Parasitic infection Parasites are divided into 2 main





















 or direct fluorescent antibody tests for Giardia antigens")


 • The leishmaniases are a diverse group of diseases caused by intracellular")
 typically affects children <5 yr of age in the")










 • Malaria is an acute and chronic illness characterized by paroxysms")












 Hookworms (Necator americanus and Ancylostoma spp. )")





, • Mebendazole (100 mg")









 is the most widespread, serious human cestode")











- Slides: 82
Parasitic infection
• Parasites are divided into 2 main groups taxonomically: protozoans, which are unicellular, and helminths, which are multicellular. • Chemotherapeutic agents appropriate for 1 group may not be appropriate for the other, and not all drugs are readily available.
Protozoan Diseases • • • Primary Amebic Meningoencephalitis Amebiasis Giardiasis and Balantidiasis Cryptosporidium, Isospora, Cyclospora, and Microsporidia Trichomoniasis (Trichomonas vaginalis) Leishmaniasis (Leishmania) African Trypanosomiasis (Sleeping Sickness; Trypanosoma brucei Complex) American Trypanosomiasis (Chagas Disease; Trypanosoma cruzi) Malaria (Plasmodium) Babesiosis (Babesia) Toxoplasmosis (Toxoplasma gondii)
Amebiasis • Entamoeba histolytica infects up to 10% of the world's population; endemic foci are particularly common in the tropics, especially in areas with low socioeconomic and sanitary standards. • In most infected individuals, E. histolytica parasitizes the lumen of the gastrointestinal tract and causes few symptoms or sequelae. • The 2 most common forms of disease caused by E. histolytica are amebic colitis with parasitic invasion of the intestinal mucosa and amebic liver abscess with dissemination of the parasite to the liver.
Etiology • E. histolytica, the pathogenic species, causes a spectrum of disease and can become invasive. • Infection is acquired through the ingestion of parasite cysts, which measure 10 -18 mm in diameter and contain 4 nuclei. • Cysts are resistant to harsh environmental conditions including the concentrations of chlorine commonly used in water purification but can be killed by heating to 55 C.
• After ingestion, cysts are resistant to gastric acidity and digestive enzymes and germinate in the small intestine to form trophozoites. • These large, actively motile organisms colonize the lumen of the large intestine and may invade the mucosal lining. • Infection is not transmitted by trophozoites, as these rapidly degenerate outside the body and are unable to survive the low p. H of the stomach if swallowed.
Epidemiology • It is estimated that infection with E. histolytica leads to 50 million cases of symptomatic disease and 40, 000 -110, 000 deaths annually. • Prospective studies have shown that 4 -10% of individuals infected with E. histolytica develop amebic colitis and that <1% of infected individuals develop disseminated disease, including amebic liver abscess.
Clinical Manifestations • Clinical presentations range from asymptomatic cyst passage to amebic colitis, amebic dysentery, ameboma, and extraintestinal disease. • E. histolytica infection is asymptomatic in about 90% of persons but has the potential to become invasive and should be treated. • Severe disease is more common in young children, pregnant women, malnourished individuals, and persons taking corticosteroids. • Extraintestinal disease usually involves the liver, but less common extraintestinal manifestations include amebic brain abscess, pleuropulmonary disease, ulcerative skin, and genitourinary lesions.
Diagnosis • A diagnosis of amebic colitis is made in the presence of compatible symptoms with detection of E. histolytica antigens in stool. • This approach has a greater than 95% sensitivity and specificity and coupled with a positive serology test is the most accurate means of diagnosis in developed countries. • The E. histolytica II stool antigen detection test (Tech. Lab, Blacksburg, VA) is able to distinguish E. histolytica from E. dispar infection. • Microscopic examination of stool samples has a sensitivity of 60%. • Sensitivity can be increased to 85 -95% by examining 3 stools, since excretion of cysts can be intermittent. • However, microscopy cannot differentiate between E. histolytica and E. dispar unless phagocytosed erythrocytes (specific for E. histolytica) are seen.
Differential diagnosis • The differential diagnosis for amebic colitis includes colitis due to bacterial (Shigella, Salmonella, enteropathogenic Escherichia coli, Campylobacter, Yersinia, Clostridium difficile), mycobacterial (tuberculosis and atypical mycobacteria), and viral (cytomegalovirus) pathogens, as well as noninfectious causes such as inflammatory bowel disease (IBD). • Pyogenic liver abscess due to bacterial infection, hepatoma, and echinococcal cysts are in the differential for amebic liver abscess. • However, echinococcal cysts are rarely associated with systemic symptoms such as fever unless there is cyst rupture or leakage.
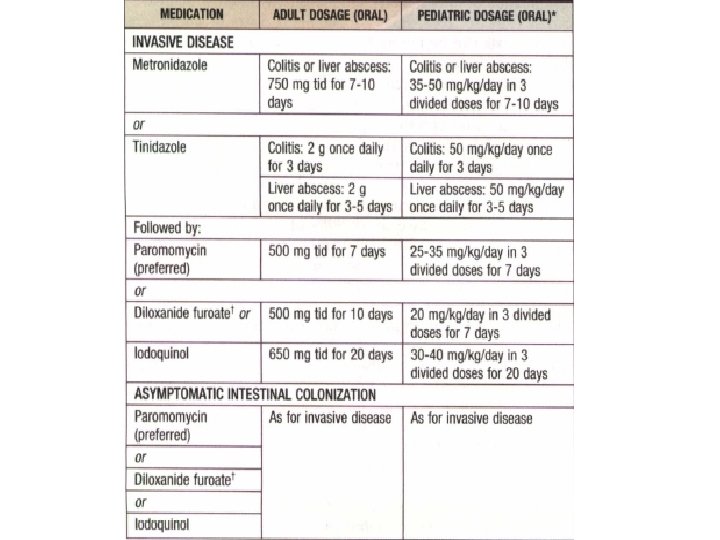
Treatment • Invasive amebiasis is treated with a nitroimidazole such as metronidazole or tinidazole and then a luminal amebicide.
Prevention • Control of amebiasis can be achieved by exercising proper sanitation and avoiding fecal-oral transmission. • Regular examination of food handlers and thorough investigation of diarrheal episodes may help identify the source of infection. • No prophylactic drug or vaccine is currently available for amebiasis.
Giardiasis • Giardia lamblia is a flagellated protozoan that infects the duodenum and small intestine. • Infection results in clinical manifestations that range from asymptomatic colonization to acute or chronic diarrhea and malabsorption. • Infection is more prevalent in children than in adults.
• Giardia is endemic in areas of the world with poor levels of sanitation. • It is also an important cause of morbidity in developed countries, where it is associated with urban child-care centers, residential institutions for the developmentally delayed, and water-borne and food-borne outbreaks. • Giardia is a particularly significant pathogen in people with malnutrition, certain immunodeficiencies, and cystic fibrosis.
Etiology • The life cycle of G. lamblia (also known as Giardia intestinalis or Giardia duodenalis) is composed of 2 stages: trophozoites and cysts. • Giardia infects humans after ingestion of as few as 10 -100 cysts (which measure 8 -10 mm in diameter). • Each ingested cyst produces 2 trophozoites in the duodenum. • After excystation, trophozoites colonize the lumen of the duodenum and proximal jejunum, where they attach to the brush border of the intestinal epithelial cells and multiply by binary fission.
Epidemiology • Giardia occurs worldwide and is the most common intestinal parasite identified in public health laboratories in the USA, where it is estimated that up to 2 million cases of giardiasis occur annually. • The age-specific prevalence of giardiasis is high during childhood and begins to decline after adolescence. • The asymptomatic carrier rate of G. lamblia in the USA is as high as 20 -30% in children younger than 36 mo of age attending child-care centers. • Asymptomatic carriage may persist for several months.
• Transmission of Giardia is common in certain high-risk groups, including children and employees in child-care centers, consumers of contaminated water, travelers to certain areas of the world, men who have sex with men, and persons exposed to certain animals. • Humoral immunodeficiencies, including common variable hypogammaglobulinemia and X-linked agammaglobulinemia, predispose humans to chronic symptomatic Giardia infection, suggesting the importance of humoral immunity in controlling giardiasis. • Selective immunoglobulin A (Ig. A) deficiency is also associated with Giardia infection.
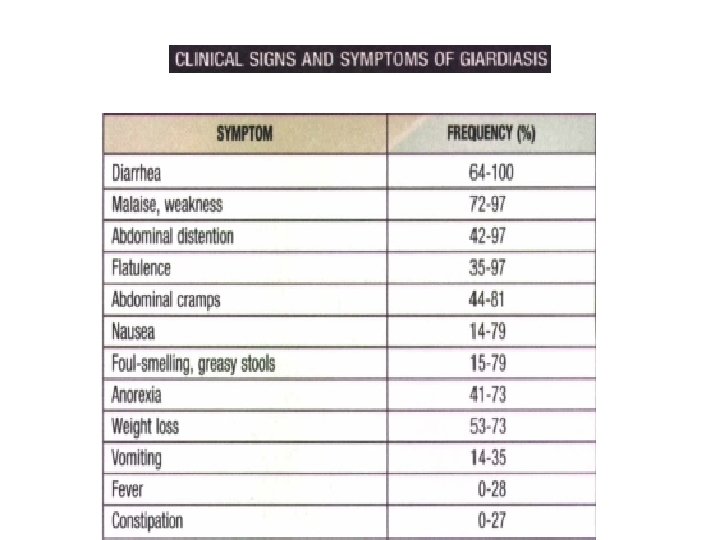
Clinical Manifestations • The incubation period of Giardia infection usually is 1 -2 wk but may be longer. • A broad spectrum of clinical manifestations occurs, depending on the interaction between G. lamblia and the host. • Children who are exposed to G. lamblia may experience asymptomatic excretion of the organism, acute infectious diarrhea, or chronic diarrhea with persistent gastrointestinal tract signs and symptoms, including failure to thrive and abdominal pain or cramping.
• Symptomatic infections occur more frequently in children than in adults. • Most symptomatic patients usually have a limited period of acute diarrheal disease with or without low -grade fever, nausea, and anorexia; in a small proportion of patients, an intermittent or more protracted course characterized by diarrhea, abdominal distention and cramps, bloating, malaise, flatulence, nausea, anorexia, and weight loss develops.
Diagnosis • Giardiasis should be considered in children who have acute nondysenteric diarrhea, persistent diarrhea, intermittent diarrhea and constipation, malabsorption, chronic crampy abdominal pain and bloating, failure to thrive, or weight loss. • It should be particularly high in the differential diagnosis of children in child care, children in contact with an index case, children with a history of recent travel to an endemic area, and children with humoral immunodeficiencies. • Testing for giardiasis should be standard for internationally adopted children from Giardia-endemic areas, and screening for iron deficiency should be considered in internationally adopted children with giardiasis.
• Stool enzyme immunoassay (EIA) or direct fluorescent antibody tests for Giardia antigens are now the tests of choice for giardiasis in most situations. EIA is less reader dependent and more sensitive for detection of Giardia than microscopy. • Traditionally, a diagnosis of giardiasis has been established by microscopy documentation of trophozoites or cysts in stool specimens, but 3 stool specimens are required to achieve a sensitivity of >90%. • In patients with chronic symptoms in whom giardiasis is suspected but in whom testing of stool specimens for Giardia yields a negative result, aspiration or biopsy of the duodenum or upper jejunum should be considered. • In a fresh specimen, trophozoites usually can be visualized by direct wet mount.
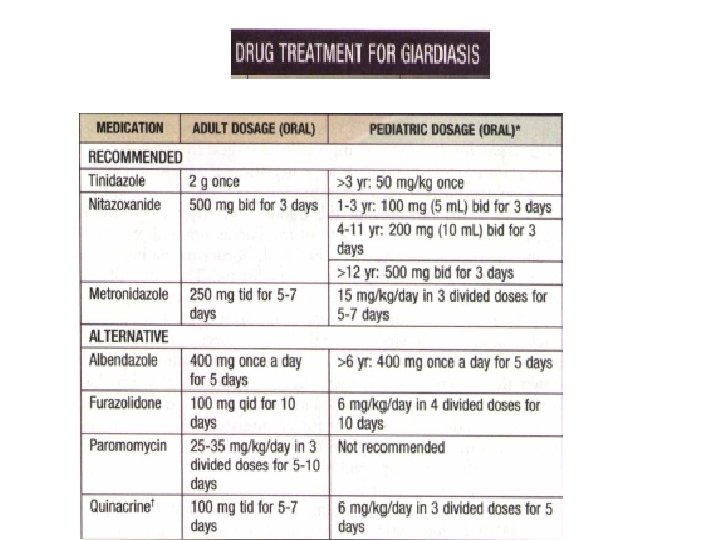
Treatment • Children with acute diarrhea in whom Giardia organisms are identified should receive therapy. • In addition, children who manifest failure to thrive or exhibit malabsorption or gastrointestinal tract symptoms such as chronic diarrhea should be treated. • Asymptomatic excreters generally are not treated except in specific instances such as in outbreak control, for prevention of household transmission by toddlers to pregnant women and patients with hypogammaglobulinemia or cystic fibrosis, and in situations requiring oral antibiotic treatment where Giardia may have produced malabsorption of the antibiotic.
Prevention • Infected persons and persons at risk should practice strict handwashing after any contact with feces. • This point is especially important for caregivers of diapered infants in child-care centers, where diarrhea is common and Giardia organism carriage rates are high.
Leishmaniasis (Leishmania) • The leishmaniases are a diverse group of diseases caused by intracellular protozoan parasites of the genus Leishmania, which are transmitted by phlebotomine sandflies. • Multiple species of Leishmania are known to cause human disease involving the skin and mucosal surfaces and the visceral reticuloendothelial organs. • Cutaneous disease is generally mild but may cause cosmetic disfigurement. • Mucosal and visceral leishmaniasis is associated with significant morbidity and mortality.
Visceral Leishmaniasis • VL (kala-azar) typically affects children <5 yr of age in the New World and Mediterranean region (L. infantum/chagasi) and older children and young adults in Africa and Asia (L. donovani). • After inoculation of the organism into the skin by the sandfly, the child may have a completely asymptomatic infection or an oligosymptomatic illness that either resolves spontaneously or evolves into active kala-azar.
• Children with asymptomatic infection are transiently seropositive but show no clinical evidence of disease.
• Children who are oligosymptomatic have mild constitutional symptoms (malaise, intermittent diarrhea, poor activity tolerance) and intermittent fever; most will have a mildly enlarged liver. • In most of these children the illness will resolve without therapy, but in approximately 25% it will evolve to active kalaazar within 2 -8 mo. • Extreme incubation periods of several years have rarely been described. • During the 1 st few weeks to months of disease evolution the fever is intermittent, there is weakness and loss of energy, and the spleen begins to enlarge.
• The classic clinical features of high fever, marked splenomegaly, hepatomegaly, and severe cachexia typically develop approximately 6 mo after the onset of the illness, but a rapid clinical course over 1 mo has been • • noted in up to 20% of patients in some series. At the terminal stages of kala-azar the hepatosplenomegaly is massive, there is gross wasting, the pancytopenia is profound, and jaundice, edema, and ascites may be present. Anemia may be severe enough to precipitate heart failure. Bleeding episodes, especially epistaxis, are frequent. The late stage of the illness is often complicated by secondary bacterial infections, which frequently are a cause of death.
• A younger age at the time of infection and underlying malnutrition may be risk factors for the development and more rapid evolution of active VL. • Death occurs in >90% of patients without specific antileishmanial treatment.
Laboratory Findings • Laboratory findings associated with classic kala-azar include anemia (hemoglobin 58 mg/d. L), thrombocytopenia, leukopenia (2, 000 -3, 000 cells/mic. L), elevated hepatic transaminase levels, and hyperglobulinemia (>5 g/d. L) that is mostly immunoglobulin G (Ig. G).
Differential Diagnosis • VL should be strongly suspected in the patient with prolonged fever, weakness, cachexia, marked splenomegaly, hepatomegaly, cytopenias, and hypergammaglobulinemia who has had potential exposure in an endemic area. • The clinical picture may also be consistent with that of malaria, typhoid fever, miliary tuberculosis, schistosomiasis, brucellosis, amebic liver abscess, infectious mononucleosis, lymphoma, and leukemia.
Diagnosis • Serologic testing by enzyme immunoassay, indirect fluorescence assay, or direct agglutination is very useful in VL because of the very high level of antileishmanial antibodies. • An enzyme-linked immunosorbent assay using a recombinant antigen (K 39) has a sensitivity and specificity for VL that is close to 100%. • A negative serologic test result in an immunocompetent individual is strong evidence against a diagnosis of VL. • Serodiagnostic tests have positive findings in only about half of the patients who are co-infected with HIV.
• In patients with VL, smears or cultures of material from splenic, bone marrow, or lymph node aspirations are usually diagnostic. • In experienced hands, splenic aspiration has a higher diagnostic sensitivity, but it is rarely performed in the USA because of the risk for bleeding complications.
Treatment • All patients with VL or ML should receive therapy. • Glucantime • Amphotericin B
Malaria (Plasmodium) • Malaria is an acute and chronic illness characterized by paroxysms of fever, chills, sweats, fatigue, anemia, and splenomegaly. • It has played a major role in human history, causing harm to more people than perhaps any other infectious disease. • Malaria is of overwhelming importance in the developing world today, with an estimated 300 to 500 million cases and more than 1 million deaths each year. • Most malarial deaths occur among infants and young children.
Etiology • Malaria is caused by intracellular Plasmodium protozoa transmitted to humans by female Anopheles mosquitoes. • Prior to 2004, only 4 species of Plasmodium were known to cause malaria in humans: P. falciparum, P. malariae, P. ovale, and P. vivax. • In 2004 P. knowlesi (a primate malaria species) was also shown to cause human malaria, and cases of P. knowlesi infection have been documented in Malaysia, Indonesia, Singapore, and the Philippines.
• Malaria also can be transmitted through blood transfusion, use of contaminated needles, and from a pregnant woman to her fetus. • The risk for blood transmission is small and decreasing in the USA but may occur by way of whole blood, packed red blood cells, platelets, leukocytes, and organ transplantation.
Clinical Manifestations • The classic presentation of malaria is seldom noted with other infectious diseases and consists of paroxysms of fever alternating with periods of fatigue but otherwise relative wellness. • Febrile paroxysms are characterized by high fever, sweats, and headache, as well as myalgia, back pain, abdominal pain, nausea, vomiting, diarrhea, pallor, and jaundice.
• Typical laboratory findings include anemia, thrombocytopenia, and a normal or low leukocyte count. The erythrocyte sedimentation rate (ESR) is often elevated.
WORLD HEALTH ORGANIZATION CRITERIA FOR SEVERE MALARIA, 2000 Impaired consciousness Prostration Respiratory distress Multiple seizures Jaundice Hemoglobinuria Abnormal bleeding Severe anemia Circulatory collapse Pulmonary edema
Diagnosis • Any child who presents with fever or unexplained systemic illness and has traveled or resided in a malaria-endemic area within the previous year should be assumed to have lifethreatening malaria until proven otherwise. • Malaria should be considered regardless of the use of chemoprophylaxis. • Important criteria that suggest P. falciparum malaria include symptoms occurring less than 1 mo after return from an endemic area, more than 2% parasitemia, ring forms with double chromatin dots, and erythrocytes infected with more than 1 parasite.
• The diagnosis of malaria is established by identification of organisms on Giemsa-stained smears of peripheral blood or by rapid immunochromatographic assay.
Differential Diagnosis • The differential diagnosis of malaria is broad and includes viral infections such as influenza and hepatitis, sepsis, pneumonia, meningitis, encephalitis, endocarditis, gastroenteritis, pyelonephritis, babesiosis, brucellosis, leptospirosis, tuberculosis, relapsing fever, typhoid fever, yellow fever, amebic liver abscess, Hodgkin disease, and collagen vascular disease.
Treatment • Fever without an obvious cause in any patient who has left a P. falciparum endemic area within 30 days and is nonimmune should be considered a medical emergency. • Thick and thin blood smears should be obtained immediately, and all children with symptoms of severe disease should be hospitalized. • If blood films are negative, they should be repeated every few hours.
• If the patient is severely ill, antimalarial therapy should be initiated immediately. • Outpatient therapy generally is not given to nonimmune children but may be considered in immune or semi-immune children who have low-level parasitemia (less than 1%), no evidence of complications defined by the World Health Organization (WHO), no vomiting, and a lack of toxic appearance; who are able to contact the physician or emergency department at any time; and in whom follow-up within 24 hr is assured.
Toxoplasmosis • Toxoplasma gondii, an obligate intracellular protozoan, is acquired perorally, transplacentally, or, rarely, parenterally in laboratory accidents; by transfusion; or from a transplanted organ. • In immunologically normal children, acute acquired infection may be asymptomatic, cause lymphadenopathy, or affect almost any organ.
Clinical Manifestations • Manifestations of primary infection with T. gondii are highly variable and are influenced primarily by host immunocompetence. • There may be no signs or symptoms or severe disease. • Reactivation of previously asymptomatic congenital toxoplasmosis usually manifests as ocular toxoplasmosis.
Helminthic Diseases • • Ascariasis (Ascaris lumbricoides) Hookworms (Necator americanus and Ancylostoma spp. ) Trichuriasis (Trichuris trichiura) Enterobiasis (Enterobius vermicularis) Strongyloidiasis (Strongyloides stercoralis) Flukes (Liver, Lung, and Intestinal) Adult Tapeworm Infections Echinococcosis (Echinococcus granulosus and Echinococcus multilocularis)
Ascariasis • Ascariasis is caused by the nematode, or roundworm, Ascaris lumbricoides. • The reproductive potential of Ascaris is prodigious; a gravid female worm produces 200, 000 eggs/day. • After passage in the feces, the eggs embryonate and become infective in 5 -10 days under favorable environmental conditions. • Adult worms can live for 12 -18 mo.
Ascaris lumbricoides
Epidemiology • Ascariasis occurs globally and is the most prevalent human helminthiasis in the world. • It is most common in tropical areas of the world where environmental conditions are optimal for maturation of ova in the soil. • Approximately 1 billion persons are estimated to be infected. • Key factors linked with a higher prevalence of infection include poor socioeconomic conditions, use of human feces as fertilizer, and geophagia.
Clinical Manifestations • The clinical presentation depends on the intensity of infection and the organs involved. • Most individuals have low to moderate worm burdens and have no symptoms or signs. • The most common clinical problems are due to pulmonary disease and obstruction of the intestinal or biliary tract.
Diagnosis • Microscopic examination of fecal smears can be used for diagnosis because of the high number of eggs excreted by adult female worms. • A high index of suspicion in the appropriate clinical context is needed to diagnose pulmonary ascariasis or obstruction of the gastrointestinal tract. • Ultrasound examination of the abdomen is capable of visualizing intraluminal adult worms.
Treatment • Albendazole (400 mg PO once, for all ages), • Mebendazole (100 mg bid PO for 3 days or 500 mg PO once for all ages) • Pyrantel pamoate (11 mg/kg PO once, maximum 1 g) • Piperazine citrate (75 mg/kg/day for 2 days maximum 3. 5 g/day)
Enterobiasis • The cause of enterobiasis, or pinworm infection, is Enterobius vermicularis, which is a small (1 cm in length), white, threadlike nematode, or roundworm, that typically inhabits the cecum, appendix, and adjacent areas of the ileum and ascending colon. • Gravid females migrate at night to the perianal and perineal regions, where they deposit up to 15, 000 eggs.
• Eggs embryonate within 6 hr and remain viable for 20 days. • Human infection occurs by the fecal-oral route typically by ingestion of embryonated eggs that are carried on fingernails, clothing, bedding, or house dust. • After ingestion, the larvae mature to form adult worms in 36 -53 days.
Epidemiology • Enterobiasis infection occurs in individuals of all ages and socioeconomic levels. • It infects 30% of children worldwide, and humans are the only known host. • The prevalence of pinworm infection is highest in children 5 -14 yr of age.
Clinical Manifestations • Pinworm infection is innocuous and rarely causes serious medical problems. • The most common complaints include itching and restless sleep secondary to nocturnal perianal or perineal pruritus. • Eosinophilia is not observed in most cases, because tissue invasion does not occur. • Aberrant migration to ectopic sites occasionally may lead to appendicitis, chronic salpingitis, pelvic inflammatory disease, peritonitis, hepatitis, and ulcerative lesions in the large or small bowel.
Diagnosis • A history of nocturnal perianal pruritus in children strongly suggests enterobiasis. • Definitive diagnosis is established by identification of parasite eggs or worms. • Microscopic examination of adhesive cellophane tape pressed against the perianal region early in the morning frequently demonstrates.
• Repeated examinations increase the chance of detecting ova; a single examination detects 50% of infections, 3 examinations 90%, and 5 examinations 99%. • Worms seen in the perianal region should be removed and preserved in 75% ethyl alcohol until microscopic examination can be performed. • Digital rectal examination may also be used to obtain samples for a wet mount. • Routine stool samples rarely demonstrate Enterobius ova.
Treatment • Anthelmintic drugs should be administered to infected individuals and their family members. • A single oral dose of mebendazole (100 mg PO for all ages) repeated in 2 wk results in cure rates of 90100%. • Alternative regimens include a single oral dose of albendazole (400 mg PO for all ages) repeated in 2 wk, or a single dose of pyrantel pamoate (11 mg/kg PO, maximum 1 g).
• Frequent changing of underclothes, bed clothes, and bed sheets decreases environmental egg contamination and may decrease the risk for autoinfection.
Prevention • Household contacts can be treated at the same time as the infected individual. • Repeated treatments every 3 -4 mo may be required in circumstances with repeated exposure, such as with institutionalized children. • Good hand hygiene is the most effective method of prevention.
Echinococcosis • Echinococcosis (hydatid disease or hydatidosis) is the most widespread, serious human cestode infection in the world. • Two major Echinococcus species are responsible for distinct clinical presentations, E. granulosus (cystic hydatid disease) and the more malignant E. multilocularis (alveolar hydatid disease).
Clinical Manifestations • In the liver, many cysts never become symptomatic and regress spontaneously or produce relatively nonspecific symptoms. • Symptomatic cysts can cause increased abdominal girth, hepatomegaly, a palpable mass, vomiting, or abdominal pain. • However, the more serious complications result from compression of adjacent structures, spillage of cyst contents, and location of cysts in sensitive areas, such as the reproductive tract, brain, and bone.
• Anaphylaxis can occur with cyst rupture or spontaneous spillage, due to trauma or intraoperatively. • Jaundice due to cystic hydatid disease is rare. • In the lung, cysts produce chest pain, cough, or hemoptysis. • Bone cysts may cause pathologic fractures, and cysts in the genitourinary system may produce hematuria or infertility.
Diagnosis • Subcutaneous nodules, hepatomegaly, or a palpable abdominal mass may be found. • The parasite cannot be recovered from any easily accessible body fluid unless a lung cyst ruptures, after which protoscolices or layers of cyst wall may briefly be seen in sputum.
• Ultrasonography is the most valuable tool for both the diagnosis and treatment of cystic hydatid disease of the liver. • The presence of internal membranes and falling echogenic cyst material (hydatid sand) observed in real time aid in the diagnosis.
• Alveolar disease is less cystic in appearance and resembles a diffuse solid tumor. • CT findings are similar to those of ultrasonography and may at times be useful in distinguishing alveolar from cystic hydatid disease in geographic regions where both occur. • CT or MRI is also important in planning a surgical intervention. • Lung hydatid is usually apparent on chest x-ray.
• Serologic studies may be useful in confirming a diagnosis of cystic echinococcosis, but the false-negative rate may be >50%. • Most patients with alveolar hydatidosis develop detectable antibody responses.
Treatment • Indications for surgery are the presence of large liver cysts with multiple daughter cysts, single superficially situated liver cysts that may rupture spontaneously or as the result of a trauma, infected cysts, cysts communicating with the biliary tree and/or exerting pressure on adjacent vital organs, and cysts in the lung, brain, kidney, or bones.
• For simple, accessible cysts surrounded by tissue, ultrasound- or CT-guided Percutaneous Aspiration, Instillation (hypertonic saline or another scolicidal agent) and Re-aspiration (PAIR) is the preferred therapy.
• Nonpregnant patients with cysts not amenable to PAIR or surgery or with contraindications can be managed with albendazole (15 mg/kg/day divided bid PO for 1 -6 mo, maximum 800 mg/day). A favorable response occurs in 40 -60% of patients.
• Adverse effects include occasional alopecia, mild gastrointestinal disturbance, and elevated transaminases on prolonged use. • Because of leukopenia, the U. S. Food and Drug Administration recommends that blood counts be monitored at the beginning and every 2 wk during therapy.
Prognosis • Factors predictive of success with chemotherapy are age of the cyst (<2 yr), low internal complexity of the cyst, and small size. • The site of the cyst is not important, although cysts in bone respond poorly. For alveolar hydatidosis, if surgical removal is unsuccessful, the average mortality is 92% by 10 yr after diagnosis.