Review of Common Radiographs Pneumoperitoneum Air under the








 •")






















 •")



 hyperdense lesion Effacement of ipsilateral ventricle Midline")

- Slides: 56
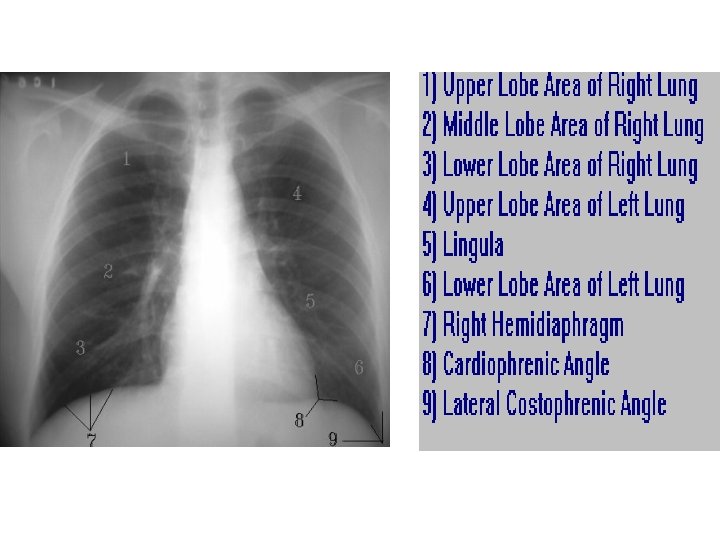
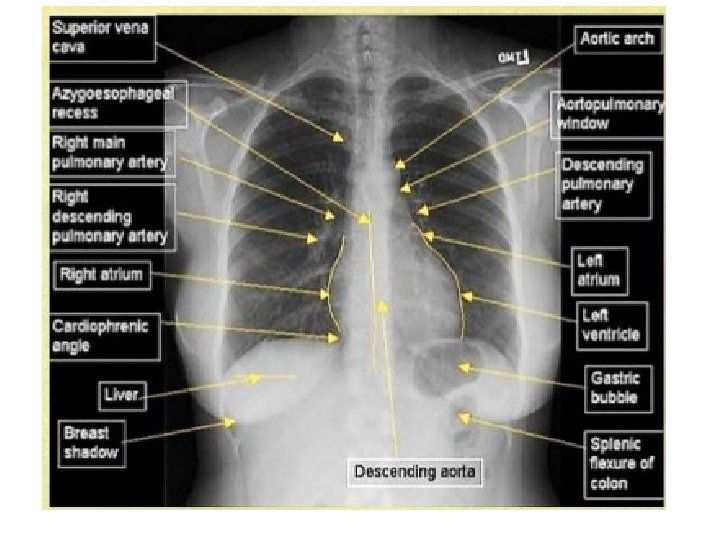
Review of Common Radiographs
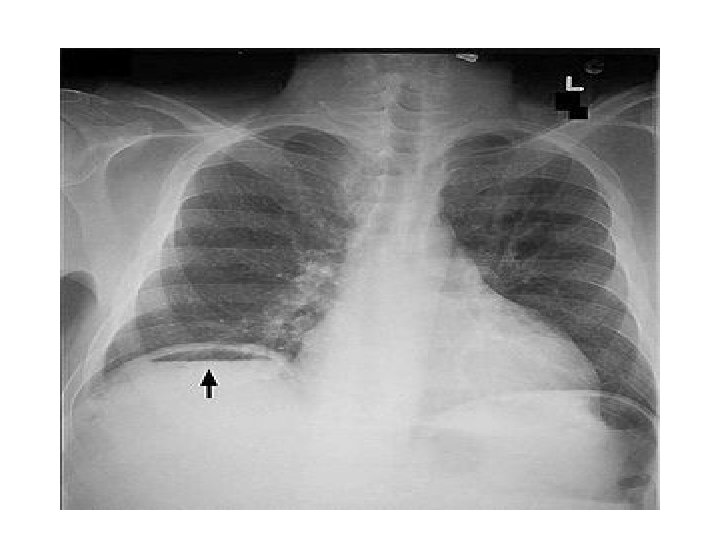
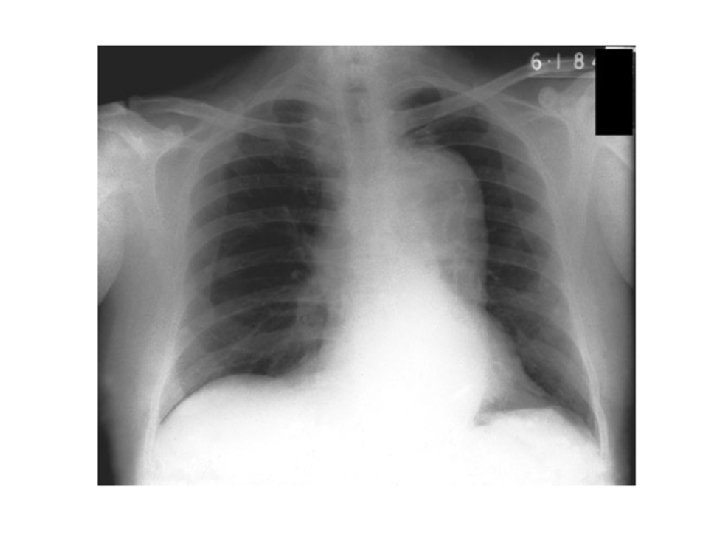
Pneumoperitoneum/ Air under the diaphragm • Erect Chest Xray • Pneumoperitoneum indicates a perforated viscous • Causes : perforated PUD(duodenal ulcer), ruptured appendicitis, typhoid perforation, necrotising enterocolitis, ruptured inflammatory bowel disease, ruptured diverticulitis, bowel cancer, penetrating trauma.
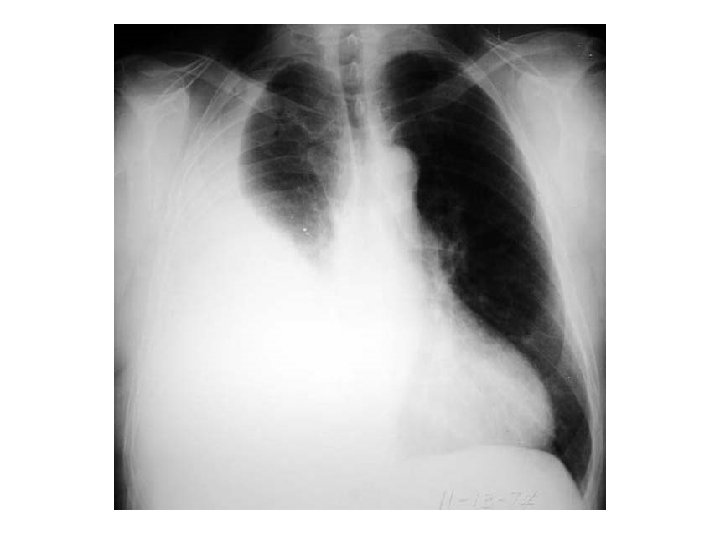
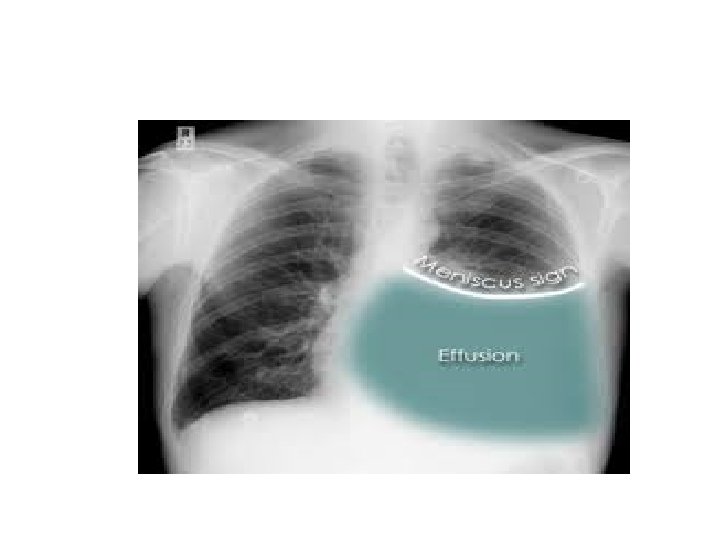
Pleural Effusion • • • Obliteration of the costophrenic angle Obliteration of the cardiophrenic angle Tracheal deviation Meniscus sign Compensatory hyperinflation Causes : heart failure, nephrotic syndrome, cirrhosis, pneumonia, tuberculosis, mesothelioma, bronchogenic CA, SLE, trauma.
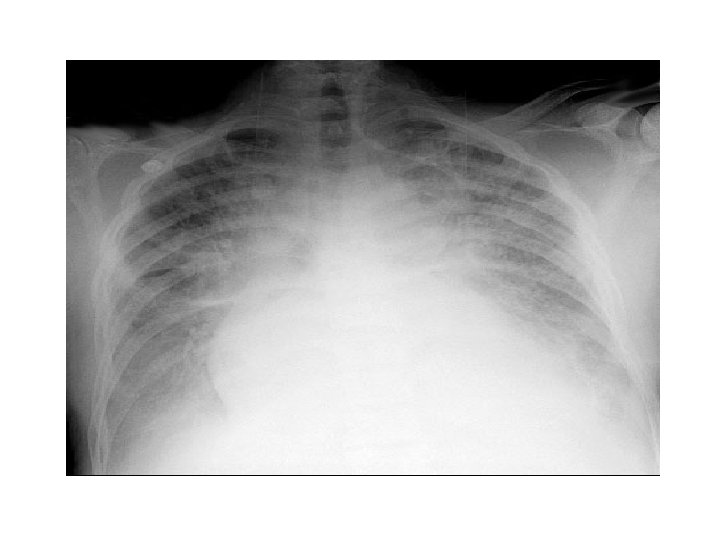
Congestive Cardiac Failure • • • Alveolar oedema Kelly B lines Cardiomegally Upper lobe deviation Pleural Effusion
Cannonball Metastases of the Lungs • • • Causes; Renal cell carcinoma Endometrial carcinoma Choriocarcinoma Prostate cancer
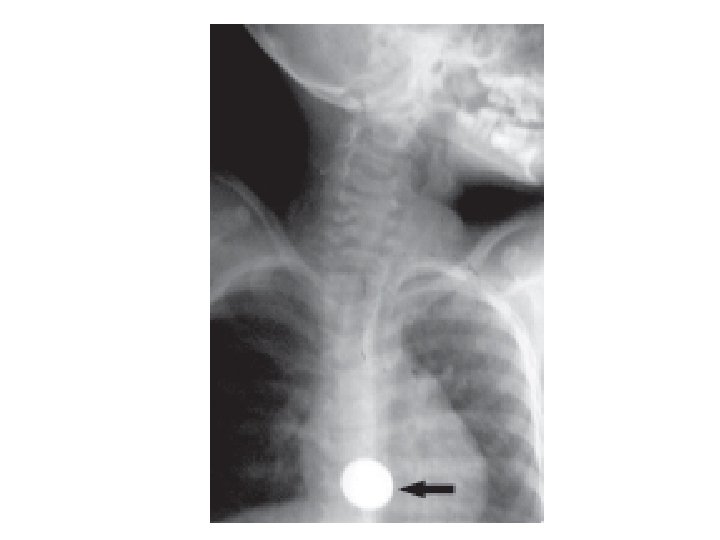
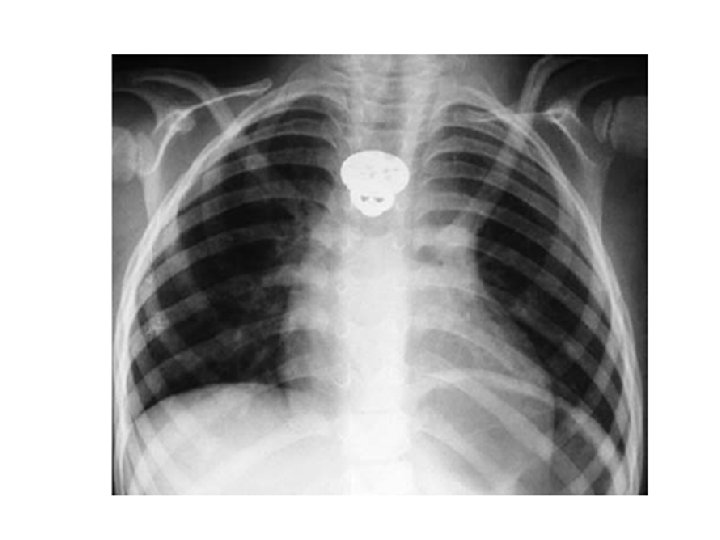
Foreign Body in the Oesophagus • Common sites are the cervical constriction, broncho-aortic constriction and diaphragmatic constriction. • Common foreign object: coin, dentures, bone • Treatment: antibiotics, endoscopic removal, thoracotomy
Widened mediastinium • Diagnostic feature—widened mediastinum (>8 cm at level of aortic knob) • Causes : aortic aneurysm, traumatic aortic rupture, aortic unfolding, mediastinal lymphadenopathy, pericardial effusion
Lobar Pneumonia and Bronchopneumonia • Lobar pneumonia is usually unilateral and involves a lobe • Bronchopneumonia is usually bilateral with patchy reticulonodular opacities.
Lung Cavitation Nodular mass with a central air-filled area Causes: Bronchogenic Ca Pulmonary tuberculosis Lung abscess Pulmonary metastases from breast and GIT tumours • Pulmonary coccidioidomycosis • • •
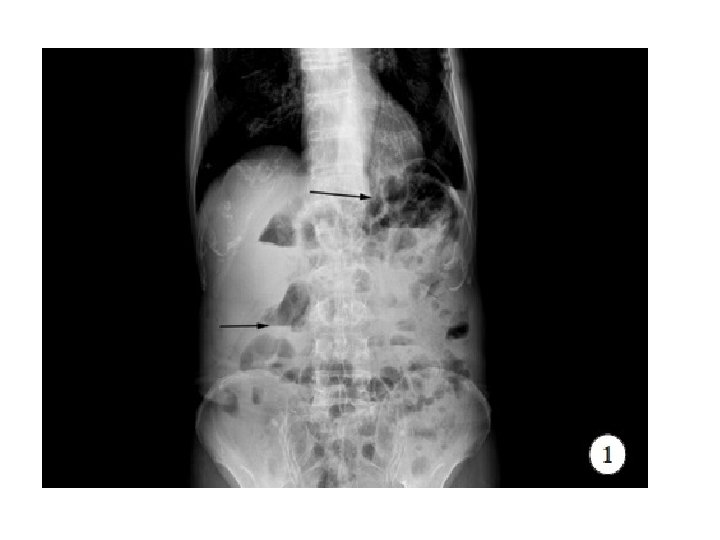
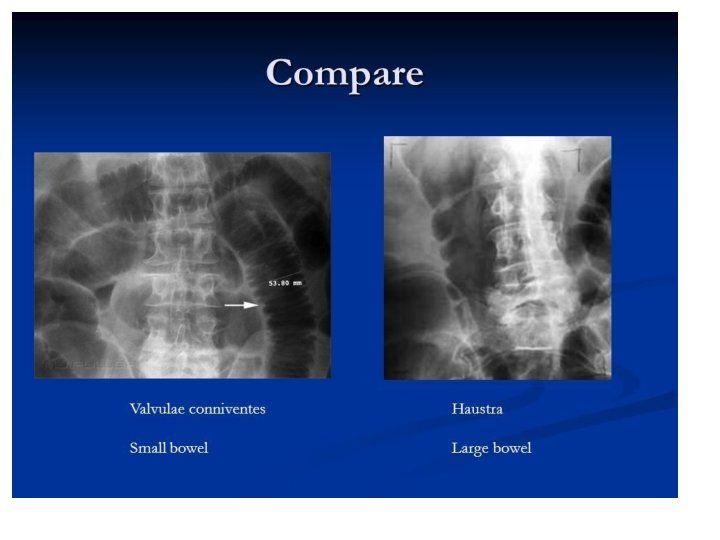
Intestinal Obstruction Supine Xray : Dilated/distended bowel loops Erect Xray : Multiple air-fluid levels Classifications: Based on Site: Small bowel or Large bowel Based on aetiopathology: Mechanical or Funtional • Based on onset : congenital or acquired • • •
Intestinal Obstruction • Congenital: anorectal malformation, intestinal atresia, congenital megacolon, congenital bands and adhesions. • Mechanical Obstruction: hernia, adhesion, volvulus, tuberculous stricture, malignancies, worm infestation, fecal impaction. • Functional Obstruction: electrolyte imbalance, spinal injuries, bowel surgeries.
Chronic Osteomyelitis • • • Involucrum Sequestrum Cortical destruction Periosteal elevation Cloaca Pathological fracture
Chronic Osteomyelitis • Common causes : Staphylococcus aureus, Escherichia coli, Pseudomonas spp, Klebsiella spp, Salmonella spp. • Treatment : antibiotics(clindamycin, flouroquinolones, augmentin), sequestrectomy, saucerization, decortication.
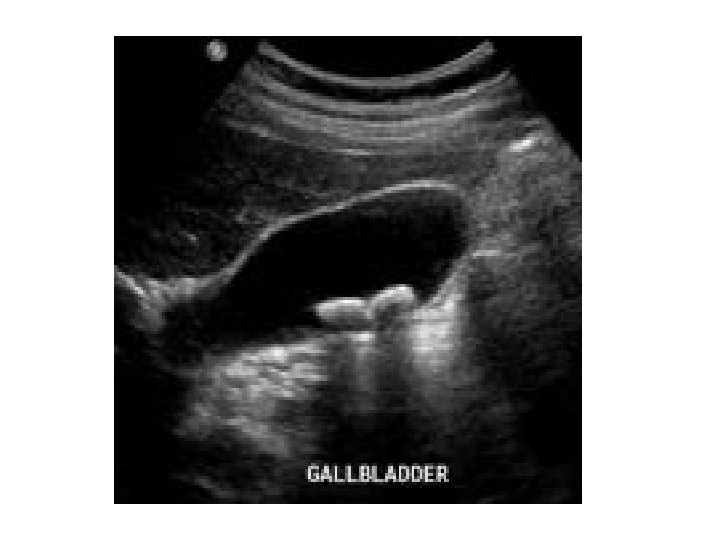
Gallstones • Hyperechoic area casting a posterior acoustic shadow. • Risk factors : obesity, drugs, ileal diseases, ileal resection, parasitic infection(ascariasis) • Cholesterol, Pigment and Mixed gall stones • Cholecystectomy
Kidney Stones • Mostly radiopaque • Calcium, cystine , uric acid and struvite stones • Aetiology : hyperparathyroidism hyperoxaluria, high citrate level, vitamin A deficiency, pyelonephritis, prolonged immobilisation,
Kidney Stones • • Increased fluid intake Medical : Nifedipine, tamsulosin Minimal Invasive surgery : ESWL, PNL Open Surgeries: Open Nephrolithotomy
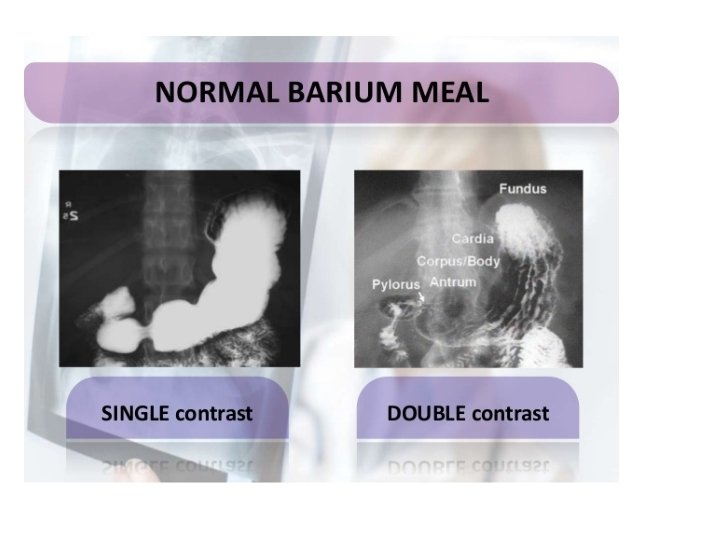
Barium Studies • Barium swallow: used to outline the pharynx and oesophagus. • Barium meal: used to outline the stomach and the first part of the small intestine • Barium follow through: used to outline the small intestine • Barium enema: used to outline the colon
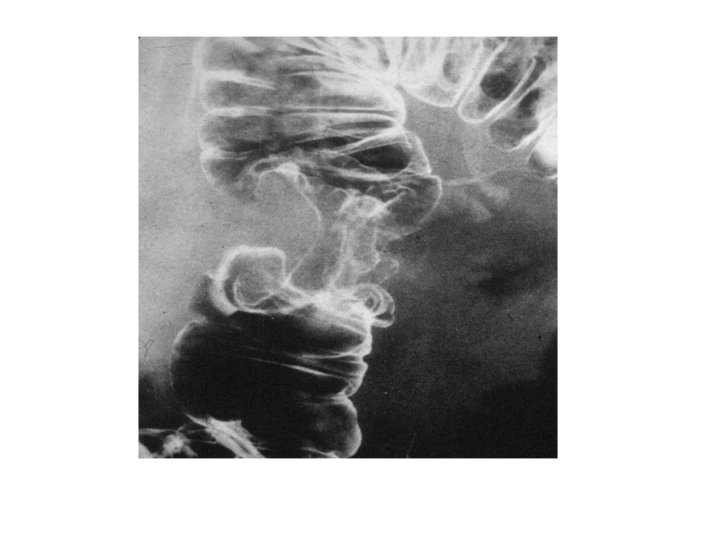
Achalasia • Absent or reduced ganglions within the myenteric plexus • Mostly idiopathic • Can be caused by vitamin B 1 deficiency, Chagas disease and can be congenital • Dysphagia, weight loss, regurgitation • Heller’s procedure
Duodenal Atresia • Commonest intestinal atresia • 1 in 10, 000 live births • Can occur in isolation or with other conditions like – Downs syndrome, – anorectal malformations, – CHD, – annular pancrease
Duodenal atresia • Vomiting, dehydration, jaundice, growth retardation • Fluids, electrolyte correction, nutrition(TPN) • Surgery: Duodenoduodenostomy, duodenostomy.
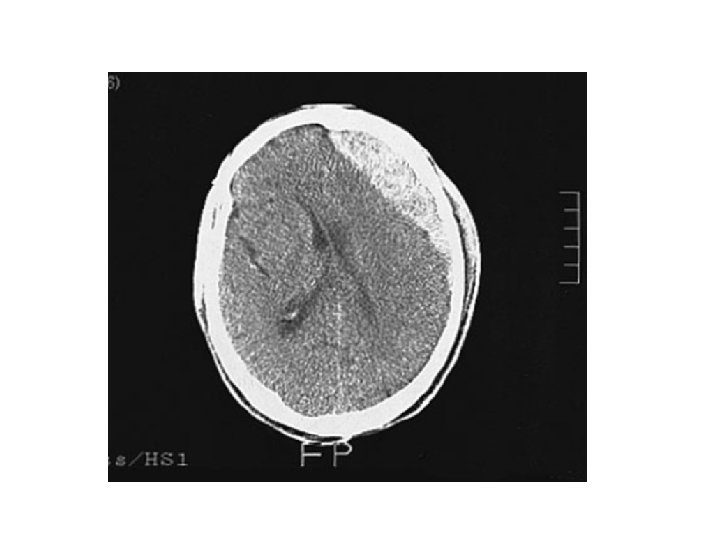
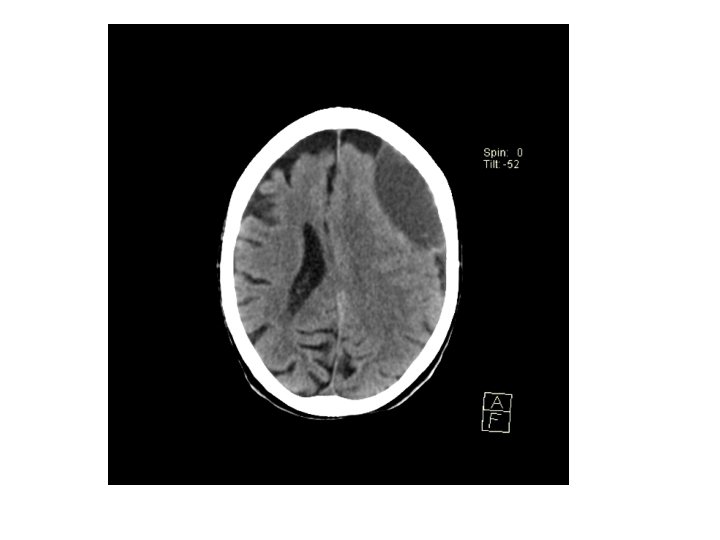
Acute Subdural haematoma • • • Crescentic hyperdense lesion Effacement of the lateral ventricle Midline shift Damage to bridging veins T
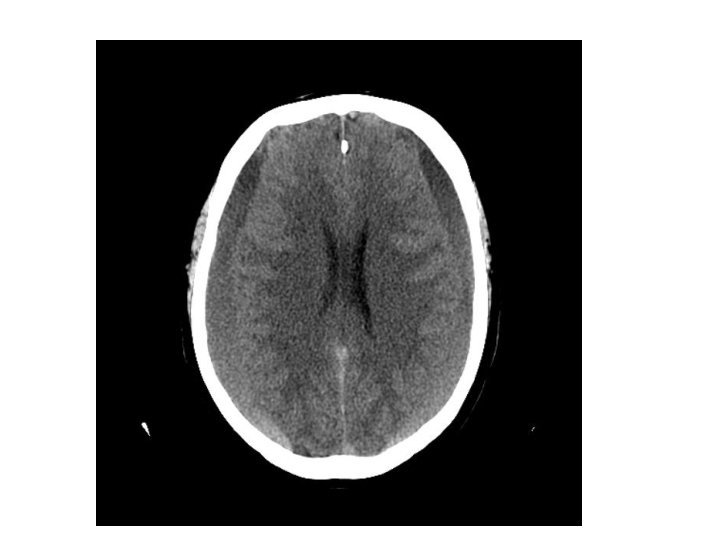
Chronic Subdural haematoma • • Hypodense lesion There might not be midline shift If asymptomatic, serial CT monitoring If symptomatic, burr hole craniostomy
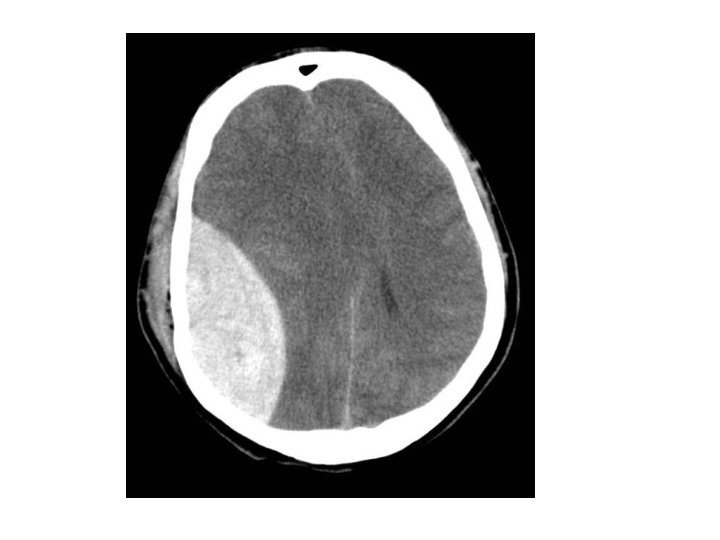
Extradural Haematoma • • • Biconvex(lens shaped) hyperdense lesion Effacement of ipsilateral ventricle Midline shift Lucid interval is a common feature Emergency craniotomy
• Thank You