Nutrition Care Process Assessment Nutrition Assessment The purpose




, nutrition assessment is")






















 ¨ Hamwi (%")




![Calculating BMI (Quetelet Index) ¨ BMI = Weight (kg) divided by (height [m]2) OR](https://slidetodoc.com/presentation_image/03c129fc6472bed1d363e9cb0ebe282f/image-34.jpg "Calculating BMI (Quetelet Index) ¨ BMI = Weight (kg) divided by (height [m]2) OR")
 from")









 ¨ Validity depends on measurement technique and repetition")









 ¨ Body weight ¨ Body fat ¨ Somatic")



 ¨ Men = 66. 47 + (13. 75 x wt")




![Adjusted Body Weight ¨ [(ABW – IBW) *. 25] + IBW Alternative equation: ¨](https://slidetodoc.com/presentation_image/03c129fc6472bed1d363e9cb0ebe282f/image-65.jpg "Adjusted Body Weight ¨ [(ABW – IBW) *. 25] + IBW Alternative equation: ¨")





 = 629 – 11(A) + 25(W)")
")

 ages 19")




 (0. 85) + Ve(33) + Tmax(175)")








- Slides: 87
Nutrition Care Process: Assessment
Nutrition Assessment ¨ The purpose of nutrition assessment is to collect and interpret relevant patient/client information to identify nutrition-related problems and their causes ¨ Is the first step in the Nutrition Care Process ¨ Different from monitoring and evaluation where similar or same data may be used to determine changes in client behavior or nutrition status and the efficacy of nutrition intervention ADA IDNT Reference Manual, 2008, p. 8
Nutrition Assessment Involves Critical Thinking ¨ Determine appropriate data to collect and selecting valid and reliable tools ¨ Distinguish relevant from irrelevant data ¨ Select appropriate norms and standards for comparing the data ¨ Organizing and categorizing the data in a meaningful way that relates to nutrition problems
Nutrition Assessment Is Ongoing ¨ Is the first step in the Nutrition Care Process but not an isolated event ¨ A dynamic process that evolves throughout the NCP as the pt’s status changes or new information becomes available
Nutrition Assessment ¨ In ADA’s draft Standards of Professional Practice (SOPP), nutrition assessment is a function of the registered dietitian ¨ A dietetic technician, registered, contributes by collecting data, providing some interventions, and evaluating and monitoring patient/client response ¨ Assessment parameters and possible nutrition diagnoses are listed in the IDNT manual and pocket guide
Nutrition Assessment Data ¨ Data collected depends on the practice setting ¨ For individuals, data can come directly from pt/client through interview, observations, and measurement; from health care providers or referring agencies, medical record or laboratory tests ¨ For populations, data from surveys, administrative data sets, and epidemiological and research studies are used ADA IDNT Reference Manual, 2008, p. 8
Categories of Nutrition Assessment Data ¨ Food/nutrition history ¨ Biochemical data, medical tests and procedures ¨ Anthropometric measurements ¨ Physical examination findings ¨ Client history IDNT Reference Manual, ADA, 2008, p. 9
Food/Nutrition Histories: Food Intake ¨ Composition and adequacy of food and nutrient intake, meal and snack patterns, environmental cues to eating, food and nutrient tolerance, and current diets and/or food modifications ADA IDNT Reference Manual, 2008, p. 11)
Food/Nutrition Histories: Nutrition and Health Awareness ¨ Knowledge and beliefs about nutrition recommendations, self-monitoring/ management practices, and past nutrition counseling and education ADA IDNT Reference Manual, 2008, p. 11)
Food/Nutrition Histories: Physical Activity and Exercise ¨ Functional status, activity patterns, amount of sedentary time (TV, phone, computer) and exercise intensity, frequency, and duration ADA IDNT Reference Manual, 2008, p. 11
Food/Nutrition Histories: Food Availability ¨ Food planning, purchasing, preparation abilities and limitations, food safety practices, food/nutrition program utilization, and food insecurity ADA IDNT Reference Manual, 2008, p. 11
Biochemical Data, Medical Tests and Procedures ¨ Include laboratory data (e. g. electrolytes, glucose, lipid panel ¨ Gastric emptying time ¨ Colonoscopy, CT scan or EKG results
Anthropometric Measurements ¨ Include height, weight, body mass index, growth chart percentile, growth rate, and rate of weight change
Physical Examination Findings ¨ Include oral health, general physical appearance, muscle and subcutaneous fat wasting, and affect
Client History ¨ Social history: socioeconomic status, social and medical support, cultural and religious beliefs, housing situation, and social isolation/connection ¨ Personal history: factors including age, occupation, role in family, and education level ¨ Medical/health history includes chief nutrition complaint, present/past illness, surgical history, chronic disease or complication risk, family medical history, mental/emotional health and cognitive abilities ¨ Medication/supplement history: prescription and over-the-counter drugs, herbal and dietary supplements, and illegal drugs IDNT Reference Manual, ADA, 2008, p. 11
Food/Nutrition History Information
Food/Nutrition History Information — cont’d
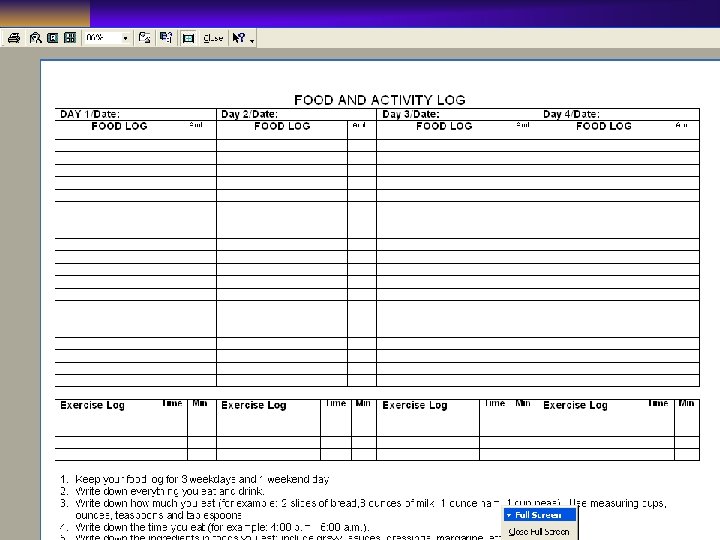
Methods of Obtaining Intake Data ¨ Direct observation and nutrient analysis: can be used only in controlled settings; doesn’t represent usual intake; calorie counts fall into this category ¨ Food record or diary: prospective tool; asks client to record or weigh food intake for a specific time period ¨ Food frequency questionnaire: retrospective; asks client to complete a survey about food intake over a specific time period ¨ 24 -hour recall: retrospective tool; asks client about food intake during the previous 24 hours
24 -Hour Recall Strengths Weaknesses Less likely to modify dietary behavior Memory dependent Quick and inexpensive Overestimates low intake Low client burden Underestimates high intake Literacy independent High-interviewer variability
Food Records Strengths Weaknesses Greater precision than single 24 -hour recall Not memory reliant Eating behavior may change Literate and numerate dependent; requires knowledge of portion sizes High client burden Considered “actual” intake
Food Frequency Questionnaire Strengths Weaknesses Low client burden Primarily provides qualitative information Quick and inexpensive Literate and numerate dependent Can examine specific nutrients Memory dependent Considered “usual” intake Cognitively difficult since food list not meal based Easily standardized Accuracy improves when combined with other data
Direct Observation Strengths Weaknesses Low client burden Client unaware of assessment Not memory or literacy dependent High staff burden Intrusive Difficult to attain and interpret Does not represent usual intake Expensive
NCI Food Frequency Questionnaire
Food Diary What’s wrong with this picture?
Weight Status and Anthropometry
Anthropometry ¨ Involves obtaining physical measurements of an individual and relating them to standards that reflect the growth and development of the individual ¨ Can be used in nutrition assessment and evaluation and monitoring
Height Measurement ¨ Standing: taken without shoes, feet flat, heels together, legs straight ¨ Arm span: with arms at right angles, distance from tip of the middle finger on the right hand to tip of middle finger on the left; does not change with age ¨ Knee height: can be used to measure stature in those unable to stand; there are equations to convert knee height to stature
Commonly Used Weight Standards ¨ NHANES (%ile or IBW or DBW) ¨ Hamwi (% IBW or DBW) ¨ BMI ¨ % ABW/UBW (weight loss)
Hamwi ¨ Population: small group of people with diabetes; desirable weight related to best blood glucose control ¨ Advantage: Portable and easy to use ¨ Disadvantage: no evidence this is predictive of morbidity/mortality in general or in hospitalized population Hamwi GJ. Changing dietary concepts. In: Donowski TS, ed. Diabetes Mellitus: Diagnosis and Treatment. New York, NY: American Diabetes Association, 1964; 73 -78.
Metropolitan Height/Weight Tables ¨ Population: 4. 2 million mostly Caucasian policy holders; upper socio-economic class. ¨ Advantages: desirable wt associated with lowest morbidity/mortality in this population ¨ Disadvantages: may not apply to different socio-economic classes; requires frame size measurement and reference to a table; data gathering methods poorly controlled; data collected 1954 -1972
NHANES DATA ¨ Population: U. S. Population over time; generally percentiles <5 and >95 are considered to be at risk. 50 th percentile is median ¨ Advantages: more rigorous data gathering methodology; can be normed to age, sex, race, socio-economic class etc. ¨ Disadvantages: Americans are growing larger; median is not necessarily a healthy weight
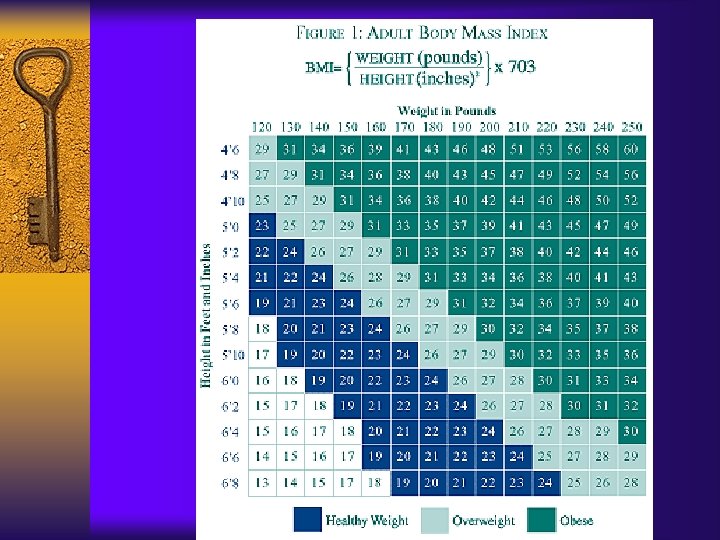
NIH BMI Classification ¨ Population: NHANES data has been collected in general population; many RCT use BMI to describe height-weight relationships ¨ Advantage: Strong evidence from RCT and epidemiological studies demonstrating relationship between BMI classification and risk for morbidity and mortality ¨ Disadvantage: Paucity of evidence showing BMI predicts risk in an acute care population
Calculating BMI (Quetelet Index) ¨ BMI = Weight (kg) divided by (height [m]2) OR ¨ BMI = (Weight in Pounds x 703 (Ht/in) x (Ht/in)
“Ideal” Body Weight vs “Usual” Body Weight ¨ Ideal weight for height (IBW) from standards like NHANES and Metropolitan ht/wt tables (and Hamwi) is no longer used —Hammond in K&M, p. 400 ¨ However, IBW IS often used, whether evidence-based or not ¨ Usual body weight is more useful in those who are ill
What is “Desirable” Weight in Men? Wt in Kg
Weight Status as a Predictor of Morbidity and Mortality ¨ In young to middle aged adults, morbidity/ mortality is highest in the highest quintile of BMI ¨ In the elderly, morbidity/mortality is highest in the lowest quintile of BMI ¨ In most populations, there is a U-shaped relationship between mortality and BMI
Weight Status as a Predictor of Morbidity and Mortality ¨ Mc. Clave et al found that “marasmic PCM” defined as <90% “IBW” was not predictive of poor outcome in acute care pts receiving TPN (JPEN 16: 337. 1002) ¨ Weight loss and unintentional weight loss is strongly predictive of morbidity/mortality, particularly in the elderly. It is unclear whether this is a nutritional issue
Evaluation of Weight Loss ¨ Significant weight loss: 5% loss in 1 month; 7. 5% loss in 3 months; 10% loss in 6 months ¨ Severe weight loss: >5% loss in 1 month; 7. 5% loss in 3 months, >10% weight loss in 6 months Blackburn GL et al. Nutritional and metabolic assessment of the hospitalized patient. J Parent Ent Nutr 1: 11, 1977
Evaluation of % Usual Body Wt ¨ 85 -90% of usual weight: mild malnutrition ¨ 75 -84% of usual weight: moderate malnutrition ¨ <74% of usual weight: severe malnutrition Buchman AL: Handbook of nutritional support, Baltimore, 1997, Williams & Wilkins, cited in Hammond in Krause, p. 434
Weight Issues in Clinical Settings ¨ Accuracy and reproducibility of weights taken on different scales and by different personnel ¨ Weights of critically ill patients may be unavailable on admission; sometimes heights are not measured ¨ Fluid status ¨ Accuracy of weight history data from patients and family members ¨ Confounding factors (wheelchairs, splints, casts, clothing, amputations) ¨ Question of dosing weight: actual, usual, ideal, adjusted? ? ?
Anthropometrics in Pediatrics ¨ Recumbent length measurements used for children younger than 2 or 3 years of age; recorded on birth -to-36 month growth grids ¨ Standing heights of children age 2 or 3 should be recorded on the 2 -20 years growth grids ¨ Rate of length or height gain reflects long-term nutritional adequacy ¨ Head circumference: used to evaluate growth in children <3 years of age; usually detects nonnutritional abnormalities
Weight in Pediatrics ¨ A more sensitive measure of nutritional adequacy than height, and reflects recent nutritional intake ¨ Provides crude evaluation of fat and muscle stores
Measurement of the Length of an Infant
Body Composition: Skinfold Thickness (subcutaneous fat) ¨ Validity depends on measurement technique and repetition over time ¨ Changes take 3 to 4 weeks ¨ Accuracy decreases with increasing obesity ¨ Skinfold sites most reflective of body fatness are over the triceps and the biceps, below the scapula, suprailiac, and upper thigh
Body Composition: Circumference measurements ¨ Waist circumference: smallest area below the ribcage and above the umbilicus; measurements >40 for men and >35 for women are risk factors for disease ¨ Mid arm circumference (MAC) in combination with TSF can determine arm muscle area (lean body mass)
Fatfold Measurements
Skinfold Calipers Measure Thickness of Subcutaneous Fat in Millimeters Courtesy Dorice Czajika-Narins, Ph. D
Other Methods of Body Composition ¨ Underwater weighing ¨ Total body potassium ¨ Neutron activation analysis ¨ BIA: fat free mass and fat mass ¨ CT: subcutaneous and intraabdominal fat ¨ MRI: size of skeleton and internal organs; abdominal fat ¨ DEXA: dual-energy x-ray absorptiometry; bone mineral density and fat and boneless lean tissue
Visceral Protein Status
Evaluation of Visceral Protein Status ¨ Affected by numerous other factors, including hydration status, chronic illness, acute phase response ¨ May have low sensitivity/specificity ¨ However, low serum albumin and acute phase proteins are associated with increased complications and length of stay in hospitalized patients; probably an index of severity of illness
Preoperative Albumin as a Predictor of Risk in Elective Surgery Patients ¨ Retrospective review of 520 patients with preoperative serum albumin measurements ¨ Preoperative albumin correlated inversely with complications, length of stay, postoperative stay, ICU stay, mortality, and resumption of oral intake ¨ S. albumin levels <3. 2 were predictive of risk – Kudsk et al, JPEN, 2003
Role of Visceral Protein Measurement in Nutrition Screening and Assessment ¨ Low values in critically ill patients a measure of severity of illness ¨ Is a valuable predictor of morbidity/mortality in hospitalized and LTC patients ¨ Can be used to identify elective surgery patients who could benefit from nutrition intervention ¨ Sequential measurements may reflect changes/improvement of nutritional status
Nutrition-Focused Physical Examination ¨ Physical signs: using inspection, palpation, percussion, auscultation ¨ Immune function: skin testing and TLC; not always useful for hospitalized patients ¨ Handgrip dynamometry: measures muscle function; useful for serial measurements ¨ Biochemical analysis
Classifying Malnutrition (determination of ICD-9 codes) ¨ Body weight ¨ Body fat ¨ Somatic and visceral protein stores ¨ Laboratory values
More Research Needed ¨ More data needed to evaluate sensitivity/ specificity of nursing screening systems ¨ More research needed to validate nutrition assessment parameters in clinical settings ¨ More data needed to evaluate whether nutrition intervention is helpful in patients identified to us ¨ The Joint Commission requirements for nutrition screening and assessment are critical in keeping nutrition care front of mind among nurses and administrators
Estimation of Energy and Protein Needs
Harris-Benedict Equation ¨ Monograph in 1919 described results of indirect calorimetry on 239 healthy men and women of varying body sizes up to a BMI of 56 in men and 40 in women ¨ Predicts BMR (RMR) with systematic overestimation of 5 -15% (1) ¨ Random error greater in women than in men ¨ Stress and activity factors must be applied to estimate total energy expenditure 1. Daly JM, Helmsfield SB, Head CA, et al. Human energy requirements : overestimation by widely -used predictive equations. Am J. Clin Nutr 1985; 42: 1170 -1174.
Harris Benedict Equation (HBE) ¨ Men = 66. 47 + (13. 75 x wt in kg) + (5 x ht in cm) – (6. 76 x age) ¨ Women = 655. 1 + (9. 56 x wt in kg) + (1. 85 x ht in cm) – (4. 68 x age)
Stress Factors for Use with HBE ¨ Elective surgery 1. 0 – 1. 1 X BEE ¨ Multiple bone fx 1. 1 – 1. 3 X BEE ¨ Cancer 1. 1 – 1. 45 X BEE ¨ Fever 1. 2 X BEE per 1 C >37 C ¨ Sepsis 1. 2 – 1. 4 X BEE ¨ Severe infection 1. 2 – 1. 6 X BEE ¨ Closed head injury 1. 3 X BEE ¨ Infection with trauma 1. 3 – 1. 55 X BEE Elwyn DH et al. Surg Clin N Am 1981; 61: 545 -556; Souba WB et al. In Shils ME. Modern Nutrition in Health and Disease, 9 th ed. Baltimore, MD: Williams & Wilkins, 1999; Sax HC et al. In The ASPEN Nutrition Support Practice Manual Silver Springs, MD: ASPEN, 1998, 1 -5. Cited in ADA Manual of Clinical Dietetics, 6 th edition.
Activity Factors for Use with REE ¨ Hospitalized and critical illness ¨ Chair or Bed-Bound ¨ Seated work with little movement and little or no leisure activity ¨ Seated work with requirement to move but little strenuous leisure activity ¨ Standing work ¨ Strenuous work or highly active leisure activity ¨ 30 -60 minutes strenuous leisure activity 4 -5 times a week 1. 05 -1. 1 1. 2 x BEE 1. 4 -1. 5 x BEE 1. 6 -1. 7 x BEE 1. 8 -1. 9 x BEE 2. 0 -2. 4 x BEE AF +. 3 Shetty PS, Henry CJK, Black AE, et a. Energy requirements in adults: an update of basal metabolic rate (BMR) and physical activity levels (PALs). Eur J. Clin Nutr 1996; 50: S 11 -S 23, Frankenfeld et al Crit Car Med 22; 1796: 1994
Dosing Weight ¨ The weight on which nutritional calculations are based ¨ Must consider – Fluid status – Weight vs standard (IBW? SBW? Adjusted wt? )
Adjusted Body Weight ¨ In common use for obese patients ¨ Rationale is that fat is less metabolically active than lean tissue; thus using actual body weight in an obese person will overpredict energy needs ¨ However, studies have shown that in very overweight persons, calculating HBE using the adjusted wt tends to make calculations less accurate; underestimating total energy needs
Adjusted Body Weight ¨ [(ABW – IBW) *. 25] + IBW Alternative equation: ¨ [(ABW – IBW) *. 50] + IBW – Barak N, et al. Evaluation of stress factors and body weight adjustments currently used to estimate energy expenditure in hospitalized patients. JPEN 26: 231 -238, 2001.
What Weight Should We Use to Calculate HBE in Obese Patients? ¨ Use Average of IBW/AW. Glynn CC, et al. JPEN 1999; 23: 147 -154. Barak N at al. Evaluation of stress factors and body weight adjustments currently used to estimate energy expenditure in hospitalized patients. JPEN 26: 231 -238, 2002. ¨ Use actual weight in the HBE equation. Or use obesity-specific equations. Ireton-Jones CS, Turner WW. Actual or ideal body weight: which should be used to predict energy expenditure? JADA 1991; 91: 193 -195. ¨ Use the Mifflin-St. Jeor equation and actual weight for healthy patients (Frankenfeld et al JADA 2003; 103: 1152 -1159)
What Weight Should We Use to Calculate HBE in Obese Patients? ¨ ADA Pocket Guide to Nutritional Assessment. Does not include adjusted body weight. Chicago: The American Dietetic Association, 2004. ¨ ADA Nutrition Care Manual. Does not use adjusted body weight. Online at www. nutritioncaremanual. org ¨ ADA Evidence Library cites maximal underestimation of 42% to overestimation of 25% when using HBE and adjusted body weight
REE Estimates Using Various Equations Healthy Non Obese Pts Mifflin-St. Jeor 82% of estimates are accurate; maximal underestimation 18%; overestimation 15% Harris-Benedict 45 -81% of estimates are accurate; Actual BW errors tend to be overestimates; underestimation 23%; over 42% Owen 73% of estimates are accurate; errors tend to be underestimates; max underestimation 24%; overestimation 28%
REE Estimates Using Various Equations Healthy Obese Pts Mifflin-St. Jeor 70% of estimates are accurate; errors tend to be underestimates; max underestimations 20%; over 15% Harris 38 -64% of estimates are accurate; Benedict errors tend to be overestimates; max Actual BW underestimation 35%; over 57% Harris 26% of estimations are accurate; Benedict errors tend to be underestimates Adjusted BW Max underestimation 42% to overestimation 25% ADA EAL NCP accessed 12 -07
Recommendations for Predicting RMR in Critically Ill Pts ¨ HBE should not be used to predict RMR in critically ill patients (Grade I) ¨ Ireton-Jones 1997 should not be used to predict RMR in critically ill patients (Grade II) ¨ Ireton-Jones 1992 may be used to predict RMR in critically ill pts but errors will occur. (Grade III) – ADA Evidence Analysis Library, 12 -07
Ireton-Jones 1992 Equations Spontaneously-breathing patients: ¨ IJEE (s) = 629 – 11(A) + 25(W) – 609 (O) Ventilator-dependent patients: ¨ IJEE (v) = 1925 – 10(A) + 5(W) + 281 (S) + 292 (T) + 851 (B) Frankenfield D, Smith JS, Cooney RN. Validation of 2 approaches to predicting resting metabolic rate in critically ill patients. JPEN 2004; 28(4): 259 -64.
Ireton-Jones Equations Where: ¨ A = age in years ¨ W = weight (kg) ¨ O = presence of obesity >30% above IBW (0 = absent, 1 = present) ¨ G = gender (female = 0, male = 1) ¨ T = diagnosis of trauma (absent = 0, present = 1) ¨ B = diagnosis of burn (absent = 0, present = 1) ¨ EEE = estimated energy expenditure
Advantages of Ireton-Jones ¨ Validated in hospitalized patients with varying conditions (pancreatitis, diabetes, trauma, burns) ¨ No need to apply stress factor ¨ Data are easily obtainable
Mifflin-St. Jeor ¨ Derived from data on 498 healthy subjects (females=247, males=251) ages 19 -78 years ¨ Included normal weight (n=264) and obese (n=234) subjects ¨ REE (males) = 10 x wt (kg) + 6. 25 x height (cm) – 5 x age (years) + 5 ¨ REE (females) = 10 x weight (kg) + 6. 25 x height (cm) – 5 x age (years) - 161
Mifflin-St. Jeor ¨ Best validated of predictive equations in estimating REE in healthy patients ¨ Like HBE, studies were done in healthy patients, so stress factors must be applied if used in medical or surgical patients
Comparison of Prediction Equations with Indirect Calorimetery in Critically Ill Patients ¨ Compared REE measurements by indirect calorimetry with standard predictive equations (Harris-Benedict, Ireton-Jones, Fusco, Frankenfeld) ¨ None of the REEs predicted by the equations correlated well with indirect calorimetry ¨ Mean REEs predicted by Ireton-Jones and Frankenfield were not significantly different, but had low correlation coefficients (r=. 26 and r=. 39, respectively), meaning they predicted poorly in individual patients Flancbaum L, Choban PS, Sambucco S, Verducci J, Burge JC. Comparison of indirect calorimetry, the Fick method, and prediction equations in estimating the energy requirements of critically ill patients. Am J Clin Nutr 1999; 69: 461 -6.
Validation of Equations for RMR in Obese and Non-obese People ¨ Subjects: 130 non-hospitalized volunteers grouped by degree of obesity (BMI 18. 8 to 96. 8) ¨ Resting metabolic rate determined using indirect calorimetry was compared with Harris-Benedict, Harris-Benedict with adjusted body wt in obese persons, Mifflin-St. Jeor, and Owen equations ¨ Main outcome was % of subjects whose calculated metabolic rate differed more than 10% from measured values Frankenfield DC, Rose WA, Smith JS, Cooney RN. Validation of several established equations for resting metabolic rate in obese and nonobese people. J Am Diet Assoc 2003; 103: 1152 -1159
Results ¨ Calculated RMR was 10% different from measured in 22% of subjects using Mifflin; 33% using Harris-Benedict; 35% using the Owen equation; and 74% in obese subjects using adjusted body wt (vs 36% in obese subjects using actual wt) ¨ Mifflin-St. Jeor was accurate in the largest percentage of non-obese and obese healthy individuals Frankenfield DC, Rose WA, Smith JS, Cooney RN. Validation of several established equations for resting metabolic rate in obese and nonobese people. J Am Diet Assoc 2003; 103: 1152 -1159
Penn State Equation ¨ RMR = RMR (healthy) (0. 85) + Ve(33) + Tmax(175) – 6433 ¨ Where RMR = RMR calculated using Harris Benedict equation and actual body weight, Ve is minute ventilation in L/min, and Tmax is maximum body temperature in the previous 24 hours in degrees Centigrade ¨ ADVANTAGE: does not require the application of stress factors; usually does not require activity factor unless the patient is seizing or unusually active; found to be highly correlated with MEE in validation studies – Frankenfeld DC et al. Validation of two approaches to predicting resting metabolic rate in critically ill patients. J Parent Ent Nutr 2004; 28: 259.
In-Class Use of Predictive Equations for EEE and REE ¨ Use actual body weight in calculations in class ¨ Use Mifflin-St. Jeor plus activity factors, if applicable, in ambulatory patients ¨ Use Harris-Benedict with actual weight in hospitalized, stressed patients. Apply stress factors and very small activity factor (1. 05 to 1. 1) – ADA Nutrition Care Manual, www. nutritioncaremanual. org, accessed 1 -06
In-Class Use of Predictive Equations for EEE and REE ¨ Use Ireton-Jones 1992 in patients with burns and trauma where Penn State data not available ¨ Use Penn State equation in the ICU where minute ventilation and temperature available
Indirect Calorimetry ¨ Better estimate in critically ill hypermetabolic patient ¨ The “gold standard” in estimating energy needs in critical care ¨ Can be used in both mechanically ventilated and spontaneously breathing patients (ventilated patients most accurate) ¨ Equipment is expensive and not readily available in many facilities
Indirect Calorimetry ¨ Requires appropriate calibration of equipment, attainment of a steady state for measurement, and appropriate timing of measurement ¨ Requires interpretation by trained clinician ¨ Inaccurate in patients requiring inspired oxygen (Fi. O 2>60%), and with air leaks via the entrotracheal tube cuff, chest tubes or bronchopleural fistula ¨ RQ should be within physiological range of . 67 to 1. 3
Indications for Indirect Calorimetry ¨ Patients with altered body composition (underweight, obese, limb amputation, peripheral edema, ascites) ¨ Difficulty weaning from mechanical ventilation ¨ Patients s/p organ transplant ¨ Patients with sepsis or hypercatabolic states (pancreatitis, trauma, burns, ARDS) ¨ Failure to respond to standard nutrition support Malone AM. Methods of assessing energy expenditure in the intensive care unit. Nutr Clin Pract 17: 21 -28, 2002.
Estimation of Protein Needs ¨ Adult maintenance: 0. 8 -1 g/kg ¨ Older adults: 1 g/kg ¨ Predialysis: 0. 6 -0. 8 based on GFR ¨ Hemodialysis: 1. 1 -1. 4 g/kg ¨ PD: 1. 2 -1. 5 g/kg ¨ Short bowel syndrome: 1. 5 -2 g/kg ¨ Cancer 1 -1. 2 g/kg ¨ Cancer cachexia 1. 2 - 1. 5 g/kg ¨ Obesity, stressed: 1. 52 g/kg IBW ¨ Pregnancy: + 10 g/day ¨ Critical illness: 1. 5 -2 g/kg ¨ Major Surgery: 1. 0 -1. 5 g/kg (Cresci, p. 101) See Chart in ADA Pocket Guide to Nutrition Assessment, p. 159
Estimation of Protein Needs ¨ Use actual weight in estimating protein needs ¨ Use lower end of range in obese patients (BMI>30)
Clinical Standards of Care ¨ Providers in a community or health care organization should develop evidence-based standards for care delivery ¨ This promotes consistency among providers and improved quality of care ¨ Review University of Akron Nutritional Standards of Care