Acne Description Acne is a papular or pustular








 Bacterial(Gram negative folliculitis) and yeast folliculitis(not")

 Bacterial (Gram negative")








 Adapalene 0. 1% Tazarotene(Tazarac o. 05%, o. 1%")

 Many patients have a combination of comedones, papules, and pustules")
 Some patients respond to the program outlined above for")




 Description Rosacea is a common facial eruption characterized by redness, telangiectasia, lupus")





, Erythromycin(500 mg twice a day) Doxycycline(100 mg")
 is a chronic recurring disorder of the follicular unit,")



 2. 5 -10")
, metronidazole(375")
- Slides: 43
Acne Description Acne is a papular or pustular eruption, involving the face, chest, and back. History • Acne may occur at any age, but is more common in the teenage years, and may persist well into adulthood • Twenty per cent of affected individuals will develop severe acne resulting in scarring.
Acne History • Acne may occur at any age, but is more common in the teenage years, and may persist well into adulthood • Twenty per cent of affected individuals will develop severe acne resulting in scarring.
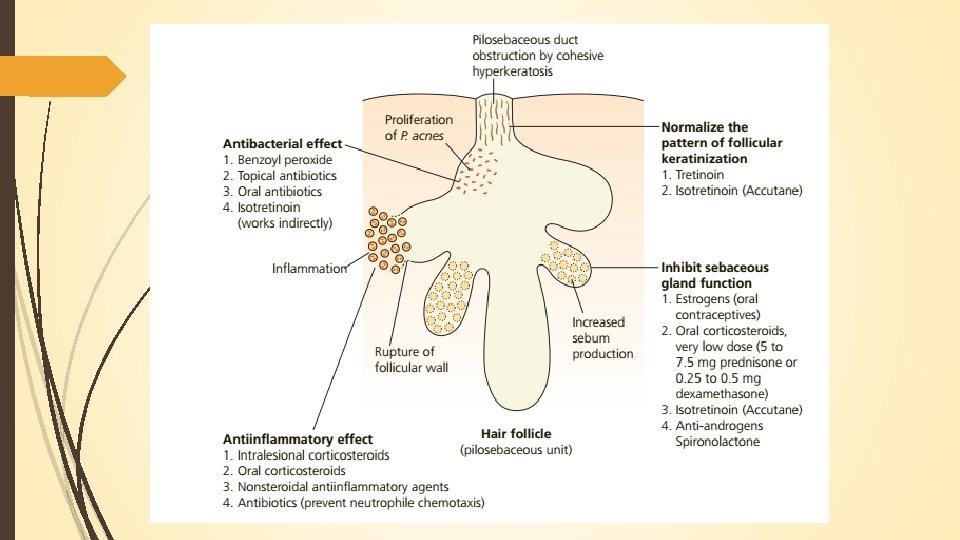
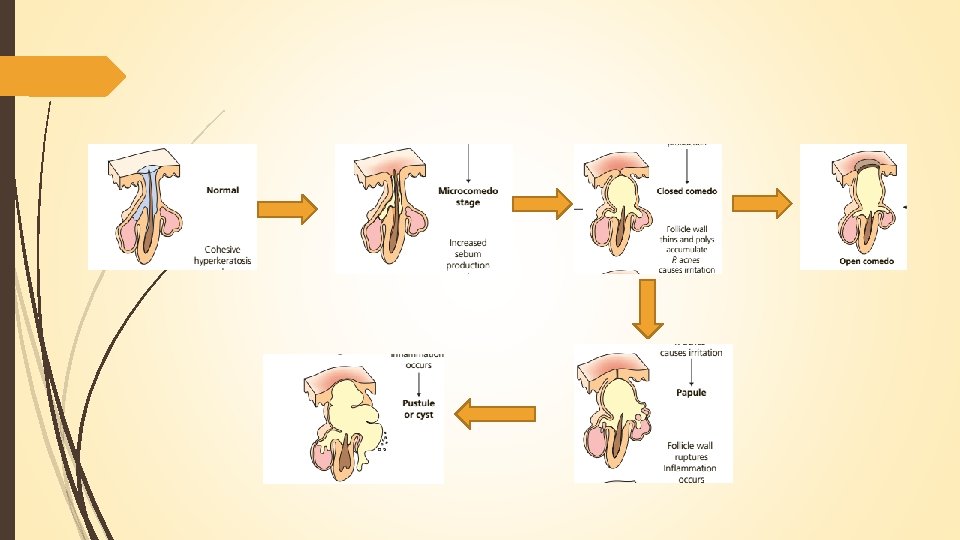
Pathogenisis Plugged follicles 2 Propionibact erium acnes 1 3 4 Inflammation increased sebum production
There are several variants of acne. Steroid acne(a comedonal and pustular acne on the chest 2 -5 weeks after a steroid has been taken) Neonatal acne(acne at birth) Infantile acne(during infancy) Acne necrotica(itchy acne of the scalp) Acne excoriée(acne that has been manipulated by the patient, leaving erosions and scars)
Dite and Acne The role of diet in the pathogenesis of acne remains unclear, although consumption of dairy production and simple sugars have been implicated in some studies
Genetics Acne can run in families and those with a family history of acne often develop acne at an earlier age. If both parents have acne, there is a 75% chance that a given child will develop acne. One parents (25%)
Skin Findings Acne lesions are divided into non inflammatory and inflammatory lesions Noninflammatory lesions consist of open comedones (blackheads and closed comedones (whiteheads). Inflammatory lesions are characterized by the presence of papules, pustules, and nodules (cysts). Recurring rupture and re-epithelialization of cysts lead to epithelial-lined sinus tracks, often accompanied by disfiguring scars. Eroded papules are seen in patients who pick acne papules (acne excoriée).
Non-skin Findings Patients with androge excess can develop signs of virilism (t of scalp hair, puberty. hirsutism) and precocious Rarely, acne occurs in association with fever and bone and joint problems( acne fulminans) Significant psychosocial issues may be present including depression, anxiety and social withdrawal. Laboratory and Biopsy
Differential Diagnosis Rosacea(flushing and blushing but no comedones) Bacterial(Gram negative folliculitis) and yeast folliculitis(not typical on the face) Keratosis pilaris (location more typical on the extensor upper arms) Perioral dermatitis( comedones are not seen)
Laboratory and biopsy Laboratory evaluation is indicated for female patients with persistent acne and onsist of evidence of a hyperandrogenic state (facial ds) hair, muscle hypertrophy, irregular menses). and ads). Tests include measurements for testosterone, follicle stimulating hormone, luteinizing hormone, and Pust dehydroepiandrosterone sulfate. Bacterial and fungal cultures can be done to rule out infectious folliculitis, sinus y disfr igutin
Differential Diagnosis Rosacea (flushing and blushing but no atients wh comedones) Bacterial (Gram negative folliculitis) and yeast folliculitis typical on the face Keratosis pilaris
Course and Prognosis Men have more severe disease than women; men are less likely to seek early medical treatment. Androgens can aggravate acne. It is important to ask about use of anabolic steroids, especially in athletes. The propensity to form scars varies from patient to patient.
severe forms of acne occur more frequently in males, but the disease tends to be more persistent in females, The most who may have periodic flare-ups before menstrual periods, which continue until menopause.
Acne flares may be seen during: periods of stress, before menstrual periods with certain medications(corticosteroids, lithium, anticonvulsants, anti-tuberculosis medications and iodides).
Acne usually begins between ages 10 years and 15 years and lasts for 5 -10 years Children who require oral medications at and an early age tend to have a more severe(facial Course. enses). Women over the age of 25 years are a special problem in the treatment of acne. They tend to have long-term low-grade acne. Girls who develop a large number of done comedones and lesions at an early age are likely to develop more severe acne.
Treatment It takes at least 2 months for most topical medications to show their full effect, so patience must be exercised. Most treatment is continual and prolonged, since it is control--not cure-that is most often achieved.
Skin Sensitivity The skin should be gently cleansed with a mild soap and tepid water. Patients should be encouraged not to excessively scrub the skin Let the skin dry before applying topical agents. Medications should be applied in a thin P layer with a gentle message to acne prone sites. If the skin becomes red or dry, one should ensure that excessive medication T in not being applied and the correct vehicle was chosen for the patient's skin type. Solutions and gels are better for oily skin while creams and lotions are better for dry skin.
Skin Sensitivity Lower concentration medications are better for patients with sensitive skin. Hair conditioners and oils should be avoided. If cosmetics are used, they should be oil free and water based. Patients should not pick or pop their acne lesions
Non-Inflamed Blocked Pores(Comedones. Blackheads and Whiteheads Agents that gently exfoliate the top layer of skin and have antibacterial properties(e. g. benzoyl peroxide) are used in combination with agents that correct follicular plugging(e. g. tretinoin, adapalene, tazarotene). One agent is usually applied in the morning and the topical other in the evening. Prescription and over-the-counter products used for exfoliation contain sulfur, salicylic acid, resorcinol, and benzoyl peroxide
Retinoids Tretinoin (0. 025%, 0. 01%) Adapalene 0. 1% Tazarotene(Tazarac o. 05%, o. 1% gel nt is and cream) Correct follicular pluging
Other medications Azelaic acid is comedolytic and antibacterial product but is only moderately effective. It may be used safely during pregnancy. Facial peels glycolic acid, salicylic acid) are sometimes used to free blocked pores.
Inflamed Pores(Papules and Pustules) Many patients have a combination of comedones, papules, and pustules Tretinoin, adapalene or tazarotene + benzoyl peroxide Tretinoin is applied at bedtime and the benzoyl peroxide or an antibiotic are applied in the morning. combination of benzoyl peroxide and an antibiotic such as clindamycin With oral antibiotics, better clinical results and a lower rate of relapse are achieved by starting at higher dosages and tapering only after control is achieved. Typical starting dosages are tetracycline 500 mg twice a day, doxycycline 100 mg twice a day and minocycline 100 mg twice a day.
Inflamed Nodules and cysts(Nodulocystic Acne) Some patients respond to the program outlined above for papular and pustular acne. If a 3 month trial of this therapy does not provide control then the treatments described here should be used. Oral Isotretinoin is very effective. A steroid(triamcinolone 2. 5 mg/ml) can be injected into individual cysts. Caution is advised given the potential for atrophy. Oral prednisone is sometimes used as initial therapy for very severe acne. In female patients, oral contraceptive can be beneficial. Spironolactone should be considered for women, especially in those not able to take an oral contraceptive,
Perioral Dermatitis Description Perioral dermatitis is a distinctive scaly papular eruption around the mouth nose, and eyes that occurs almost exclusively in women.
History The eruption may start around the mouth but may also involve the perinasal and periocular regions. This condition is asymptomatic, or somewhat itchy. Patients may have tried topical steroids, which cause temporary improvement but may contribute to refractory progressions. Perioral dermatitis typically occurs in young women and can occur in children. Fusobacterium and Candida have been isolated from lesions, but the relevance of these organisms is unknown.
Skin Findings Pinpoint papules and pustules on a red and scaling are confined to the chin and nasolabial folds. There is a clear zone around the vermilion border Pustules on the cheeks adjacent to the nostrils are common. Sometimes, perioral dermatitis remains confined to the perinasal area. Sometimes, it occurs lateral to the eyes. Children often have periocular and perinasal lesions
Rosacea(Acne Rosacea) Description Rosacea is a common facial eruption characterized by redness, telangiectasia, lupus flushing, blushing vascular component and papules and pustules(inflammatory Acne component
History Patients are usually over age 30 years Rosacea can occur in children. The cause is unknown. Demodex mites may play a pathogenic
Skin Findings Papules and pustules occur on the forehead, cheeks, nose and about the that The eyes. Erythema and/or telangiectasias are present. Severe cases have numerous pustules, that telangiectasia, diffuse erythema, oily skin, and edema Chronic, deep inflammation of the nose of leads to an irreversible skin thickening called rhinophyma This is more common in men. Uncommonly, rosacea papules can involve T the scalp, the torso, and the arms and legs.
Treatment The patient should avoid known factors that exacerbate rosacea such as hot food in and drinks, spicy foods, red wine, and sunlight. Green-based cosmetic foundations will mask the redness. Sunscreens are recommended The pustular component is treated topically or systemically
Topical therapy Metronidazole sulfacetamide plus sulfur lotion
Systemic therapy Tetracycline(500 mg twice a day), Erythromycin(500 mg twice a day) Doxycycline(100 mg twice a day), or Minocycline(100 mg twice a day) in a 2 -4 -week course usually controls the pustules
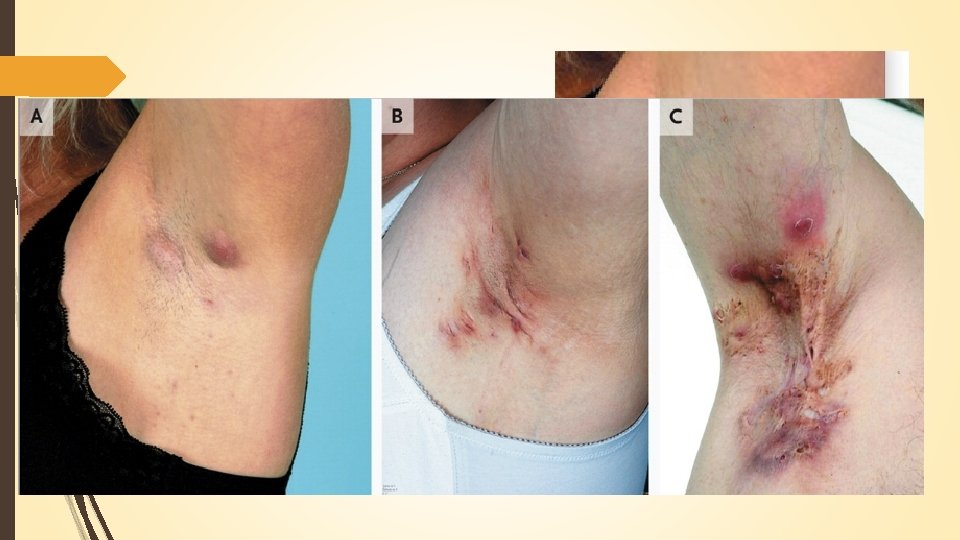
Hidradenitis Suppurativa Description Hidradenitis suppurativa(HS) is a chronic recurring disorder of the follicular unit, producing extremely painful, deep-seated nodules, cysts, sinus tracts and scars in the apocrine gland- bearing areas of the body, including the axillae, inguinal and anogenital regions.
History HS is an uncommon disorder affecting between 1 and 4% of the population and is more common in females. It presents with extremely painful recurrent “ boils" that rupture, forming sinus tracts and scars. Axiallary and inguinal involvement is more common in females, while peri- anal and buttock involvement is more common in males. The most common site of involvement is the axillae.
Causes It may be clustered in families inherited in an autosomal dominant manner; although to date no causative genes have been identified. The precise etiology of HS is not known, but likely involves follicular occlusion of the pilosebaceoappocrine apparatus with subcutaneous sinus tracts Secondary infection and inflammation. HS may be associated with Crohn's disease.
Skin Findings The hallmark is the double comedone(a blackhead with two or more surface openings"tombstones") Pink to red nodules are rounded without central necrosis, lasting up to two weeks. Extensive, deep, dermal inflammation results in large, painful, draining malodorous abscesses sinus tracts form, resulting in firm rope like scars. Follicular papules, pustules, and epidermal cysts may be associated with classic HS skin lesions. us
Treatment Large fluctuant cysts are incised and drained. Intralesional triamcinolone acetonide(Kenalog) 2. 5 -10 mg/m. L is administered for smaller cysts. Weight loss, smoking cessation, and loose clothing can sometimes be helpful to improve symptoms. Long-term oral antibiotics are a mainstay of treatment Agents include: tetracycline (500 mg twice a day), erythromycin(500 mg twice a day), doxycycline(100 mg twice a day), and minocycline Hidra(100 mg twice a day). Lower dosages are a pat tried for maintenance.
Treatment Second-line antibiotics include shoul trimethoprim-sulfamethoxazole Bactrim DS(one by mouth twice a day), metronidazole(375 mg twice a day), and clindamycin 50 mg twice a day). Oral contraceptives are sometimes helpful, especially with premenstrual flares. Isotretinoin mg/kg/day for 20 weeks is effective in selected cases(best in early non red sinus tract lesions) Anti TNF drugs(Infliximab, Etanercept and Adalimumab) are reported effective in some cases