Estimating the date of discharge Getting discharge right


 Assertive Case")

 ‘Passing the baton, a practical guide to")
 & Trust standard The organisation has approved documentation which describes a process")











 conducted a patient study (n")




















 system was")







. Discharge")




- Slides: 56
Estimating the date of discharge; Getting discharge right for patients Liz Lees Consultant Nurse (Acute Medicine) RGN, Dip N, BSc (hons), Dip HSM, MSc. Heart of England NHS Foundation Trust Birmingham
Consists of Heartlands Hospital, Solihull Hospital and in April 2007 Good Hope Hospital Heart of England NHS Foundation Trust is one of 32 Foundation Trusts in England Turnover in excess of £ 230 m One of the top five employers in the area with over 6, 000 staff Serves a population of 0. 5 million Cares for 84, 000 inpatients Treats over 350, 000 outpatients and approximately 140, 000 accident and emergency attendees each year
How does it look? Pre Hospital Intermediate Care Advanced Nurse Practitioners (3) Assertive Case Managers (20) GPWsi Geriatricians Assessment (1) Prevention Crisis support Top up services Night sitters Red Cross ANP, ACM IVT (2) Tracking & case management (3) LOS reduction Accident & Emergency Acute Medicine Unit Deep Dark hole 72 hours To Ad Infiniti !
Today 1. NHS Guidance 2. Some basic parameters of EDD 3. Involvement of the patient & family 4. Standardisation helps 5. Review daily 6. Lead professional 7. Its not just the date, it’s the time too 8. Visual, Verbal and documented systems. 9. Linked to bed management 10. Not an ‘add on’ it is ‘integral to’
National policy: the links Welsh Assembly (2008) ‘Passing the baton, a practical guide to effective discharge planning. Provides practitioners with a useful guide of how to review effective communication skills with patients for discharge planning. Urgent care Pathways for older people with complex needs (2007) Where Hospital is being considered identify specialist in put to reduce LOS, Improve outcomes for complex needs and discharge planning Recipe for care not a single ingredient (Dh, 2006) Using intermediate care facilities to promote faster recovery from illness, while reducing unnecessary admissions, supporting timely simple discharge and maximising independence…. . Achieving timely, simple discharge from Hospital (Dh, 2004) Implementing processes to encourage patient involvement, patient choice, patient information, nurse facilitated discharge and embed systems for
NHSLA (CNST) & Trust standard The organisation has approved documentation which describes a process for managing the risks associated with the discharge of patients and can demonstrate implementation a) Duties b) Specific requirements for each group c) Documentation that will accompany patient d) Information to be given to patients e) Evidence of dates of discharged to be planned in advance f) Process for discharge out of hours g) Process for monitoring compliance with all the above. Unified set of records with evidence of a discharge plan, Named person responsible for discharge Clear audit trail of the patients discharge process
NHSLA –Standards & criterion Governance Competent and capable workforce Safe environment Clinical care aspects Learning from experience Discharge Policy Induction to area Vulnerable adults Plans: ward rounds Incidents Uniform process Training needs analysis Transfer checklists Special needs: Dementia Complaints Records (Checklists) Discharge training Home visits Electronic prescribing Investigations (involve carers) Out of Hours systems Competency process Estimating dates of discharge Information for patients Promote Feedback
Today 1. NHS Guidance 2. Some basic parameters of EDD 3. Involvement of the patient & family 4. Standardisation helps 5. Review daily 6. Lead professional 7. Its not just the date, it’s the time too 8. Visual, Verbal and documented systems. 9. Linked to bed management 10. Not an ‘add on’ it is ‘integral to’
What are inpatient stays hospitals for?
Why do we make it so difficult? Dying Fluctuating Waiting for multiple reviews Indecision Complexity Non conformists Non believers that it makes any difference
Multiphase process Theory of car racing Faster the pace, the further ahead you need to look Activities Theory of constraints Speed of process, speed of slowest step Days Hours
EDD – back to basics “to introduce a simple sustainable process, that every one would understand their contribution and participate in” Discharge Ward round Management plan With patient Bed management Nurse handovers Ward maps
Planning: themes and concept analysis Abstract Empirical Readiness Planning Communication Process Coordination Prediction time 10 9 8 7 6 5 4 3 2 1 0 1 2 3 4 5 6 7 8 9 10 On either side of continuum you must take into consideration patient and organisations perspective
Estimating dates for discharge Centralised system ward consensus – Disparity from degree of variability between different practitioners entering a date. Not about a date - Length of stay, activities and commitment to dates Initiating process and reviewing progress Good nursing handovers Excellent communication Research underway: Abstract / Empirical continuum Paternalistic model Most of all what do you want it to achieve? !
Today 1. NHS Guidance 2. Some basic parameters of EDD 3. Involvement of the patient & family 4. Standardisation helps 5. Review daily 6. Lead professional 7. Its not just the date, it’s the time too 8. Visual, Verbal and documented systems. 9. Linked to bed management 10. Not an ‘add on’ it is ‘integral to’
Patient Quotes …. . . “I was so ill, I thought I was going to die and that was why no-one had told me when I was going home” “It all seems very laid back, once they have got you in, you have to fight to get out”. “I can’t hear what’s said on those Doctors rounds and I don’t know what I have to do anyway” “No-one seems to know – it’s a mystery” Assisting Timely Discharge Toolkit (Do. H, 2004)
Patient complaint letter 2/08 Excerpt: As I was on the way in to visit my mum…. I saw her being wheeled backwards down the corridor. I could not get the Porters attention, when I did, Porter: I don’t know anything, I’ve had a lot of patients to collect today – I’ll drop her off and you can ask the ward nurses. Nurse: oh great you're here - your mum is ready to go home.
Keeping up the momentum In 1998 Henwood (et al) conducted a patient study (n = 3000) Given a copy of discharge plan Told about options of care Carers concerns were considered Given written information 25% 28% 48% 25% In 2005 Acute Trust CNST requirements: Discharge checklists as audit trail Proof of patient involvement in plan of care Written discharge information (on admission)
Patient Discharge Information Booklet “I thought it was very good to get this on the day I was admitted, but a lot of what it said hadn’t really happened up to when I was discharged. ” “I was not sure what I was meant to do with the booklet” “It makes you think about going home – which gives you hope” “I thought there was too much talk of going home - I was even told all about going home the day I came in!”
Today 1. NHS Guidance 2. Some basic parameters of EDD 3. Involvement of the patient & family 4. Standardisation helps 5. Review daily 6. Lead professional 7. Its not just the date, it’s the time too 8. Visual, Verbal and documented systems. 9. Linked to bed management 10. Not an ‘add on’ it is ‘integral to’
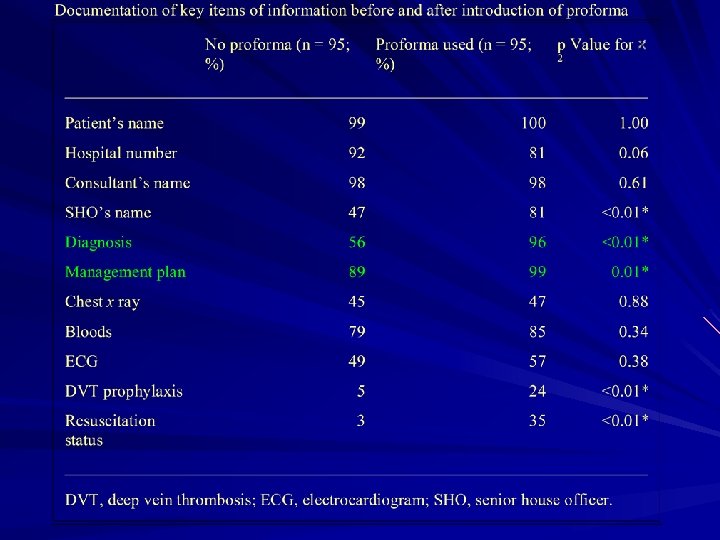
Standardized Proformas Use of a standardized proforma has been shown to improve documentation in many clinical situations Thompson et al looked at the documentation during ward rounds before and after the introduction of a proforma sheet
Specialist vs. Generalist There is evidence that, compared to specialists, hospitalist grade physicians can shorten the length of stay and decrease inpatient costs while maintaining the quality of patient care. So if a generalist can do it so can a specialist if they follow their own protocols
Specialist vs. Generalist Auerbach et al has shown that patients hospitalised with acute heart failure under the care of cardiologists are more likely to undergo invasive procedures such as right heart catheterisation or cardiac catheterisation, than patients admitted under the care of general physicians. At 30 day, however, there was no difference in adjusted survival between the groups
The British Thoracic Society Reviewed within 24 h of planned discharge home should not have more than one of the following characteristics present (unless they represent the usual baseline status for that patient) Temperature >37. 8ºC HR >100/min RR >24/min Systolic Bp <90 mm. Hg O 2 saturation <90% Inability to maintain oral intake and abnormal mental status
Standardized Proformas Led to a significant improvement in: – the documentation of a diagnosis – management plan – prophylaxis for DVT – Resuscitation status
Standardized Proforma
Thompson, A G et al. Postgrad Med J 2004; 80: 675 -676 Copyright © 2004 BMJ Publishing Group Ltd.
Radiology etc Get agreement from your radiology and other departments to honour inpatient dates for tests
Today 1. NHS Guidance 2. Some basic parameters of EDD 3. Involvement of the patient & family 4. Standardisation helps 5. Review daily 6. Lead professional – not have to be a Doctor 7. Its not just the date, it’s the time too 8. Visual, Verbal and documented systems. 9. Linked to bed management 10. Not an ‘add on’ it is ‘integral to’
Estimated date of discharge What & When & Who? What? Duration of acute hospital care When? Earliest opportunity in first 24 hrs: – Diagnosis secure/confirmed (PTWR) – MDT assessments/input to EDD – Feel for: Clinical progress/Medical stability Who? “Member of the ward team responsible for co -ordinating pt journey. . ” - discharge driver
EDD - How? Review Discharge practice - Acute Medicine: 2/12 pilot WARD ROUND-natural time to agree EDD – nurses don’t routinely participate – safari: protracted, many wards (Buddy wards) – requests for investigations haphazard – communication unclear, verbal/written – EDD and criteria for discharge unclear – same day discharge - unnecessary delays (TTOs)
EDD - How? Discharge practice -2/12 Pilot AUDIT MEDICAL NOTES: natural place to record EDD/discharge plans – Management/discharge plans unclear – what is said (on WR) not recorded – discharge documentation difficult to locate – temporary folders, poor filing, missing notes – entries (MDT) vague, no dates/time span
EDD - HOW? Pilot interviews - Patients/Staff Pt passive, optional participation 10/15 no idea of discharge date Pts easily forget - no written information No recap of plans to relieve anxieties/ misunderstandings Staff: no whole picture view, turnover too fast often conflicting discharge opinions no clear responsibility for chasing results critical to discharge information duplicated
EDD - HOW? ? Best practice Generic components: – MDM/WRs - Decision & Revision making – Case Notes Flag point on pathway - traffic lights/DATE Accurate record, pathway trail – Patient centred “informed assent” – Staff engagement
Today NHS Guidance Some basic parameters of EDD Involvement of the patient & family Standardisation helps Review daily Lead professional – not have to be a Doctor 7. Its not just the date, it’s the time too 8. Visual, Verbal and documented systems. 9. Linked to bed management 10. Not an ‘add on’ it is ‘integral to’ 1. 2. 3. 4. 5. 6.
Can Gerry Robinson Fix The NHS? Management guru, Gerry Robinson faces his biggest challenge - to reduce hospital waiting lists. Doctors/Consultants A troublesome lot
EDD – Consultants Perspective Problems/Positives Another weapon to beat us up with Estimate - patients won’t understand Unable to quantify Display/location in notes Requires: Consultation communication Avoids bludgeoning by bed crisis! Improve explanation & involvement Tailor made solutions - focus on discharge Why not? Explore delivery roles/service
Medical School Training - The Background At medical school students the focus of teaching is how to diagnose a condition and the ongoing management Rarely, they are taught how to rule out a condition or the criteria for admission or discharge. Thus the focus of the newly qualified doctor is to admit a patient to confirm a diagnosis rather than to establish whether the diagnosis is likely or not and whether the patient requires admission. This thought process continues throughout their medical career
Reluctance to conform Moloney et al found the hospital in-patient enquiry (HIPE) system was very powerful in predicting differences between hospital consultants in length of stay, re-admission rates, resource utilisation and disease coding. Data relating to emergency medical patients admitted to St James’ Hospital between 1 January 2002 and 31 October 2003
Today NHS Guidance Some basic parameters of EDD Involvement of the patient & family Standardisation helps Review daily Lead professional – not have to be a Doctor 7. Its not just the date, it’s the time too 8. Visual, Verbal and documented systems. 9. Linked to bed management 10. Not an ‘add on’ it is ‘integral to’ 1. 2. 3. 4. 5. 6.
As seen on CCTV! 30 minutes of my shift left. Only 4 staircases to go!
Today NHS Guidance Some basic parameters of EDD Involvement of the patient & family Standardisation helps Review daily Lead professional – not have to be a Doctor 7. Its not just the date, it’s the time too 8. Visual, Verbal and documented systems. 9. Linked to bed management 10. Not an ‘add on’ it is ‘integral to’ 1. 2. 3. 4. 5. 6.
The White Board
The Front of the Notes
Verbal – watch the improvement
Checklists Short Easily understandable Used by everyone Flag up variations Make people think Involve the patient
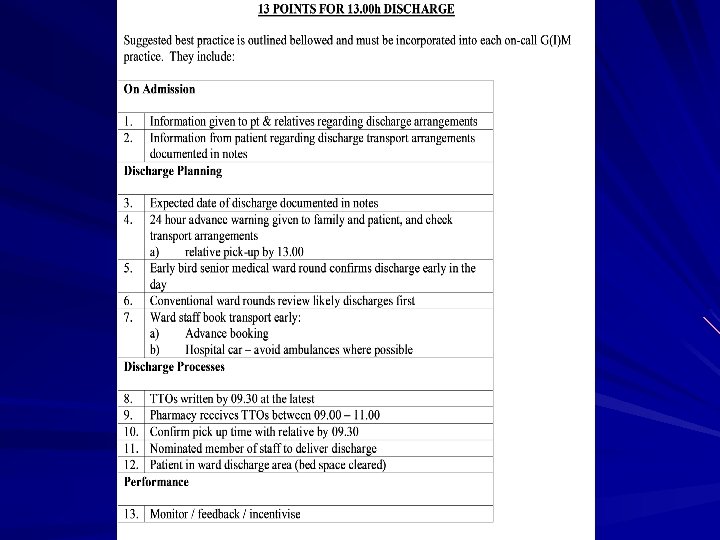
Discharge Checklist Based on Pathway, Process & Practice (Do. H, 2003 update 1994). Discharge From Hospital – good practice checklist (H&S CAT) Incorporate CSNT requirements Takes account of planning (list at 48 & 24 hours) The need to keep evidence of a plan Includes EDD A section for bespoke aspects. Agreed with primary care and social care providers
Today NHS Guidance Some basic parameters of EDD Involvement of the patient & family Standardisation helps Review daily Lead professional – not have to be a Doctor 7. Its not just the date, it’s the time too 8. Visual, Verbal and documented systems. 9. Linked to bed management 10. Not an ‘add on’ it is ‘integral to’ 1. 2. 3. 4. 5. 6.
Bed Management
Go back to the beginning D A T E S
Thank you for listening