Nursing process The Nursing Process An organized sequence







")
 •")













 Health Perception-Health management pattern Nutritional-Metabolic Pattern Elimination Pattern Activity-Exercise Pattern")











. *Risk diagnosis Risk")










 • Withdrawal into the self • Underdeveloped ego; punitive superego")
 • Inaccurate interpretation of environment • Delusional thinking • Hypovigilance")







 **Inability to ingest food due to: • Depressed mood •")
 • Loss of weight • Pale conjunctiva and mucous membranes")







 • Depressed mood • Repressed fears • Feelings of hopelessness")
 • Verbal complaints of difficulty falling asleep • Awakening earlier")


 may be helpful")

- Slides: 70
Nursing process
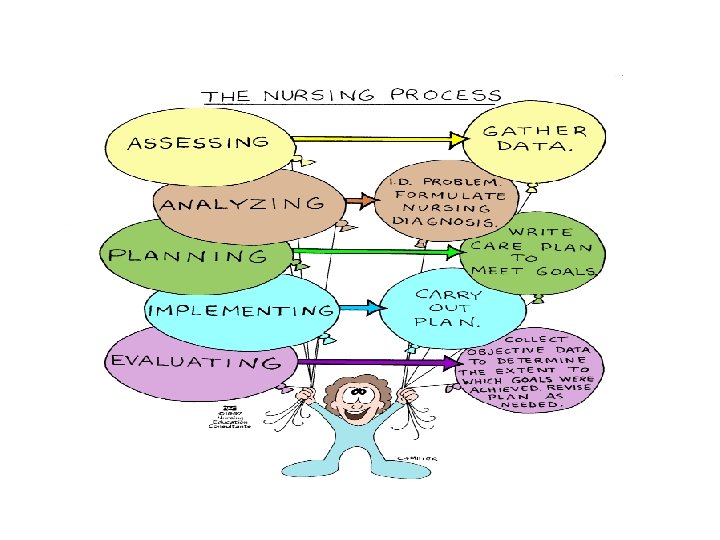
The Nursing Process *An organized sequence of problem solving steps used to identify and to manage the health problems of clients. • Orderly, systematic • Central to all nursing care • Encompasses all steps taken by the nurse in caring for a patient
*Benefits of Nursing Process: • Provides an orderly & systematic method for • • • planning & providing care Enhances nursing efficiency by standardizing nursing practice Facilitates documentation of care Provides a unity of language for nursing profession Is economical Stresses the independent function of nurses Increases care quality by using deliberate actions
Steps of nursing process • Assessment • Nursing Diagnosis • Planning • Implementation • Evaluation
Characteristics of the nursing process • • Within the legal scope of nursing Based on knowledge requiring critical thinking Planned organized and systematic Client centered Goal directed Prioritized Dynamic Continuity of care
Characteristics of nursing process-continued • Prevention of duplication • Individualized care • Standards of care • Increased client participation
Important • Nurses are responsible for a unique dimension of healthcare “the diagnosis and treatment of human responses to actual or potential health problems”. • Critical thinking in nursing is an essential component of professional accountability and quality nursing care. • Critical thinking is careful, deliberate, and goal directed. • Nurse should be understanding the reason behind knowledge. • Nurse is curious, open minded, non judgmental….
ASSESSMENT • Observation • Interview: – Types of questions – Environment (physical and emotional) and spiritual considerations • Examination
*Types of Data to Collect: • Objective data observable and measurable facts (Signs) • Subjective data information that only the client feels and can describe (Symptoms) *Sources of Data: • Primary source: Client • Secondary source: Client’s family, reports, test results, information in current and past medical records, and discussions with other health care workers
* Assessment: • Data base assessment – comprehensive information you gather on initial contact with the person to assess all aspects of health status. • Focus assessment – the data you gather to determine the status of a specific condition.
* Nursing Diagnosis: Health issue that can be prevented, reduced, resolved, or enhanced through independent nursing measures by: • Sorting, clustering, analyzing information • Identifying potential problems and strengths • Writing statement of problem or strength • Prioritizing the problems • Not a medical diagnosis * Nursing Diagnosis: Judgment or conclusion about the risk for—or actual—need/problem of the patient (NANDA format)
Diagnostic Statements: • Name of the health related issue or problem as identified in the NANDA list • Etiology (its cause) • Signs and Symptoms • The name of the nursing diagnosis is linked to the etiology with the phrase “related to, ” and the signs and symptoms are identified with the phrase “as manifested (or evidenced) by” • Problem: (Potential complication of seizure disorder related to medication incompliance) (No AEB) • Problem: (Risk of infection related to compromised nutrition state) (No AEB) • Strength: (Potential for effective breastfeeding related to knowledge level and support system)
*Planning: • The process of prioritizing nursing diagnoses and collaborative problems, identifying measurable goals or outcomes, selecting appropriate interventions, and documenting the plan of care. • The nurse consults with the client while developing and revising the plan. • The nurse shares the plan of care with nursing team members, the client, and client’s family. • The plan is a permanent part of the record. *Setting Priorities: • Determine problems that require immediate action • Maslow’s Hierarchy of Human Needs
Nurse Identified Priorities • Composite of all patient’s strengths and health concerns. • Moral and ethical issues. • Time, resources, and setting. • Hierarchy of needs. • Interdisciplinary planning. • Identifying Client centered outcomes • State what the patient will do or experience at the completion of care. • Give direction to the patient’s overall care. • Patient behaviors not nurse behaviors!!
*Outcome: -Components of Outcomes • Subject: who is the person expected to achieve the outcome? • Verb: what actions must the person take to achieve the outcome? • Condition: under what circumstances is the person to perform the actions? • Performance criteria: how well is the person to perform the actions? • Target time: by when is the person expected to be able to perform the actions?
*Steps for deriving outcomes from Nursing Diagnosis: • Look at the first clause of the nursing dx and restate in a statement that describes improvement, control or absence of the problem. • Risk for infection R/T surgical procedure. • The client will demonstrate no signs or symptoms of infection.
*Short-Term Goals: • Outcomes achievable in a few days or 1 week • Developed form the problem portion of the diagnostic statement • Client centered • Measurable • Realistic • Accompanied by a target date *Long-Term Goals: • Desirable outcomes that take weeks or months to accomplish for client’s with chronic health problems
*Selecting Nursing Interventions: • Planning the measures that the client and nurse will use to accomplish identified goals involves critical thinking. • Nursing interventions are directed at eliminating the etiologies. *Selecting an intervention: • The nurse selects strategies based on the knowledge that certain nursing actions produce desired effects. • Nursing interventions must be safe, within the legal scope of nursing practice, and compatible with medical orders.
*Nursing Interventions: • Monitor health status. • Minimize risks. • Resolve or control a problem. • Assist with ADLs. • Promote optimum health and independence. • Either: • Direct interventions: actions performed through interaction with clients. • Indirect interventions: actions performed away from the client, on behalf of a client or group of clients.
*Evaluation: • The way nurses determine whether a client has reached a goal. • It is the analysis of the client’s response, evaluation helps to determine the effectiveness of nursing care. • Ongoing part of the nursing process • Monitoring the patient’s response to drug therapy • Identifying the variables affecting outcome achievement • Deciding whether to continue, modify, or terminate the plan -Determining Outcome Achievement: • Must be aware of outcomes set for the client. • Must be sure patient is ready for evaluation. • Is patient able to meet outcome criteria? • Is it: (Completely met? , Partially met? , Not met at all? ) • Record in progress in notes. • Update care plan.
*Identifying Variable Affecting Outcome Achievement • Maintain individuality of care plan: 1. Is the plan realistic for the client? 2. Is the plan appropriate at the time for this particular client? 3. Were changes made in the plan when needed? 4. How does the client feel about the plan? *Predict, Prevent, and Manage: • Focus on early intervention • Based on research • Predict and anticipate problems • Look for risk factors
*Documentation • Clear and concise • Appropriate terminology: Usually on a designated form • Physical assessment: Usually by Review of Systems (Overview of symptoms, Diet & Each body system) • Use patient’s own words in subjective data – enclose in “ ___” (quotation marks) • Avoid generalizations – be specific • Don’t make summative statements – describe e. g. patient is being ornery should be patient resists instruction or patient states “Don’t talk to me, I don’t care about that”
Functional Health Pattern (NANDA) Health Perception-Health management pattern Nutritional-Metabolic Pattern Elimination Pattern Activity-Exercise Pattern Sexuality-Reproduction Pattern Sleep-Rest Pattern Sensory-Perceptual Pattern Cognitive Pattern Role-Relationship Pattern Self-Perception-Self- Concept Pattern Coping-Stress Tolerance Pattern Value-Belief Pattern 24
Health Perception-Health Management Pattern Energy Field Disturbance. Altered Growth and Development. Altered Health Maintenance. Ineffective Management of Therapeutic Regimen: Individual. Health Seeking Behaviors Effective Management of Therapeutic Regimen Risk for Injury Risk for diagnoses Risk for Suffocation Risk for Poisoning Risk for Trauma Risk for Peri-operative Positioning Injury
Nutritional-Metabolic Pattern Decreased Adaptive Capacity: Intracranial. Ineffective Thermo regulation. Fluid Volume Deficit Fluid Volume Excess Altered Nutrition: Less than body requirements Altered Nutrition: More than body requirements Ineffective Breastfeeding Interrupted Breastfeeding Ineffective Infant Feeding Pattern Impaired Swallowing Altered Protection Impaired Tissue Integrity Altered Oral Mucous Membrane Impaired Skin Integrity.
Elimination Pattern Altered Bowel Elimination Constipation Colonic constipation Perceived constipation Diarrhea Bowel Incontinence Altered Urinary Elimination Patterns of Urinary Retention Total Incontinence Functional Incontinence Reflex Incontinence Urge Incontinence Stress Incontinence Risk for constipation Risk for altered urinary elimination
Activity- Exercise Pattern Activity Intolerance Impaired Gas Exchange in effective Airway Clearance Ineffective Breathing Pattern Decreased Adaptive Intracranial Capacity Decreased Cardiac Output Disuse syndrome Diversional Activity Deficit Impaired Home Maintenance Management Impaired Physical Mobility Dysfunctional Ventilatory Weaning Response Inability to Sustain Spontaneous Ventilation Self-Care Deficit: (Feeding, Bathing/Hygiene, Dressing/Grooming, Toileting) Altered Tissue Perfusion: (Specify type: Cardiac, Cerebral, and Cardiopulmonary. Renal, Gastrointestinal, Peripheral) Disorganized Infant Behavior Risk for Peripheral Neurovascular Dysfunction Risk for altered respiratory function
Sexuality-Reproduction Pattern Risk- Diagnoses Risk for altered sexuality pattern Actual Diagnoses Sexual Dysfunction, Altered Sexuality Patterns
Sleep-Rest Pattern Wellness Diagnoses: Opportunity to enhance sleep Risk Diagnoses: Risk for sleep pattern disturbance Actual Diagnosis: Sleeps Pattern Disturbance
Sensory-Perceptual Pattern Wellness Diagnosis: Opportunity to enhance comfort level Risk Diagnoses: Risk for pain, Risk for Aspiration Actual Diagnoses: Pain, Chronic Pain and Dysreflexia.
Cognitive Pattern *Actual diagnosis Acute confusion Chronic Confusion Decisional Conflict Impaired Environmental Interpretation Syndrome Knowledge Deficit (Specify) Altered Thought Processes Impaired Memory *Wellness Diagnosis: Opportunity to enhance cognition *Risk Diagnoses: Risk for altered thought processes
Role-Relationship Pattern *Actual Diagnoses Impaired Verbal Communication Altered Family Processes: Alcoholism Anticipatory Grieving Dysfunctional Grieving? Altered Parenting Parental Role Conflict Altered Role Performance Impaired Social Interaction: Social Isolation *Risk Diagnoses Risk for dysfunctional grieving, High risk for Loneliness. Risk for Altered Parent/Infant/Child Attachment
Self-Perception-Self-Concept Pattern *Actual Diagnoses Anxiety fatigue - Fear - Hopelessness- Powerlessness. Personal Identity. Disturbance - Body Image Disturbance- self Esteem Disturbance. Risk Diagnoses Risk for hopelessness Risk for body image disturbance Risk for low self esteem
Coping-Stress Tolerance Pattern *Actual Diagnoses Impaired Adjustment Ineffective Individual Coping Ineffective Family Coping: Disabling Ineffective Family Coping: Compromised Ineffective Community Coping: Post-Trauma Response, Rape-Trauma Syndrome Relocation and Stress Syndrome. *Risk Diagnoses Risk for ineffective coping (individual, family, or community) Risk for self-harm Risk for self- abuse. Risk for Self-Mutilation Risk for suicide Risk for Violence; Self- directed or directed at others
Value-Belief Pattern *Actual Diagnosis Spiritual disturbance (distress of the human spirit). *Risk diagnosis Risk for spiritual distress *Wellness Diagnosis Potential for enhanced spiritual Well- Being
**PRACTICAL STEPS • Perform assessment • Look at the NANDA list • Look for the defining characteristics or symptoms from your assessment • Look for the related factors - things that cause the symptoms • Make the sentence read: NANDA Diagnosis…RT…AEB…
• Develop SMART patient goals or the "patient will" statements – Specific & Individualized – Measurable – Attainable – Reasonable Timed, and a date
• Write nursing interventions • Write rationale that match the intent of the interventions and goals • Evaluate the outcome or result of goal interventions. • More specifically. . . as you begin to write the care plan, refer to your assessment findings. What is the priority problem? Are there clues to the need for patient teaching? What symptoms is the patient experiencing?
• Often it helps to look at the NANDA list first, and see if there is one particular diagnosis that seems to fit the situation. Then look up that diagnosis in the Nursing Diagnosis book. Look at their definition, to see if it fits your patient. Then look for the defining characteristics or evidence: These are the signs and symptoms you have seen in the patient. They will be the "as evidenced by" or AEB of the diagnosis statement.
• Next, look for the related factors: These are the "related to" or R/T part of the statement. Remember, avoid using the medical diagnosis as a "related to" part. However, it may be used as a "secondary to" statement. Then change it around to make the sentence read: NANDA Diagnosis…RT…AEB…
• For example, if my patient has sores on his legs, and he also has Diabetes Mellitus, you might use the statement: Decreased blood flow and nutrients to tissues of the lower extremities, secondary to Diabetes Mellitus AEB a 2 cm skin lesion on the left great toe, and a 4 cm lesion on the inner aspect of the right ankle. "
• Nursing diagnoses that are in the "risk for" categories do not need the AEB portion of the statement, since there is no actual evidence. However, you should avoid using too many "risk for" diagnosis. One or two, out of eight to ten, is acceptable. • Assessment abnormalities should always be reflected in the nursing diagnosis, and subjective and objective data. If the assessment data is not there, you have no evidence. • Gradually, with practice, you will find that nursing diagnoses are easier and easier to develop.
*GOALS or OUTCOMES: • Next you'll want to develop patient goals or the "patient will" statements. These must be specific, measurable, attainable, realistic, timed, and dated. Collaborate with the patient, to gain cooperation with the planned goals. They should also be measurable, and include a time frame, and a date. Goals should conform to the nursing diagnosis. Make them specific to your patient's problem.
• They should be individualized to your patient, not just "canned" from the book. • They should be attainable for your patient. • Then look in the Nursing Diagnosis book for nursing interventions that could be used to assist the patient to attain the goal (s), you have established. • Next, find the rationale that match the intent of the interventions and goals. • And finally, evaluate the outcome of the interventions. These statements should match the wording used in the goal column, and be followed by the statement as to whether the goal was "met, partially met, or not met.
Nursing Care Plan 1 *Nursing Diagnosis: ALTERED THOUGHT PROCESSES *Definition: A state in which an individual experiences a disruption in cognitive operations and activities
*Possible Etiologies (related to) • Withdrawal into the self • Underdeveloped ego; punitive superego • Impaired cognition fostering negative perception of self or the environment
*Defining Characteristics (evidenced by) • Inaccurate interpretation of environment • Delusional thinking • Hypovigilance • Altered attention span distractibility • Egocentricity • Impaired ability to make decisions, problem solve, reason • Negative ruminations
*Goals/objectives **Short-Term Goal • Patient will recognize and verbalize when interpretations of the environment are inaccurate within 1 week. **Long-Term Goal • Patient will experience no delusional or distorted thinking by discharge.
*Interventions with Selected Rationales • Convey your acceptance of patient’s need for the false belief, while letting him or her know that you don’t share the delusion. A positive response would convey to the patient that you accept the delusion as reality. • Do not argue to deny the belief. Use REASONABLE DOUBT as a therapeutic technique: “I find that hard to believe. ” An arguing with the patient or denying the belief serves no useful purpose; delusional ideas are not eliminated by this approach, and the development of a trusting relationship may be impeded.
• Use the technique of CONSENSUAL VALIDATION and SEEKING CLARIFICATION when communication reflects alteration in thinking. (Examples: “Is it that you mean? “or“ I don’t understand what you mean by that. Would you please explain? ”) These techniques reveal to the patient how he or she is being perceived by others, while the responsibility for not understanding is accepted by the nurse. • Reinforce and focus on reality. Talk about real events and real people. Use real situations and events to divert patient away from long, purposeless, repetitive verbalizations of false ideas.
• Give positive reinforcement, as patient is able to differentiate between reality and nonreality based thinking. Positive reinforcement enhances self esteem and encourages repetition of desirable behaviors. • Teach patient to intervene, using thought stopping techniques, when irrational or negative thoughts prevail. Thought stopping involves using the command slop!” or a loud noise (such as hand clapping) to in terrupt unwanted thoughts. This noise or command dis tracts the individual from the undesirable thinking that often precedes undesirable emotions or behaviors.
• Use touch cautiously, particularly if thoughts reveal ideas of persecution. Patients who are suspicious may perceive touch as threatening and may respond with aggression.
*Desired Patient Outcomes/Discharge Criteria 1. Patient’s thinking processes reflect accurate interpretation of the environment. 2. Patient is able to recognize negative or irrational thoughts and intervene to stop their progression.
Nursing Care Plan 2 *Nursing Diagnosis: ALTERED NUTRITION, LESS THAN BODY REQUIREMENTS *Definition: The state in which an individual experiences an intake of nutrients insufficient to meet metabolic needs
*Possible Etiologies (related to) **Inability to ingest food due to: • Depressed mood • Loss of appetite • Energy level too low to meet own nutritional needs • Regression to lower level of development • Ideas of self destruction • Lack of interest in food
*Defining Characteristics (evidenced by) • Loss of weight • Pale conjunctiva and mucous membranes • Poor muscle tone • Amenorrhea • Poor skin turgor • Edema of extremities • Electrolyte imbalances • Weakness • Constipation • Anemias
*Goals/Objectives **Short-Term Goal • Patient will gain 2 Ib per week for the next 3 week. **Long-Term Goal • Patient will exhibit no signs or symptoms of malnutrition by discharge (e. g. ; electrolytes and blood counts will be within normal limits; a steady weight gain will be demonstrated; constipation will be corrected; patient will exhibit increased energy in participation of activities).
*Interventions with Selected Rationales • In collaboration with dietitian, determine number of calories required to provide adequate nutrition and realistic (according to body structure and height) weight gain. • Ensure that diet includes foods high in fiber content to prevent constipation. Encourage patient to increase fluid consumption and physical exercise to promote normal bowel functioning. Depressed patients are particularly vulnerable to constipation due to psychomotor retardation. Constipation is also a common side effect of many antidepressant medications.
• Keep strict documentation of intake, output, and calorie count. This information is necessary to make an accurate nutritional assessment and maintain patient’s safety. • Weigh patient daily. Weight loss or gain is important assessment information. • Determine patient’s likes and dislikes and collaborate with dietitian to provide favorite foods. Patient is more likely to eat foods that he or she particularly enjoys.
• Ensure that patient receives small, frequent feedings, including a bedtime snack, rather than three larger meals. Large amounts of food may be objectionable, or even intolerable, to the patient. • Administer vitamin and mineral supplements and stool softeners or bulk extenders, as ordered by physician. • If appropriate, ask family members or significant others to bring in special foods that patient particularly enjoys.
• Stay with patient during meals to assist as needed and to offer support and encouragement. • Monitor laboratory values, and report significant changes to physician. Laboratory values provide objective data regarding nutritional status. • Explain the importance of adequate nutrition and fluid intake. Patient may have inadequate or inaccurate knowledge regarding the contribution of good nutrition to overall wellness.
*Desired Patient Outcomes/Discharge Criteria 1. Patient has shown a slow, progressive weight gain dur ing hospitalization. 2. Vital signs, blood pressure, and laboratory serum stud ies are within normal limits. 3. Patient is able to verbalize importance of adequate nutrition and fluid intake.
Nursing Care Plan 3 *Nursing diagnosis: SLEEP PATTERN DISTURBANCE • Definition: Disruption of sleep time which causes patient discomfort or interferes with desired lifestyle
*Possible Etiologies (related to) • Depressed mood • Repressed fears • Feelings of hopelessness • Fear of failure • Anxiety, moderate to severe • Hallucinations • Delusional thinking
*Defining Characteristics (evidenced by) • Verbal complaints of difficulty falling asleep • Awakening earlier or later than desired • Interrupted sleep • Verbal complaints of not feeling well rested • Remaining awake 30 minutes after going to bed • Awakening very early in the morning and being unable to go back to sleep • Excessive yawning and desire to nap during the day • Hypersomnia; using sleep as an escape
*Goals/Objectives **Short-Term Goal • Patient will be able to sleep 4 to 6 hours with the aid of a sleeping medication within 5 days. **Long-Terms Goal • Patient will be able to fall asleep within 30 minutes of retiring, and obtain 6 to 8 hours of uninterrupted sleep each night without medication by discharge.
*Interventions with Selected Rationales • Keep strict records of sleeping patterns. Accurate base line data are important in planning care to assist patient with this problem. • Discourage sleep during the day to promote restful sleep at night. • Administer antidepressant medication at bedtime so patient does not become drowsy during the day. • Assist with measures that may promote sleep, such as warm, non stimulating drinks, light snacks, warm baths, backrubs.
• Performing relaxation exercises to soft music (or other technique) may be helpful before sleep. • Limit intake of caffeinated drinks, such as tea, coffee, and coals. Caffeine is a CNS stimulant that may interfere with the patient’s ability to rest and sleep. • Administer sedative medications, as ordered, to assist patient achieve sleep until normal sleep pattern is restored. • For patient experiencing hypersomnia, set limits on time spent in room. Plan stimulating diversionary activities on a structured, daily schedule. Explore fears and feelings that sleep is helping to suppress.
*Desired Patient Outcomes/Discharge Criteria 1. Patient is sleeping 6 to 8 hours per night without med ication. 2. Patient is dealing to fall asleep within 30 minutes of retiring. 3. Patient is dealing with fears and feelings rather than es caping from them through excessive sleep.