3 pneumoperitoneum Small bowel obstruction Radiographupright chest or

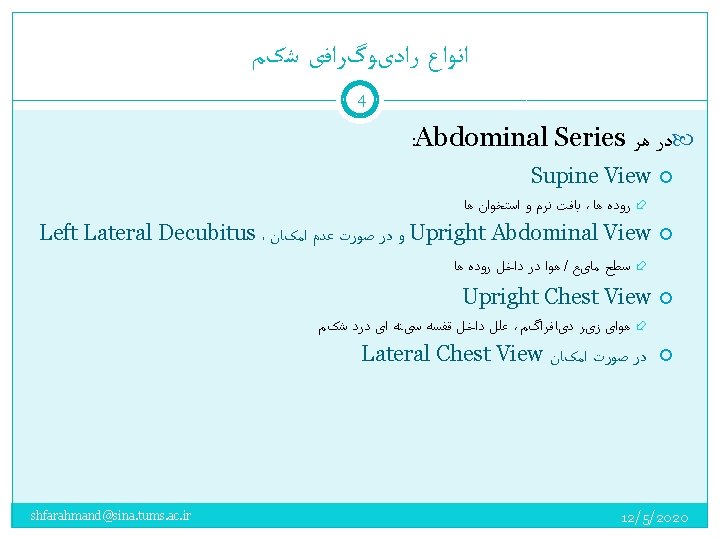
ﻣﻘﺪﻣﻪ گﺮﺍﻓی ﻫﺎی ﻣﻮﺭﺩ ﻧیﺎﺯ ﺑﺮ ﺍﺳﺎﺱ پﺎﺗﻮﻟﻮژی ﻫﺎی ﺍﺣﺘﻤﺎﻟی 3 pneumoperitoneum Small bowel obstruction Radiograph—upright chest or left lateral decubitus abdominal view ; CT (supine and upright); CT (IV contrast, oral ﺗﺼﻮیﺮﺑﺮﺩﺍﺭی ﺍﺭﺟﺢ Radiography—abdomen گﺬﺷﺘﻪ ﺩﺭ ، ﺗﺸﺨیﺼی ﺩﻗﺖ ﺑﻮﺩﻥ ﻣﺤﺪﻭﺩ ﻭﺟﻮﺩ ﺑﺎ contrast not essential); Upper GI contrast study (enteroclysis)—not in ED ﻣﻮﺍﺭﺩ ﻟﺰﻭﻡ ﺍﻧﺠﺎﻡ گﺮﺍﻓی ﺳﺎﺩﻩ ﺩﺭ ﺑﺨﺶ ﺍﻭﺭژﺎﻧﺲ Large bowel obstruction (tumor or volvulus) Radiography; CT (Contrast enema) Intussusception (children) Radiography; ultrasonography; Contrast or air enema—therapeutic (reduces the intussusception) Appendicitis CT, MRI (pregnancy); Ultrasonography (graded-compression technique) Diverticulitis CT Ovarian cyst (bleed or torsion), pelvic abscess Ultrasonography (transvaginal, including Doppler); CT (if enteric disorders are also being considered) Early pregnancy (ectopic) Ultrasonography (transvaginal) Colitis, enteritis No imaging needed for infectious diarrhea; CT for Crohn’s disease or ischemic colitis Mesenteric ischemia CT; angiography for acute arterial occlusion; Emergency surgery, if bowel infarction and peritonitis; Radiography—intramural gas and hepatic portal venous gas (rare) Abdominal aortic aneurysm or dissection Ultrasonography—detects aneurysm, not leakage; CT—noncontrast to detect aneurysm leakage, IV contrast for dissection Renal colic CT—noncontrast to detect aneurysm leakage, IV contrast for dissection; Renal colic Helical CT (noncontrast); radiography (to follow a known stone); Ultrasonography—hydronephrosis, Contrast urography (if no CT) Cholecystitis Ultrasonography; CT; Radiography (gallstones, gallbladder gas); Hepatobiliary scintigraphy (HIDA) shfarahmand@sina. tums. ac. ir Pancreatitis CT—prognostic assessment in severe pancreatitis, complications (pseudocyst), 12/5/2020 negative in mild pancreatitis

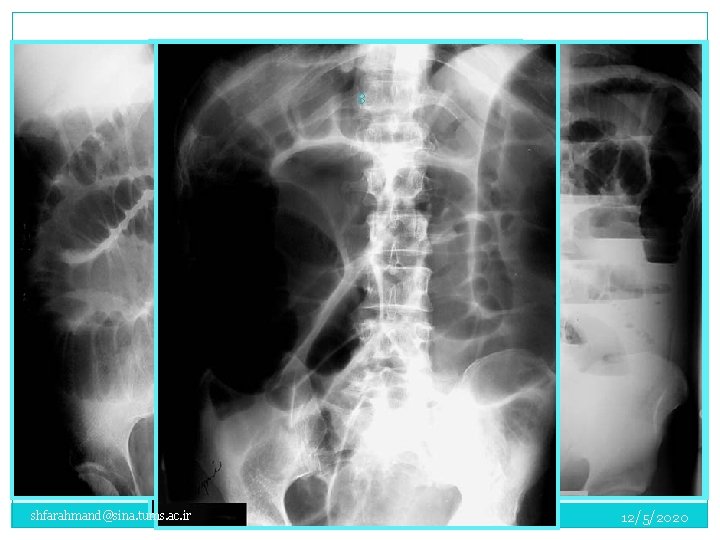

Small Bowel Obstruction 9 shfarahmand@sina. tums. ac. ir 12/5/2020

؛ ﺍﺩﺍﻣﻪ 1 ﺑیﻤﺎﺭ 10 A 50 -year-old man complained of periumbilical and left lower quadrant abdominal pain that began earlier in the day. The pain was intermittent, “crampy” in character, and accompanied by anorexia and vomiting. He had a normal bowel movement the previous day. He had not experienced similar pain in the past. There was no history of prior abdominal surgery. On examination: the patient was afebrile and in moderate distress due to his abdominal pain. Bowel sounds were present, and the abdomen was mildly distended with periumbilical tenderness, but no rebound tenderness. shfarahmand@sina. tums. ac. ir 12/5/2020

؛ ﺍﺩﺍﻣﻪ 1 ﺑیﻤﺎﺭ 11 shfarahmand@sina. tums. ac. ir 12/5/2020
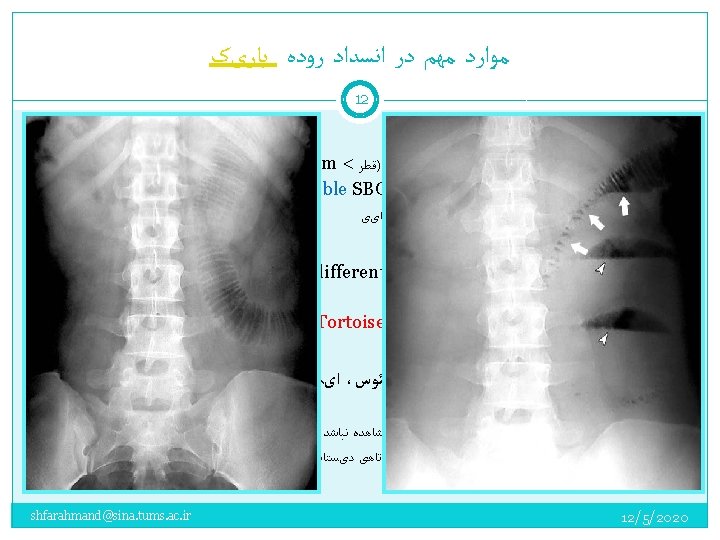

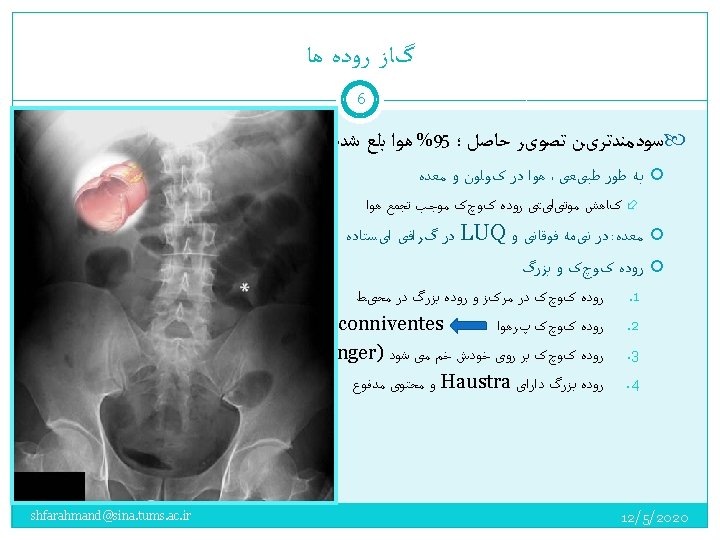
13 shfarahmand@sina. tums. ac. ir 12/5/2020

1 ﺑیﻤﺎﺭ 14 Left Incarcerated Inguinal H. shfarahmand@sina. tums. ac. ir ﻣﺠﺪﺩﺍ ﺑیﻤﺎﺭ ﺩﻗیﻖ ﻣﻌﺎیﻨﻪ ﺷﺪ 12/5/2020

2 ﺑیﻤﺎﺭ 15 shfarahmand@sina. tums. ac. ir 12/5/2020

3 ﺑیﻤﺎﺭ 16 shfarahmand@sina. tums. ac. ir 12/5/2020
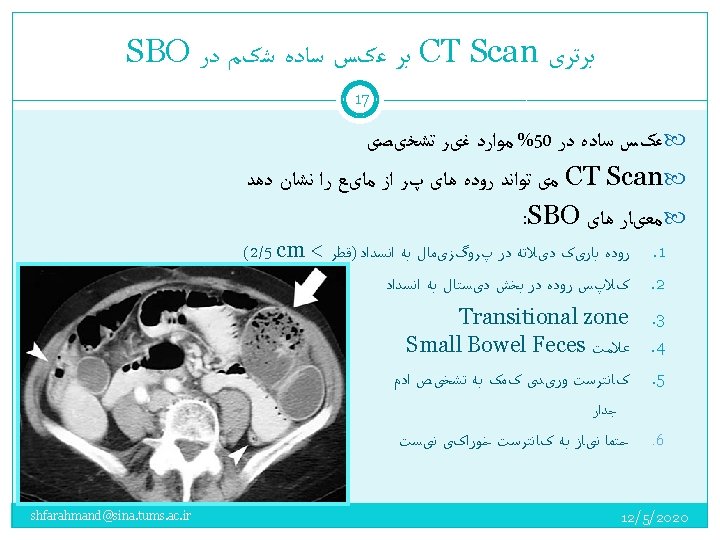

ﺍﺳکﻦ ﺷکﻢ CT 18 shfarahmand@sina. tums. ac. ir 12/5/2020

Large Bowel Obstruction 19 shfarahmand@sina. tums. ac. ir 12/5/2020

3 ﺑیﻤﺎﺭ 20 An 83 -year-old man was brought to the ED by ambulance for progressive shortness of breath of one day duration. On arrival, he was in severe respiratory distress and was unable to provide a detailed medical history. On examination: Vital signs: BP: 150/80 mm Hg PR: 120/min, irregular RR: 36/min; pulse oximetry SO 2 78% on room air. There was poor air movement bilaterally. His abdomen was distended, tympanitic to percussion, and non-tender. Bowel sounds were quiet, but present. The patient stated that he had been constipated for six days, but had a bowel movement the previous day. On 100% oxygen by face mask, the pulse oximetry SO 2 was 92%. ABG: p. H 7. 20, PCO 2 59 mm Hg, 79 mm Hg, PO 2 79 mm Hg The patient was intubated. shfarahmand@sina. tums. ac. ir 12/5/2020

3 ﺑیﻤﺎﺭ 21 shfarahmand@sina. tums. ac. ir 12/5/2020

Coffee Bean 23 Whirl Sign Beard’s Beak shfarahmand@sina. tums. ac. ir 12/5/2020
 24 Sigmoid volvulus Large bowel obstruction— distal Coffee bean—a doubled-back")
Large Bowel Obstruction (LBO) 24 Sigmoid volvulus Large bowel obstruction— distal Coffee bean—a doubled-back and dilated bowel segment Diffuse distention of large bowel and often small bowel Extends from left lower quadrant to right upper Cecum disproportionately quadrant distended (75% of cases) Proximal large bowel dilated Rectum not distended Cecal volvulus Ileus—pseudo-obstruction Single dilated segment (kidney Diffuse distention of colon and shaped) in mid or upper often small bowel abdomen Rectum distended on CT or Distal large bowel collapsed, prone rectal view (air filled) unless concomitant colonic ileus Toxic megacolon Small bowel often dilated Distended colon with focal bowel (effectively obstructed at wall edema (nodularity) terminal ileum) shfarahmand@sina. tums. ac. ir 12/5/2020

Sigmoid Volvulus 25 Coffee bean—a doubled- back and dilated bowel segment Extends from left lower quadrant to right upper quadrant Proximal large bowel dilated shfarahmand@sina. tums. ac. ir 12/5/2020
 in mid or upper abdomen Distal large")
Cecal Volvulus 26 Single dilated segment (kidney-shaped) in mid or upper abdomen Distal large bowel collapsed, unless concomitant colonic ileus Small bowel often dilated (effectively obstructed at terminal ileum) shfarahmand@sina. tums. ac. ir 12/5/2020

Distal LBO 27 Diffuse distention of large bowel and often small bowel Cecum disproportionately distended (75% of cases) Rectum not distended shfarahmand@sina. tums. ac. ir 12/5/2020
 28 Diffuse small and large bowel dilation Without underlying")
Adynamic Ileus (Pseudo – obstruction) 28 Diffuse small and large bowel dilation Without underlying cause; Ogilvie syndrome shfarahmand@sina. tums. ac. ir 12/5/2020
 with clinical sign of systemic toxicity Ulcerative Colitis")
Toxic Megacolon 29 Colonic distention (Megacolon) with clinical sign of systemic toxicity Ulcerative Colitis Infections colitis + Antiparalitic Clostridium D. Amibiasis Shigellosis Distended colon Loss of haustral marking Focal bowel wall edema (nodularity) shfarahmand@sina. tums. ac. ir 12/5/2020

؛ ﺍﺩﺍﻣﻪ 4 ﺑیﻤﺎﺭ 30 A 51 -year-old man presented to the ED with progressive abdominal pain of one day's duration. He had not eaten all day and had vomited twice. There was no associated diarrhea or melena. He had a history of alcoholic hepatitis, COPD, and surgical repair of a colonic-bladder fistula 10 years earlier. He had mild constipation and abdominal discomfort for the past few months. On examination, the patient was in moderate distress due to abdominal pain. Vital signs: BP: 130/70 mm Hg; PR: 118/min; RR: 24/min; temperature 100. 8 ؛ F (rectal). His abdomen was distended but soft, with mild diffuse tenderness and no rebound tenderness. His stool was negative for occult blood. He was anicteric. shfarahmand@sina. tums. ac. ir 12/5/2020

؛ ﺍﺩﺍﻣﻪ 4 ﺑیﻤﺎﺭ 31 shfarahmand@sina. tums. ac. ir 12/5/2020
 ﻫﻤﻪ ﻣﻮﺍﺭﺩ")
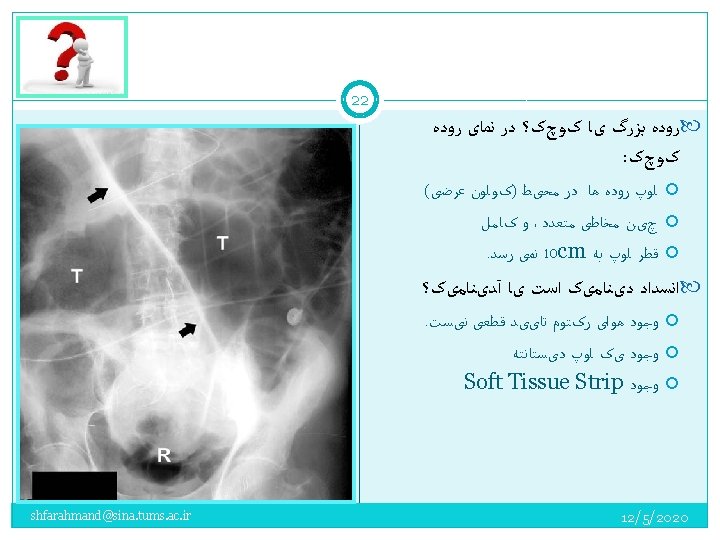
پﻨﻮﻣﻮپﺮیﺘﻮﺋﻦ 32 ﻋﻠﻞ ﺯﺧﻢ پپﺘیک ﺳﻮﺭﺍﺥ ﺷﺪﻩ 80% ( ﺣﺴﺎﺳیﺖ %60) ﻫﻤﻪ ﻣﻮﺍﺭﺩ ﻗﺎﺑﻞ ﻣﺸﺎﻫﺪﻩ ﻧیﺴﺖ pneumatosis cystoides ، ﺍﺯ ﻋﻠﻞ ﻧﺎﺩﺭ intestinalis shfarahmand@sina. tums. ac. ir Perforated peptic ulcer (usually duodenal) Gastric ulcer perforation (benign or malignant) Large bowel obstruction causing cecal perforation Cecal or sigmoid volvulus Perforated appendicitis or diverticulitis (infrequent) Colonoscopy and biopsy Residual postoperative gas Ruptured pneumatosis cystoides intestinalis Extension from pneumomediastinum 12/5/2020

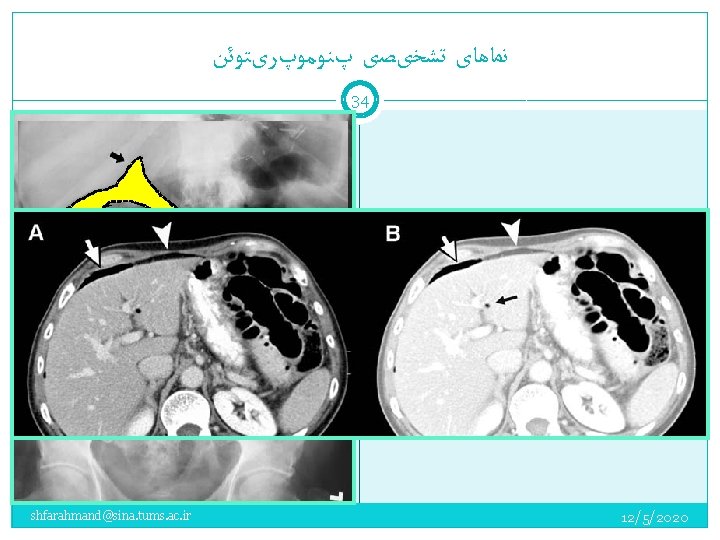
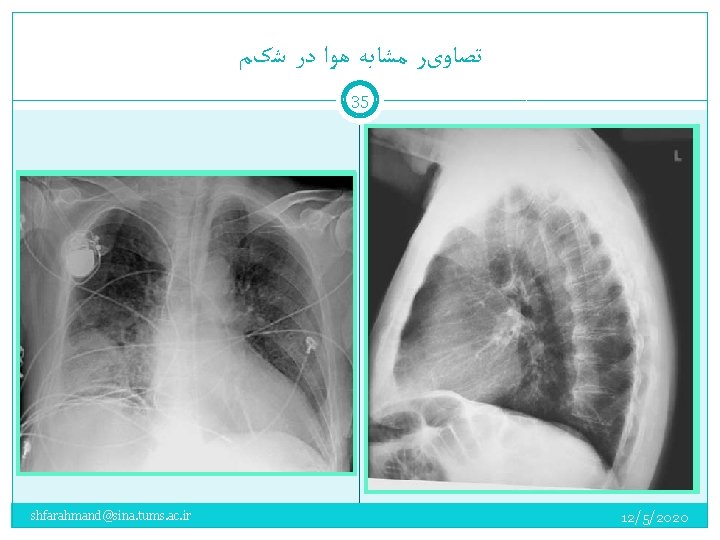
ﻧﻤﺎﻫﺎی ﺗﺸﺨیﺼی پﻨﻮﻣﻮپﺮیﺘﻮﺋﻦ 33 Upright chest radiograph Left lateral decubitus abdominal radiograph Lateral chest radiograph Pneumogastrogram—NG air insufflation Supine abdominal radiograph (massive free air) CT Ultrasonography shfarahmand@sina. tums. ac. ir 12/5/2020

5 ﺑیﻤﺎﺭ 36 A 2 -year-old girl presented to the ED with intermittent abdominal pain that began 18 hours earlier. The previous evening, she had an episode of abdominal pain accompanied by a large bowel movement. During the night and following day, she had several bouts of abdominal pain. Her oral intake was poor and she vomited after eating. Late that afternoon, her mother brought her to the ED. The child had been in good health. At age 4 months, she was brought to the ED for abdominal pain, which resolved over several hours. A medical evaluation at that time was normal. In the ED, her vital signs were: PR: 114/min, RR: 24 min, and temperature 100. 1 F (rectal). The child appeared well. Her abdomen was soft and non-distended. There was minimal right lower quadrant tenderness with no rebound tenderness or palpable mass. Stool was guiac negative. The child would not eat or drink and was admitted to the hospital for observation. shfarahmand@sina. tums. ac. ir 12/5/2020
 on the right side of the")
Intussusception 37 Soft tissue mass (absence of gas) on the right side of the abdomen 2. Crescent sign (the visible head of the intussusceptum) 3. Target sign 4. Small bowel obstruction with dilated loops of airfilled bowel 1. shfarahmand@sina. tums. ac. ir 12/5/2020

پﺎﺗﻮﻟﻮژی ﻫﺎی کیﺴﻪ ﺻﻔﺮﺍ 38 shfarahmand@sina. tums. ac. ir 12/5/2020

ﺍﺳپﻠﻨﻮﻣگﺎﻟی 39 shfarahmand@sina. tums. ac. ir 12/5/2020

40 shfarahmand@sina. tums. ac. ir 12/5/2020
- Slides: 40