternation of orthokeratosis and parakeratosis in the cornified layer ØUnderneath the parakeratotic areas, there is mild exocytosis of lymphocytes and slight spongiosis ØThe papillary dermis shows a mild to moderate perivascular inflammatory infiltrate of lymphocytes and histiocytes.
Differential Diagnosis Ø ILVEN, in contrast to lichen striatus, is pruritic and persistent. Ø Histologically, lichen striatus tends to have a lichenoid pattern, and ILVEN a psoriasiform pattern. Ø While alternating orthokeratosis and parakeratosis can be seen in psoriasis and occasionally Munro microabscesses can be found in ILVEN, the differential diagnosis of these two entities could be sometimes difficult to assess and clinicopathologic correlation is necessary
PITYRIASIS RUBRA PILARIS Ø follicular keratotic papules and perifollicular erythema that coalesce to form orange-red scaly plaques that contain islands of normalappearing skin. As the erythema extends, the follicular component is often lost Ø The lesions spread caudally and may progress to a generalized erythroderma Ø Other clinical findings are palmoplantar keratoderma and scaling of the face and scalp.
Ø PRP: Ø acanthosis with broad and short rete ridges, slight spongiosis, thick suprapapillary plates, focal or confluent hypergranulosis, and alternating orthokeratosis and parakeratosis oriented in both vertical and horizontal directions Ø In the dermis, there is a mild superficial perivascular lymphocytic infiltrate and moderately dilated blood vessels Ø Areas corresponding to follicular papules show dilated infundibula filled out with an orthokeratotic plug, and often display perifollicular shoulders of parakeratosis and a mild perifollicular lymphocytic infiltrate
Pityriasis Lichenoides In pityriasis lichenoides chronica, the mild form, : Ø superficial perivascular infiltrate composed of lymphocytes that extends into the epidermis, where there is vacuolar alteration of the basal layer, Ø mild spongiosis Ø a few necrotic keratinocytes Ø confluent parakeratosis Ø Melanophages and small numbers of extravasated erythrocytes are commonly seen in the papillary dermis
In PLEVA, the more severe form, : Ø perivascular and dense band-like, predominantly lymphocytic infiltrate in the papillary dermis that extends into the reticular dermis in a wedge-shaped pattern that obscures the dermalepidermal junction with pronounced Ø vacuolar alteration of the basal layer, marked exocytosis of lymphocytes and erythrocytes, and intercellular and intracellular edema leading to variable degrees of epidermal necrosis Ø The overlying cornified layer shows parakeratosis and a scaly crust with neutrophils in the more severe cases Ø Variable degrees of papillary dermal edema, endothelial swelling, and extravasated erythrocytes are seen in the majority of cases
Pathogenesis Most of the cells are activated T-lymphocytes (HLADR+/CD 3+) that express CD 7 and rarely lack other T-cell antigens (CD 2, CD 5) Two constant findings in PLEVA : Ø the predominance of CD 8+ (cytotoxic-suppressor) over CD 4+ (helper-inducer) T-lymphocytes in the infiltrate Ø the expression of HLA-DR on the surrounding keratinocytes , suggesting a direct cytotoxic immune reaction in the pathogenesis of epidermal necrosis.