Integrative Physiology O 2CO 2 transport disorders Respiratory
















")






















 Disorder of + H excretion H+excretion (4) diarhoea CO 2 HCO")
















")





 Low")



![Measurement of Acid-Base parameters p. H, p. CO 2, [HCO 3 -] HCO 3](https://slidetodoc.com/presentation_image_h/20d111cc48f9af160b9d60a39fb9b35d/image-68.jpg "Measurement of Acid-Base parameters p. H, p. CO 2, [HCO 3 -] HCO 3")
![Measurement of Acid-Base parameters p. H, p. CO 2, [HCO 3 -] HCO 3](https://slidetodoc.com/presentation_image_h/20d111cc48f9af160b9d60a39fb9b35d/image-69.jpg "Measurement of Acid-Base parameters p. H, p. CO 2, [HCO 3 -] HCO 3")
![Measurement of Acid-Base parameters p. H, p. CO 2, [HCO 3 -] Alkaline reserve](https://slidetodoc.com/presentation_image_h/20d111cc48f9af160b9d60a39fb9b35d/image-70.jpg "Measurement of Acid-Base parameters p. H, p. CO 2, [HCO 3 -] Alkaline reserve")
![Measurement of Acid-Base parameters p. H, p. CO 2, [HCO 3 -] P. Astrup](https://slidetodoc.com/presentation_image_h/20d111cc48f9af160b9d60a39fb9b35d/image-71.jpg "Measurement of Acid-Base parameters p. H, p. CO 2, [HCO 3 -] P. Astrup")

![Buffer Base (BB) BB = [HCO 3 ]+ [Buf ] CO 2 depends on](https://slidetodoc.com/presentation_image_h/20d111cc48f9af160b9d60a39fb9b35d/image-73.jpg "Buffer Base (BB) BB = [HCO 3 ]+ [Buf ] CO 2 depends on")









![Siggaard-Andersen BB=[HCO 3 -] +[Buf-] = const HCO 3 - CO 2 Siggaard-Andersen H](https://slidetodoc.com/presentation_image_h/20d111cc48f9af160b9d60a39fb9b35d/image-83.jpg "Siggaard-Andersen BB=[HCO 3 -] +[Buf-] = const HCO 3 - CO 2 Siggaard-Andersen H")

![Siggaard-Andersen (1960 -1962) Definition (for blood in vitro) - Buffer Base: [BB]=[HCO 3 -]+[Buf-]](https://slidetodoc.com/presentation_image_h/20d111cc48f9af160b9d60a39fb9b35d/image-85.jpg "Siggaard-Andersen (1960 -1962) Definition (for blood in vitro) - Buffer Base: [BB]=[HCO 3 -]+[Buf-]")
![Siggaard-Andersen (1974 -1995) Definition (for blood in vitro) - Buffer Base: [BB]=[HCO 3 -]+[Buf-]](https://slidetodoc.com/presentation_image_h/20d111cc48f9af160b9d60a39fb9b35d/image-86.jpg "Siggaard-Andersen (1974 -1995) Definition (for blood in vitro) - Buffer Base: [BB]=[HCO 3 -]+[Buf-]")

 Ca+ K+ Mg+ Na+ HCO 3 - Buf- XA - Cl-")
![Stewart theory – solution of equations [H+]4 + (SID + KBUF) [H+]3 + +(KBUF](https://slidetodoc.com/presentation_image_h/20d111cc48f9af160b9d60a39fb9b35d/image-89.jpg "Stewart theory – solution of equations [H+]4 + (SID + KBUF) [H+]3 + +(KBUF")





























































 Decrease of peripheral resistance Increase")
 Decrease of peripheral resistance Decrease")





































- Slides: 198
Integrative Physiology O 2/CO 2 transport disorders Respiratory disorders Circulation disorders Acid-Base disorders Osmolarity disorders Electrolyte disorders Volume disorders Kidney disorders Gastrointestinal disorders
Homeostasis of internal enviroment Disorders of the acid-base chemistry, influence of respiration, lungs and altered metabolism
Inputs Balance between input and output flow retention Storage ? ? depletion Outputs
External environment of organism Balance estimation Concentrations extracellular fluid - ECF intracellular fluid - ICF Metabolism
External environment of organism Balance estimation Concentrations Lymph plasma capillaries interstitial fluid - ISF intracellular fluid - ICF Metabolism extracellular fluid -ECF
External environment of organism plasma Lymph capillaries interstitial fluid - ISF intracellular fluid - ICF Metabolism intravascular blood cells (part of ICF) fluid extracellular fluid -ECF
External environment of organism plasma Lymph capillaries blood cells capillaries interstitial fluid - ISF intracellular fluid - ICF Metabolism (part of ICF) intravascular fluid extracellular fluid -ECF transcellular fluid
„exchangers“ External environment of organism GIT Lungs Kidney Lymph plasma blood cells capillaries interstitial fluid - ISF intracellular fluid - ICF Metabolism (part of ICF) intravascular fluid extracellular fluid -ECF transcellular fluid
„exchangers“ External environment of organism GIT Kidney Lymph „mixing“ Lungs plasma Circulation blood cells capillaries interstitial fluid - ISF intracellular fluid - ICF Metabolism (part of ICF) intravascular fluid extracellular fluid -ECF transcellular fluid
„exchangers“ External environment of organism GIT Kidney Lymph „mixing“ Lungs plasma Circulation blood cells capillaries interstitial fluid - ISF intracellular fluid - ICF Metabolism (part of ICF) intravascular fluid extracellular fluid -ECF transcellular fluid
Hemodynamics Integrative physiology Volume balance osmotic balance Oxygen transport ionic balance Acid-Base homeostasis
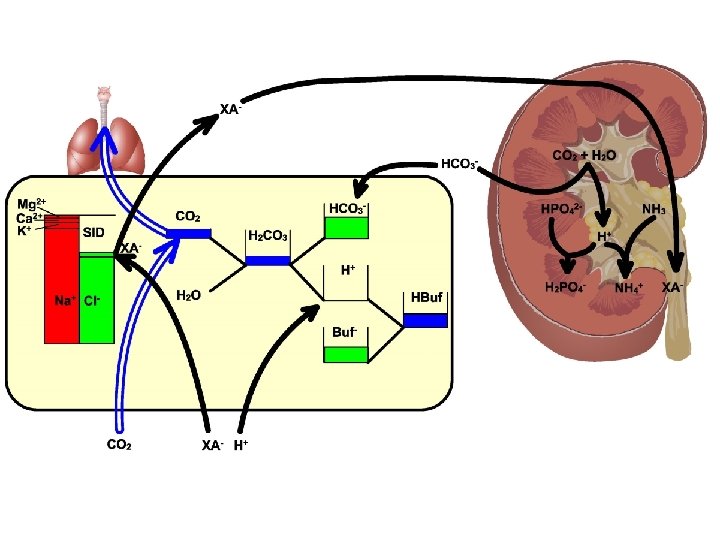
„exchangers“ External environment of organism GIT Kidney Lymph „mixing“ Lungs plasma Circulation blood cells (part of ICF) intracellular fluid - ICF ACID-BASE BALANCE Metabolism fluid extracellular fluid -ECF capillaries interstitial fluid - ISF CO 2 intravascular H+ transcellular fluid
Practically complete reabsorbtion of HCO 3 - Acid-Base Balance H+ excretion 60 mmol/24 h CO 2 HCO 3 H 2 CO 3 TA+NH 4 H H 2 O A + - 20 000 mmol/24 hod Metabolic production of CO 2 - 60 mmol/24 hod Metabolic production od strong acids +
Buffering systems of the blood CO 2 + H 2 O H+ + HCO 3 - H 2 CO 3 H+ + Buf- HBuf H+ + Hb- HHb H+ + Alb- HAlb H+ + HPO 42 - H 2 PO 4 - non-bicarbonate buffers Buf = Hb + Alb + PO 4 -
Buffering reactions HCO 3 - CO 2 H 2 CO 3 H 2 O H+ HBuf Buf-
Acid-Base Balance Acid Balance Base Balance Production of HCO 3 - Production of H+ Diet -> 2 H++SO 42 Diet ->H+ + HPO 4 - Diet -> 3 K++ 3 HCO 3 - Removal of H+ Removal of HCO 3 - Glucose -> 3 H++Citrate- 2 H++2 HCO 3 - -> 2 CO 2+2 H 2 O Excrete organic anions Add „new“ HCO 3 - 2 NH 4++SO 4 H 2 PO 42 - Urine 3 K++Citrate-
H+ formation/removal Reactions that yields H+ (more negative charge in products than in substrates) Glucose -> Lactate- + H+ C 16 fatty acids -> 4 ketoacids anions- + 4 H+ Cysteine -> urea + CO 2+H 2 O+SO 42 - + 2 H+ Lysine+ -> urea + CO 2 + H+ Reactions that removes H+ (more net positive charge in products than in substrates) Lactate- + H+ -> Glucose Glutamate- + H+ -> urea + CO 2+H 2 O Citrate- + 3 H+ -> CO 2+H 2 O H+ are neither produced nor removed (neutrals to neutrals) Glucose -> Glycogen or + CO 2+H 2 O Triglyceride -> CO 2+H 2 O Alanine -> urea + glucose or CO 2+H 2 O
Diet ECF 2 H+ Sulfur-AA 2 CO 2+2 H 2 O 2 HCO 3 SO 42 - urine Glutamine SO 42 - 2 NH 4+ Diet H+ ECF kidney CO 2+H 2 O HCO 3 - RNA-PHPO 42 - CO 2+H 2 O urine HPO 4 - H+ kidney
Diet liver OA utilisation OA- Glucose HCO 3 - H+ OA- ECF K+ CO 2+H 2 O K+ OAurine OA- kidney
Acid-base regulation HCO 3 - CO 2 TA + NH 4+ H 2 CO 3 CO 2 balance H 2 O 1. 2. 3. Buffer systems (msec) Respiration control (12 hours) Kidney control (3 -5 days) H + H+ balance HBuf Exchange H+/K+ H+/Na+ between cells and ECF Role of liver in AB regulation -
Acid-base disturbances: HCO 3 - CO 2 TA + NH 4+ H 2 CO 3 CO 2 balance H 2 O H + H+ balance HBuf Buffer system acid-base disturbances Balance acid-base disturbances: - metabolic acidosis/alkalosis - respiration acidosis/alkalosis Buf -
HCO 3 - CO 2 TA + NH 4+ H 2 CO 3 CO 2 balance H 2 O H + H+ balance Buffers system acid-base disturbances: Dilutional acidemia Contractional alkalemia Hypoproteinemic alkalemia HBuf -
Hemodynamics Integrative physiology Volume balance osmotic balance Oxygen transport ionic balance Acid-Base homeostasis
Alveolar ventilaton pa. CO 2 Cv. CO 2 = Ca. CO 2+VCO 2/Q Ca. CO 2 Perfusion - Q (Cardiac output) By Fick law: VCO 2 = Q (Cv. CO 2 - Ca. CO 2) VCO 2 - CO 2 metabolic production (15 000 -20 000 mmol/24 h Strong acids metabolic production (60 -70 mmol/24 h
Alveolar ventilaton Cv. CO 2 = Ca. CO 2+VCO 2/Q Perfusion - Q (Cardiac output) By Fick law: VCO 2 = Q (Cv. CO 2 - Ca. CO 2) Hypercapnic acidosis in tissues – p. CO 2 Hypoperfusion – Q
Hemodynamics Integrative physiology Volume balance osmotic balance Oxygen transport ionic balance Acid-Base homeostasis
Dilution HCO 3 - CO 2 TA + NH 4+ H 2 CO 3 CO 2 balance H 2 O H + H+ balance Buffers system acid-base disturbances: Dilutional acidemia HBuf -
Dilution CO 2 equilibrium shift HCO 3 TA + NH 4+ H 2 CO 3 CO 2 balance H 2 O H + H+ balance Buffers system acid-base disturbances: Dilutional acidemia HBuf -
Hemoconcentration HCO 3 - CO 2 TA + NH 4+ H 2 CO 3 CO 2 balance H 2 O H + H+ balance Buffers system acid-base disturbances: Contractional alkalemia HBuf -
Hemoconcentration CO 2 HCO 3 TA + NH 4+ H 2 CO 3 CO 2 balance H 2 O H + H+ balance Buffers system acid-base disturbances: Contractional alkalemia HBuf -
Hemoconcentration CO 2 equilibrium shift HCO 3 TA + NH 4+ H 2 CO 3 CO 2 balance H 2 O H + H+ balance Buffers system acid-base disturbances: Contractional alkalemia HBuf -
Hemodynamics Integrative physiology Volume balance osmotic balance Oxygen transport ionic balance Acid-Base homeostasis
Acute hypoproteinemia HCO 3 - CO 2 TA + NH 4+ H 2 CO 3 CO 2 balance H 2 O H + H+ balance Buffers system acid-base disturbances: Hypoproteinemic alkalemia HBuf -
Patogenesis of acute hypoproteinemic alkalosis Liver – albumine production Alb - H+ Endotel, liver – albumine degradation
Patogenesis of acute hypoproteinemic alkalosis Liver – albumine production H 2 O + CO 2 Alb - H+ HCO 3 - -d[Alb-] = d[HCO 3 -] Endotel, liver – albumine degradation no changed value of SID
Acute hypoproteinemia production CO 2 +H 2 O Alb - H+ HCO 3 - HCO 3 - CO 2 degradation TA + NH 4+ H 2 CO 3 CO 2 balance H 2 O H + -d[Alb-] = d[HCO 3 -] no changed value of SID Balance disorders: Hypoproteinemic alkalosis H+ balance HBuf -
Hemodynamics Integrative physiology Volume balance osmotic balance Oxygen transport ionic balance Acid-Base homeostasis
Acid-base disturbances: HCO 3 - CO 2 TA + NH 4+ H 2 CO 3 CO 2 balance H 2 O H + H+ balance HBuf Buffer system acid-base disturbances Balance acid-base disturbances: - metabolic acidosis/alkalosis - respiration acidosis/alkalosis Buf -
is , 3 7 =7 p. H pir ed ain Sus t acidos l bo a t e dm s osi l a lk ic a , 6 p 7 H= Akute metabolic alkalosis Acute metabolic acidosis ed ain t Sus -20 olic b a et si do i c a m d ne r o at ir p es ka l ya r i ta s Su -15 -10 -5 is s lo Acute respiratory acidosi s 10 -25 p ta Sus 30 20 7, 5 = H ine 50 40 p res atory 60 43 7, = H ato respir 70 ry a cid osi s =7, 3 =7, p. H 80 p. H Acute =7, 2 1 90 p. H PCO 2 torr 0 5 10 15 20 25 30 Base Excess mmol/l
Bicarbonate reabsorbtion (2) Disorder of + H excretion H+excretion (4) diarhoea CO 2 HCO 3 H 2 CO 3 + H retention H H 2 O A (3) losses of HCO 3 + TA+NH 4 + H depletion + HBuf - Buf (1) Increased metabolic production of strong acids - -
Cl Anion gap - Urea HCO 3 - Cl Cl- Normal Na+ anion In urine: gap [K+]+[Na+]-[Cl-] < 0 Relative accumulation of chlorides Cl- NH 3 HCO 3 - HCO 3 H+ Na+ - Cl- NH 4+ K+ HCO 3 - Na+ Cl H+ Overdosis of NH 4 Cl Increased anion gap HCO 3 - H+ HCO 3 - Accumulation of anions of strong acids (laktate acidosis ketoacidosis uremic acidosis) Na+ NH 3 Gastrointestinal losses of bicarbonate Metabolic acidosis with: -increased anion gap A-normal anion gap Cl- Decreased acidification HCO 3(tubular acidosis, + hypoaldosteronisms, Cl NH 4 decreases glomer. filtration) K+ Na+ Cl- in urine: [K+]+[Na+]-[Cl-] >= 0
Diarrhoea
Cl. Na+ H+ H 2 O H 20 + CO 2 HCO 3 - H 2 O Colon NHE Na+ AE H+ Cl- H 20 + CO 2 HCO 3 - HCO 3 Na+ Cl. H 2 O HCO 3 -
Cl- H+ H 20 + CO 2 HCO 3 - Na+ H 2 O HCO 3 - H 2 O Na+ H 2 O Colon NHE Na+ AE H+ Cl- H 20 + CO 2 HCO 3 - Hypotonic fluid loss Cl- Na+ HCO 3 - H 2 O Alkalic diarrhoea Hypertonic dehydratation Cl- HCO 3 - Hyperchloremic acidosis
Cl- H+ H 20 + CO 2 HCO 3 - Na+ H 2 O HCO 3 - H 2 O Colon NHE Na+ AE K+ Potassium loss H+ Cl- H 20 + CO 2 HCO 3 - Hypotonic fluid loss Cl- Na+ HCO 3 - H 2 O Severe alkalic diarrhoea Hypertonic dehydratation Cl- HCO 3 - Hyperchloremic acidosis
Histidine Cl- H. Histidine+ H 20 + CO 2 H+ HCO 3 - Na+ H 2 O Cl- H 2 O Colon NHE Na+ AE H+ Cl- H 20 + CO 2 HCO 3 - HCO 3 Na+ Hypotonic fluid loss Cl- HCO 3 - H 2 O Acidic diarrhoea in DRA, down-regulated adenoma Hypertonic dehydratation Cl- HCO 3 Hypochloremic alkalosis
Rate of bicarbonate reabsorbtion on i t rb o s ab norm re Anion gap HCO 3 H+ e let norm p m Co Na+ Cl - proximal tubular renal acidosis b c Normal acidification + Cl NH 4+ a K+ Cl- Normal Na+ urine anion In urine: gap [K+]+[Na+]-[Cl-] < 0 10 15 Hyperchloremic acidosis with normal anion gap HCO 3 - Na+ Cl- 20 Plasma level of HCO 3 - 25 Cl- NH 3 HCO 3 - Cl. HCO 3 H+ normal anion gap Decreased acidification HCO 3(tubular acidosis, + hypoaldosteronisms, Cl NH 4 decreases glomer. filtration) Cl- K+ c b p. H=5, 5 p. H=6, 5 a p. H=7, 8 norm p. H=5, 5 Positive Cl + urine Na In urine: anion [K+]+[Na+]-[Cl-] > 0 gap
Metabolic alkalosis Bicarbonate reabsorbtion Overdosis HCO 3 - infusion CO 2 H+excretion HCO 3 + H 2 CO 3 Retence H H H 2 O A - TA+NH 4 + Retence H + HBuf - hyperaldosteronism katabolism Buf - + (7) K depletion (6) vomiting + H K +
is , 3 7 =7 p. H pir ed ain Sus t acidos l bo a t e dm s osi l a lk ic a , 6 p 7 H= Akute metabolic alkalosis Acute metabolic acidosis ed ain t Sus -20 olic b a et si do i c a m d ne r o at ir p es ka l ya r i ta s Su -15 -10 -5 is s lo Acute respiratory acidosi s 10 -25 p ta Sus 30 20 7, 5 = H ine 50 40 p res atory 60 43 7, = H ato respir 70 ry a cid osi s =7, 3 =7, p. H 80 p. H Acute =7, 2 1 90 p. H PCO 2 torr 0 5 10 15 20 25 30 Base Excess mmol/l
Vomiting
Normal state HCO 3 - Stomach H+ CO 2 Cl- Balanced CO 2 H 2 O Cl- No acid-base changes H+ Cl HCO 3 - H+ CO 2 H 2 O Duodenum and pancreas
Hypertonic dehydratation Chloride H+ loss Cl- H+ loss Hypotonic fluid loss HCO 3 retention Vomitoing HCO 3 - Stomach H+ CO 2 Cl- Unbalanced CO 2 H 2 O Cl- Hypochloremic alkalosis H+ Cl HCO 3 - H+ CO 2 H 2 O Duodenum and pancreas
Na Cl + Primary cause: Losses of Cl- a H+ by vomiting Glomerular filtraton (norm) - Cl H Readsorbtion of sodium and chlorides Na Cl H - NH 4 + H K + + Intracellular fluid Na Cl + - Increased exchange Na+ with K+ and Na+ with H+ + K Potassium depletion + Na + H H + + K Na K+ + H - Glomerulal filtration (hypochloremic alkalosis) Na+/Clreabsorbtion is diminished Metabolic alkalosis Remnant of sodium is exchanged with + and H+ K Cl Depletion of - chlorides + + H Na + Paradoxal urine acidification + K + Increases lossse ofn + Excretion of potassium increases, + acidification of K + urine regardless H of alkalosis +
is , 3 7 =7 p. H pir ed ain Sus t acidos l bo a t e dm s osi l a lk ic a , 6 p 7 H= Akute metabolic alkalosis Acute metabolic acidosis ed ain t Sus -20 olic b a et si do i c a m d ne r o at ir p es ka l ya r i ta s Su -15 -10 -5 is s lo Acute respiratory acidosi s 10 -25 p ta Sus 30 20 7, 5 = H ine 50 40 p res atory 60 43 7, = H ato respir 70 ry a cid osi s =7, 3 =7, p. H 80 p. H Acute =7, 2 1 90 p. H PCO 2 torr 0 5 10 15 20 25 30 Base Excess mmol/l
is , 3 7 =7 p. H pir ed ain Sus t acidos l bo a t e dm s osi l a lk ic a , 6 p 7 H= Akute metabolic alkalosis Acute metabolic acidosis ed ain t Sus -20 olic b a et si do i c a m d ne r o at ir p es ka l ya r i ta s Su -15 -10 -5 is s lo Acute respiratory acidosi s 10 -25 p ta Sus 30 20 7, 5 = H ine 50 40 p res atory 60 43 7, = H ato respir 70 ry a cid osi s =7, 3 =7, p. H 80 p. H Acute =7, 2 1 90 p. H PCO 2 torr 0 5 10 15 20 25 30 Base Excess mmol/l
Arterial blood at p. H=7, 4 Concentration of O 2 Oxygen released due drop PO 2 Oxygen released due to shift of dissotiacion curve (Bohr effect) Venose blood at p. H=7, 2 Pv. O 2 Pa. O 2 PO 2
Release of oxygen at respiratory alkalosis Arterial blood at p. H=7, 4 (normal conditions) Arterial blood at p. H=7, 6 (alkalemia) Concentration of O 2 Release of oxygen at normal condition Venous blood at p. H=7, 36 (alkalemia) Venous blood at p. H=7, 2 (normal conditions) Decrease of oxygen delivery to tissues at acute respiratory alkalosis Pv. O 2 normal Pa. O 2 PO 2 High Pa. O 2 during hyperventilation at respiratory alkalosis
, 3 7 =7 pir ato is ed ain Sus t acidos l bo a t e dm s osi l a lk ic a , 6 p 7 H= Akute metabolic alkalosis Acute metabolic acidosis ed ain t Sus olic b a et si do i c a m d ne r o at ir p es ka l ya r i ta s Su is s lo Acute respiratory acidosi s 10 -25 7, 5 = H p ta Sus 30 20 p ine 50 40 43 7, = H res atory Metabolic acidosis + respiratory acidosis p. H =7, 3 =7, respir 70 60 p. H 80 p. H Acute =7, 2 1 90 p. H PCO 2 torr ry a cid osi s Mixed acid-base disturbances - examples Diarrhoea -> metabolic acidosis + vomiting -> metabolic alkalosis + catabolism, ->lactate metabolic acidosi Metabolic acidosis + respiratory alkalosis -20 -15 -10 -5 0 5 10 15 20 25 30 Base Excess mmol/l
Potassium, Acid-Base and volume
K+mmol/l 8 7 Nor mal 6 B 5 4 H+ kale mia r H+ K+ ang e A K+ C 3 D 2 1 A: Norm 6, 9 7, 0 7, 1 7, 2 7, 3 7, 4 7, 5 7, 6 7, 7 7, 8 p. H H+ K+ H+ H+ H+ K+ K+ K+ B: Acidemia exchange K+ / H+ K+ K+ C: long lasting acidemia K+ depletion H+ H+ K+ K+ D: K+ Rapid alkalinization - H+/K+ - dangerous hypokalemia
K+ Potassium depletion Normal or increased intake of potassium From 10% to 50% from 5% to 30%
K + H+ H+ Intracellular acidosis in proximal tubule Enhanced resorption HCO 3 - Enhanced resorption Cl- Effect of hypokalemia on ECF volume Enhanced resorption Cl-
Potassium depletion Large delivery of sodium in CCD (e. g. in osmotic diuresis) Low chloride in CCS Catabolism Long lasting acidemia Hypealdosteronism Diuretics (Furosemid) K+ K+
Potassium retention Oliguric phase of acute renal failure Tubular damage (e. g. interstitial nephritis, diabetic nephropathy) Hypoaldosteronism (m. Addisoni) K+ K+
ACID-BASE BALANCE Danish School of acidbase balance ? "Modern" approach to acidbase balance by Stewart and Fencl
Classical approach of "Danish School" Problem: How to measure PCO 2?
Measurement of Acid-Base parameters p. H, p. CO 2, [HCO 3 -] HCO 3 - CO 2 H 2 CO 3 H 2 O H+ HBuf Buf-
Measurement of Acid-Base parameters p. H, p. CO 2, [HCO 3 -] HCO 3 - CO 2 H 2 CO 3 H 2 O H+ HBuf Buf-
Measurement of Acid-Base parameters p. H, p. CO 2, [HCO 3 -] Alkaline reserve HCO 3 - CO 2 H 2 CO 3 H 2 O H+ HBuf Buf-
Measurement of Acid-Base parameters p. H, p. CO 2, [HCO 3 -] P. Astrup 1956 HCO 3 - CO 2 H 2 CO 3 H 2 O H+ HBuf Buf-
Equilibration method for p. CO 2 measurement by Astrup log PCO 2 High level p. CO 2 in mixture O 2/CO 2 Titration curve p. CO 2 in measered sample Low level p. CO 2 In mixture O 2/CO 2 p. H after equilibration with high p. CO 2 p. H In blood sample (before í equilibration p. H after equilibration with low p. CO 2
Buffer Base (BB) BB = [HCO 3 ]+ [Buf ] CO 2 depends on c. Hb HCO 3 - H 2 CO 3 H 2 O H + Normal buffer base: NBB=41. 7+0. 42*c. HB [g/100 ml] Base Excess: BE=BB-NBB HBuf -
HCO 3 - CO 2 H 2 CO 3 H 2 O + 1 mmol H+ added to 1 litre of blood H + HBuf -
HCO 3 - CO 2 H 2 CO 3 H 2 O + 1 mmol H+ added to 1 litre of blood H + HBuf 1 mmol/l drop of [HCO 3 -] + [Buf-] Buf BE=-1 mmol/l -
HCO 3 - CO 2 H 2 CO 3 H 2 O + 1 mmol OH- added to 1 litre of blood H + HBuf -
HCO 3 - CO 2 H 2 CO 3 H 2 O + 1 mmol OH- added to 1 litre of blood H + HBuf 1 mmol/l increase of [HCO 3 -] + [Buf-] Buf BE= 1 mmol/l -
log p. CO 2 Plasma and blood with different hematocrit BE curve BE=0 40 torr BE=-5 BE=-10 7. 4 p. H
NBB=41, 7 + 0, 42 * c. HB Odečet BB reading of BE
Buffer reactions CO 2 + H 2 O H+ + HCO 3 - H 2 CO 3 H+ + Buf- HBuf H+ + Hb- HHb H+ + Alb- HAlb H+ + HPO 42 - H 2 PO 4 -
Buffer reactions CO 2 + H 2 O H+ + HCO 3 - H 2 CO 3 H+ + Buf- HBuf H+ + Hb- HHb H+ + Alb- HAlb H+ + HPO 42 - H 2 PO 4 - Nebikarbonátové pufry Buf = Hb + Alb + PO 4 -
Buffer reactions HCO 3 - CO 2 H 2 CO 3 H 2 O H+ HBuf Buf-
Siggaard-Andersen BB=[HCO 3 -] +[Buf-] = const HCO 3 - CO 2 Siggaard-Andersen H 2 CO 3 H 2 O H+ HBuf Buf-
BE=0 m. Eq/l BE=-15 m. Eq/l
Siggaard-Andersen (1960 -1962) Definition (for blood in vitro) - Buffer Base: [BB]=[HCO 3 -]+[Buf-] (independent on p. CO 2) -Normal Buffer Base: [NBB] [BB] při p. H=7. 4 při p. CO=40 torr at given. Hb (SA nomogram - at normal albumins, phophates) -Base Excess: [BE]=[BB]-[NBB] Definition only for standard conditions not included hypo/hyperalbuminemia hyper/hypophosphatemia SA nomogram initialy was defined at 38°C
Siggaard-Andersen (1974 -1995) Definition (for blood in vitro) - Buffer Base: [BB]=[HCO 3 -]+[Buf-] (independent on p. CO 2) -Normal Buffer Base: [NBB] [BB] při p. H=7. 4 při p. CO=40 torr at given. Hb (SA nomogram - at normal albumins, phophates) -Base Excess: [BE]=[BB]-[NBB] Definition NBB dependent on Hb, albumin and phosphates
Problems of Danish school • Problems: In patients with acute disturbances of nonbikarbonate buffers : e. g. altered plasma concentrations ( if the original SA nomogram is used)
Stewart theory (1983) Ca+ K+ Mg+ Na+ HCO 3 - Buf- XA - Cl- SID [H+] [OH-] = K'w Peter Stewart [Buf-]+[HBuf] = [Buf. TOT] [Buf-] [H+] = KBuf [HBuf] [H+] [HCO 3 -] = M × p. CO 2 [H+] [CO 32 -] = N × [HCO 3 -] SID+ [H+]– [HCO 3 -] – [Buf-]– [CO 32 -]– [OH-] = 0
Stewart theory – solution of equations [H+]4 + (SID + KBUF) [H+]3 + +(KBUF (SID - [Buf. TOT])- K'w-M×p. CO 2)[H+]2 - (KBUF(K'w 2 + M × p. CO 2)-N×M×p. CO 2)[H+] - K'w×N×M×p. CO 2 = 0 p. H = f (p. CO 2, SID, Buf. TOT)
Mathematical wizardry Vladimír Fencl dependency of variables = causality p. H = f (p. CO 2, SID, Buf. TOT)
Stewart‘s „modern approach Lungs Ventilation Perfusion KREV Independent variables CO 2 Dependent variables [HCO 3 -] PCO 2 Tissues Perfusion Metabolism Transport SID [Buf. TOT] [Buf-] [CO 32 -] [OH-] [H+] (p. H) CO 2 STRONG IONS KIDNEYS Filtration Resorption Secretion GIT Absorbtion Secretion LIVER Synthesis Degradation PROTEINS STRONG IONS
BALANCE THEORY Excretion of CO 2 in the lungs The excretion of strong acids in the kidney CO 2 production Metabolic production of strong acids
Hemodynamics Integrative physiology Volume balance osmotic balance Oxygen transport ionic balance Acid-Base homeostasis
Cardiac Output Frank-Starling law The heart is a pump driven by its inflow (or pressure on its input) End diastolic pressere
Basic properties of blood vessels
Inlet pressure Flow The heart is a pump driven by its inflow (or pressure on its input)
Inlet pressure Flow Elastic veins The heart is a pump driven by its inflow (or pressure on its input) Capillary and arteriolar resistances Elastic arteries
Inlet pressure Flow Elastic veins The heart is a pump driven by its inflow (or pressure on its input) pressure Capillary and arteriolar resistances volume Elastic arteries
Inlet pressure Flow Elastic veins The heart is a pump driven by its inflow (or pressure on its input) pressure Capillary and arteriolar resistances volume Elastic arteries
Inlet pressure Flow Elastic veins The heart is a pump driven by its inflow (or pressure on its input) pressure Capillary and arteriolar resistances volume Elastic arteries
Inlet pressure Flow Elastic veins The heart is a pump driven by its inflow (or pressure on its input) pressure Capillary and arteriolar resistances volume Elastic arteries
Inlet pressure Flow Elastic veins The heart is a pump driven by its inflow (or pressure on its input) pressure Capillary and arteriolar resistances volume Elastic arteries
Inlet pressure Flow Elastic veins The heart is a pump driven by its inflow (or pressure on its input) pressure P V 0 V volume compliance C=d. V/d. P Capillary and arteriolar resistances Elastic arteries
Inlet pressure Flow Elastic veins The heart is a pump driven by its inflow (or pressure on its input) pressure P V 0 V volume compliance C=d. V/d. P Capillary and arteriolar resistances Elastic arteries
Inlet pressure Flow Elastic veins The heart is a pump driven by its inflow (or pressure on its input) pressure P V 0 V volume compliance C=d. V/d. P Capillary and arteriolar resistances Elastic arteries
Inlet pressure Flow Elastic veins The heart is a pump driven by its inflow (or pressure on its input pressure P V 0 V volume compliance C=d. V/d. P Capillary and arteriolar resistances Elastic arteries
Inlet pressure Flow Elastic veins The heart is a pump driven by its inflow (or pressure on its input) pressure P V 0 V volume compliance C=d. V/d. P Capillary and arteriolar resistances Elastic arteries
Inlet pressure Flow Elastic veins The heart is a pump driven by its inflow (or pressure on its input pressure P C 1 V 0 C 2 V volume compliance C=d. V/d. P Capillary and arteriolar resistances Elastic arteries
Inlet pressure Flow Elastic veins The heart is a pump driven by its inflow (or pressure on its input pressure P C 1 d. P d. V 1 V 0 d. V 1/d. P< d. V 2/d. P < C 2 d. V 2 V volume compliance C=d. V/d. P Capillary and arteriolar resistances Elastic arteries
Inlet pressure Flow Elastic veins The heart is a pump driven by its inflow (or pressure on its input pressure P C 1 V 0 d. V 1/d. P< d. V 2/d. P < C 2 V volume compliance C=d. V/d. P Capillary and arteriolar resistances Elastic arteries
Guyton experiments http: //patf-biokyb. lf 1. cuni. cz/~tribula/cirkulaceen/
Flow Q Elastic arteries Elastic veins Pv Pa The heart is a pump driven by its inflow (or pressure on its input Capillary and arteriolar resistances
Flow Q=0 Elastic arteries Elastic veins Pv Pa The heart is a pump driven by its inflow (or pressure on its input Capillary and arteriolar resistances
Flow Q=0 Elastic arteries Elastic veins Pv Pa The heart is a pump driven by its inflow (or pressure on its input Capillary and arteriolar resistances
Flow Q=0 Elastic arteries Elastic veins Pv Pa The heart is a pump driven by its inflow (or pressure on its input Capillary and arteriolar resistances
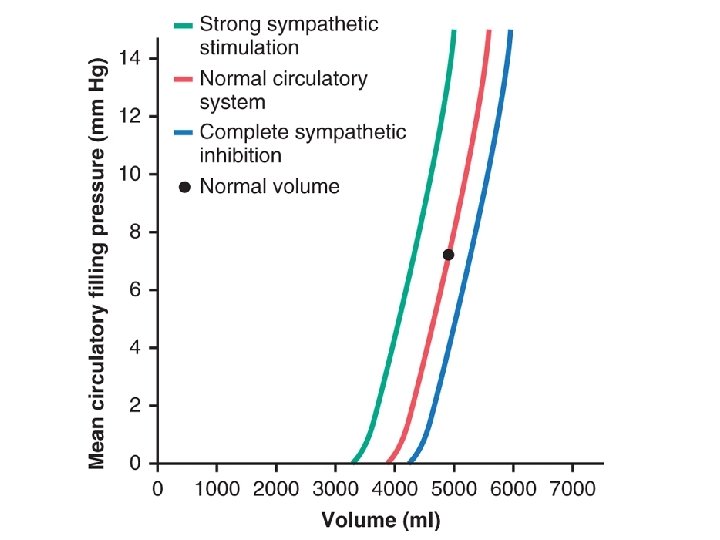
Flow Q=0 Elastic arteries Elastic veins Pa = Pm Pv Q Pv = P a = Pm Capillary and arteriolar resistances Pm Pv Pm – „mean circulatory pressure“
Flow Q Elastic arteries Elastic veins Pa Pv Q Capillary and arteriolar resistances Pm Pv
Flow Q Elastic arteries Elastic veins Pa Pv Q Capillary and arteriolar resistances Pm Pv
Flow Q Elastic arteries Elastic veins Pa Pv Q Capillary and arteriolar resistances Pm Pv
Flow Q Elastic arteries Elastic veins Q Pv=0 Pa Pv Capillary and arteriolar resistances Pm Pv
Flow Q cannot rise Elastic arteries Elastic veins Q Pv<0 Pv < 0 Pa Elastic veins collapses Pv Capillary and arteriolar resistances Pm Pv
Flow Q=0 Elastic arteries Elastic veins Q Pa = Pm Pv Pv= Pm Capillary and arteriolar resistances Pm Pv
Flow Q Elastic arteries Elastic veins Pa Pv Q Capillary and arteriolar resistances Pm Pv
Flow Q Elastic arteries Elastic veins Pa Pv Q Capillary and arteriolar resistances Pm Pv
Flow Q Elastic arteries Elastic veins Pa Pv Q Capillary and arteriolar resistances Pm Pv
Flow Q Elastic arteries Elastic veins Pa Pv Q Capillary and arteriolar resistances Pm Pv
Flow Q Elastic arteries Elastic veins Q Pv=0 Pa Pv Capillary and arteriolar resistances Pm Pv
Flow Q cannot rise Elastic arteries Elastic veins Q Pv<0 Pa Elastic veins collapes Pv Capillary and arteriolar resistances Pm Pv
Flow Q=0 Elastic arteries Elastic veins Q Pa = Pm Pv Pv= Pm Capillary and arteriolar resistances Pm Pv
Flow Q=0 Elastic arteries Elastic veins Q Pa = Pm Pv Pv= Pm Capillary and arteriolar resistances Pm Pv
Flow Q Elastic arteries Elastic veins Pa Pv Q Capillary and arteriolar resistances Pm Pv
Flow Q Elastic arteries Elastic veins Pa Pv Q Capillary and arteriolar resistances Pm Pv
Flow Q Elastic arteries Elastic veins Pa Pv Q Capillary and arteriolar resistances Pm Pv
Flow Q Elastic arteries Elastic veins Pa Pv Q Capillary and arteriolar resistances Pm Pv
Flow Q Elastic arteries Elastic veins Q Pv=0 Pa Pv Capillary and arteriolar resistances Pm Pv
Flow Q cannot rise Elastic arteries Elastic veins Q Pv<0 Pa Elastic veins collapes Pv Capillary and arteriolar resistances Pm Pv
Flow Q=0 Elastic arteries Elastic veins Q Pa = Pm Pv Pv= Pm Capillary and arteriolar resistances Pm Pv
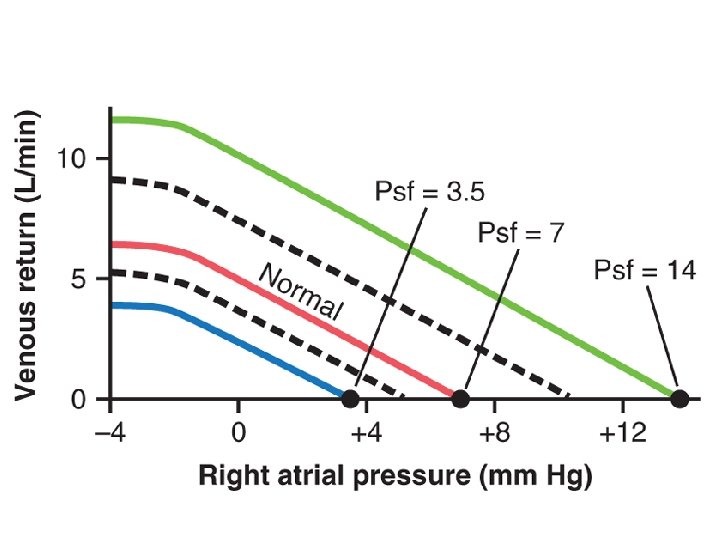
Flow Q=0 Elastic arteries Elastic veins Pa = Pm Venotonus Q Pv Pv= Pm Capillary and arteriolar resistances Pm Pm Pv
Flow Q=0 Elastic arteries Elastic veins Pa = Pm Venotonus Q Pv Pv= Pm Blood Volume Capillary and arteriolar resistances Pm Pm Pv
Flow Q=0 Elastic arteries Elastic veins Pa = Pm Venotonus Q Pv Pv= Pm Blood Volume Capillary and arteriolar resistances Pm Pm Pv
Flow Q Elastic arteries Elastic veins Pa Venotonus Pv Blood Volume Q Capillary and arteriolar resistances Pm Pm Pv
Flow Q Elastic arteries Elastic veins Pa Venotonus Pv Blood Volume Q Capillary and arteriolar resistances Pm Pm Pv
Flow Q Elastic arteries Elastic veins Pa Venotonus Pv Blood Volume Q Capillary and arteriolar resistances Pm Pm Pv
Flow Q Elastic arteries Elastic veins Pa Venotonus Pv Blood Volume Q Capillary and arteriolar resistances Pm Pm Pv
Flow Q Elastic arteries Elastic veins Pa Venotonus Q Pv=0 Pv Blood Volume Capillary and arteriolar resistances Pm Pm Pv
Flow Q cannot rise Elastic arteries Elastic veins Q Pv<0 Pv Pa Elastic veins collapes Venotonus Blood Volume Capillary and arteriolar resistances Pm Pm Pv
Heart + Vessels http: //patf-biokyb. lf 1. cuni. cz/~tribula/cirkulaceen/
Cardiac output 0 End diastolic pressure
Cardiac output Increase of peripheral resistance 0 End diastolic pressure
Cardiac output Decrease of peripheral resistance Increase of peripheral resistance 0 End diastolic pressure
Cardiac output Increase blood volume or (increase of venotone) Decrease of peripheral resistance Increase of peripheral resistance 0 End diastolic pressure
Cardiac output Increase blood volume or (increase of venotone) Decrease of peripheral resistance Decrease blood volume or (decrease of venotone) Increase of peripheral resistance 0 End diastolic pressure
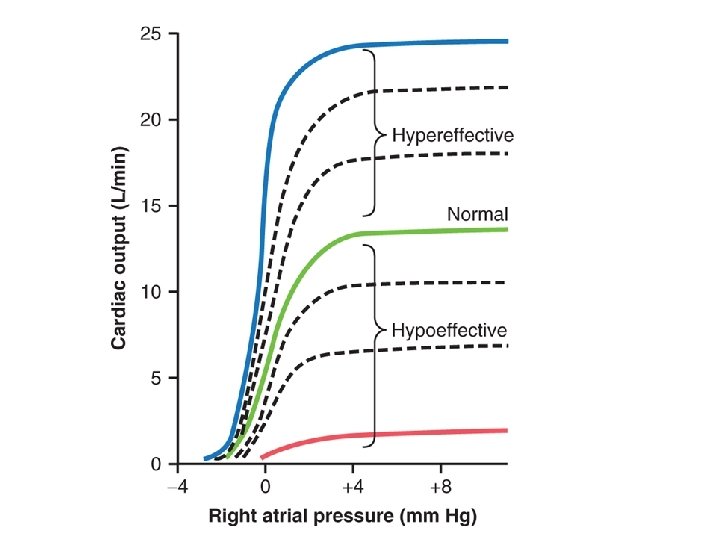
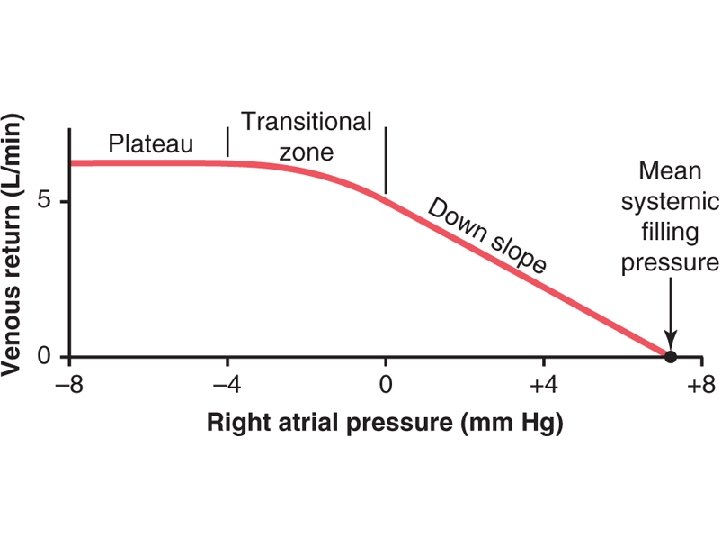
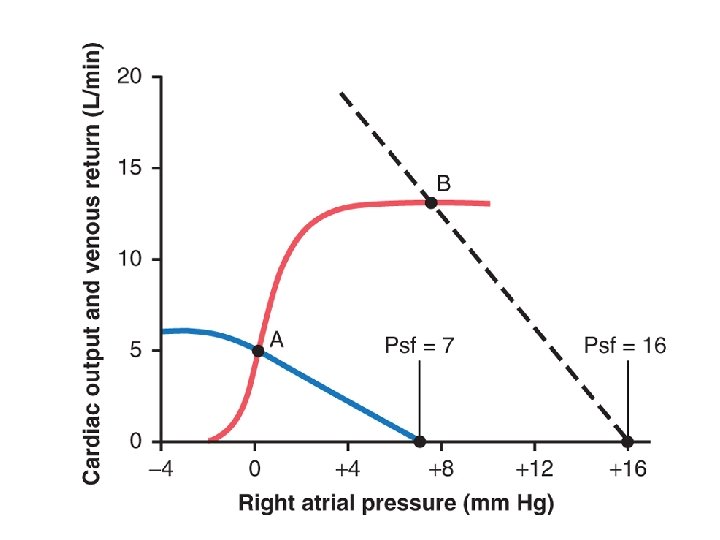
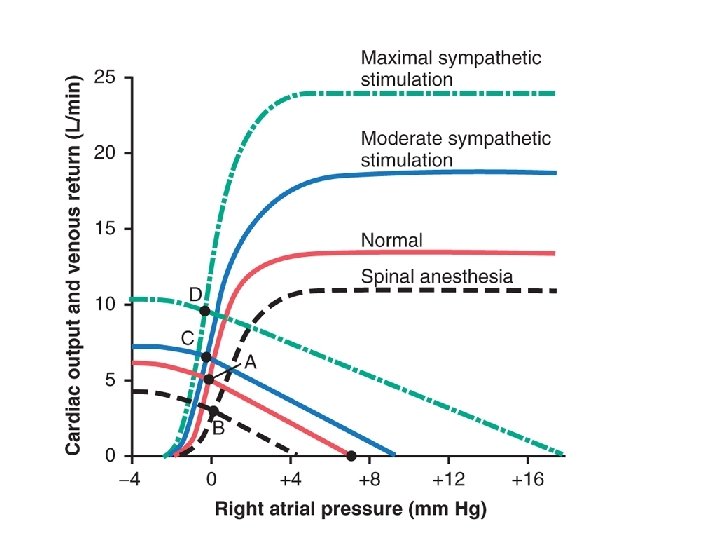
Cardiac output Frank-Starling curve Venous return curve End diastolic pressure
Cardiac output Frank-Starling curve Venous return curve End diastolic pressure
Cardiac output Frank-Starling curve Venous return curve End diastolic pressure
Cardiac output Frank-Starling curve Venous return curve End diastolic pressure
Cardiac output Frank-Starling curve Venous return curve End diastolic pressure
Cardiac output Frank-Starling curve Venous return curve End diastolic pressure
Cardiac output Frank-Starling curve Venous return curve End diastolic pressure
Cardiac output diuretics kardiotonics e i c fi in f u s he gt sin d rea of loo , Inc ume ing b tion l c vo ulat nstri tion c c cir oko nstri n ve soco va y c n End diastolic pressure increase ! pulmonary edema, swelling End diastolic pressure
Starling curve and venous return curve St ar lin g cu r ve Cardiac output us no Ve rn tu re e rv cu preload Normal circulation
Starling curve and venous return curve Cardiac output inotropy, heart rate St ar lin g cu r ve Cardiac output inotropy, heart rate us no Ve rn tu re e rv cu preload Normal circulation preload Starling curve changes
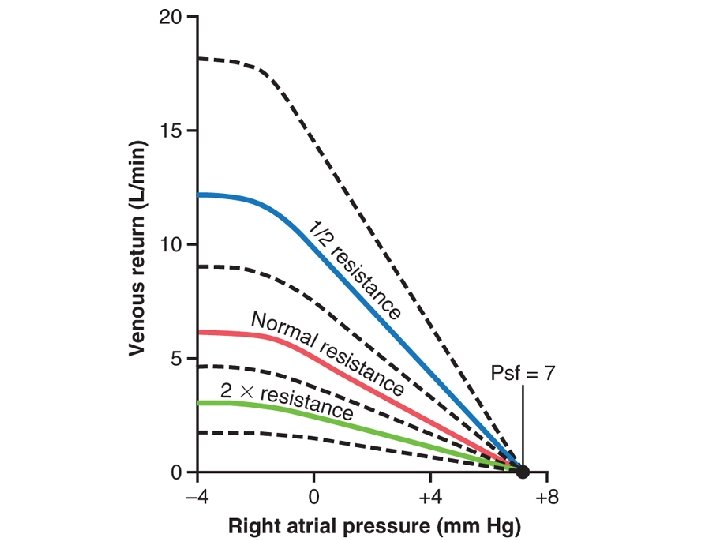
Starling curve and venous return curve Cardiac output inotropy, heart rate St ar lin g cu r ve Cardiac output inotropy, heart rate us no Ve rn tu re e rv cu preload Normal circulation Starling curve changes res ce re s an ist Cardiac output is preload ta nc e preload Venous return curve changes
Starling curve and venous return curve Cardiac output inotropy, heart rate St ar lin g cu r ve Cardiac output inotropy, heart rate us no Ve rn tu re e rv cu preload Normal circulation Starling curve changes is s, e nu um to ol no d v ve loo b ce re s an ist Cardiac output s, e nu um to ol no d v ve loo b res Cardiac output ta nc e preload Venous return curve changes
Starling curve and venous return curve Cardiac output inotropy, heart rate St ar lin g cu r ve Cardiac output inotropy, heart rate us no Ve rn tu re e rv cu preload Normal circulation Starling curve changes is s, e nu um to ol no d v ve loo b ce re s an ist Cardiac output s, e nu um to ol no d v ve loo b res Cardiac output ta nc e preload Venous return curve changes
Basic Priciples of Hemodynamics in Shock St ar lin g cu r ve Cardiac output us no Ve rn tu re e rv cu preload Normal circulation
Cardiac output ncy Cardiac insufficie in me olu se rea nv inc tio ten Re e Th co so Va us no ve e ton n tio ric t ns Cardiogenic shock End diastolic pressure preload
Basic Priciples of Hemodynamics in Shock Cardiac output St ar lin g cu r ve Cardiac output inotropy Ve us no resistance rn tu re venotonus e rv cu preload Normal circulation preload Cardiogenic shock
tropy o n i d n a art rate e h d e s a Incre Cardiac output se ea cr e in m n n lu tio a vo ric n of nst tio ss co sa Lo so pen Va om C of us no ve ne to preload Hypovolemic shock
Basic Priciples of Hemodynamics in Shock Cardiac output St ar lin g cu r ve Cardiac output inotropy Ve us no resistance rn tu re venotonus e rv cu preload Normal circulation Cardiogenic shock blood volume resistance heart rate inotropy preload Hypovolemic shock preload
nd inotropy Cardiac output rate a Increased heart n cardiodepressio od vas s of atio ilat Los n me volu tion uda nss – tra F to IS Distributive shock preload
Basic Priciples of Hemodynamics in Shock Cardiac output St ar lin g cu r ve Cardiac output inotropy Ve us no resistance rn tu re venotonus e rv cu preload Normal circulation preload Cardiogenic shock blood volume resistance heart rate inotropy preload Hypovolemic shock resistance blood volume heart rate inotropy preload Distributive shock
Basic Priciples of Hemodynamics in Shock Cardiac output St ar lin g cu r ve Cardiac output inotropy Ve us no resistance rn tu re venotonus e rv cu preload Normal circulation preload Cardiogenic shock
Basic Priciples of Hemodynamics in Shock Cardiac output St ar lin g cu r ve Cardiac output inotropy Ve us no resistance rn tu re venotonus e rv cu preload Normal circulation Cardiogenic shock blood volume resistance heart rate inotropy preload Hypovolemic shock preload
Basic Priciples of Hemodynamics in Shock Cardiac output St ar lin g cu r ve Cardiac output inotropy Ve us no resistance rn tu re venotonus e rv cu preload Normal circulation preload Cardiogenic shock blood volume resistance heart rate inotropy preload Hypovolemic shock resistance blood volume heart rate inotropy preload Distributive shock
Basic Priciples of Hemodynamics in Shock Cardiac output St ar lin g cu r ve Cardiac output inotropy Ve us no resistance rn tu re venotonus e rv cu preload Normal circulation preload Cardiogenic shock blood volume resistance heart rate inotropy preload Hypovolemic shock resistance blood volume heart rate inotropy preload Distributive shock
Hemodynamics Integrative physiology Volume balance osmotic balance Oxygen transport ionic balance Acid-Base homeostasis
Oxygen delivery Pi. O 2 Pa. O 2 Ventilation Sa. O 2 Hb Ca. O 2*Q Circulation
Oxygen delivery Pi. O 2 Pa. O 2 Ventilation Sa. O 2 Hb Circulation Ca. O 2*Q ATP/ADP ratio etc. Metabolic requirement VO 2 Cells Oxygen comsumption
Oxygen delivery Pv. O 2 Pa. O 2 Ventilation Cv. O 2 Sa. O 2 Hb Circulation Ca. O 2*Q Pa. O 2 Diffusion Pist. O 2 ATP/ADP ratio etc. Metabolic requirement VO 2 Cells Oxygen comsumption
Oxygen delivery Pi. O 2 Pa. O 2 Ventilation Cv. O 2 Sa. O 2 Circulation Hb Ca. O 2*Q Pa. O 2 Diffusion Pist. O 2 ATP/ADP ratio etc. Metabolic requirement VO 2 critical. DO 2 VO 2 Cells Oxygen comsumption Oxygen delivery - DO 2
Hemodynamics Integrative physiology Volume balance osmotic balance Oxygen transport ionic balance Acid-Base homeostasis
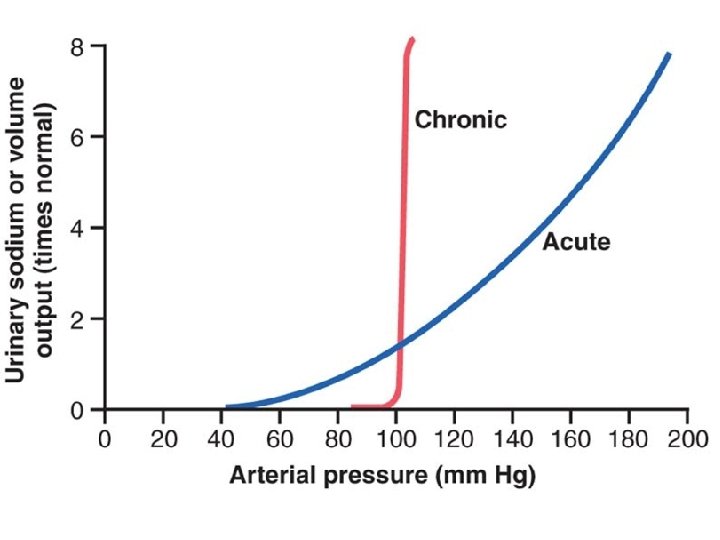
Blood Volume Extracellular fluid volume Arterial Pressure
return
Starling curve and venous return curve
Strenous excercise Rest
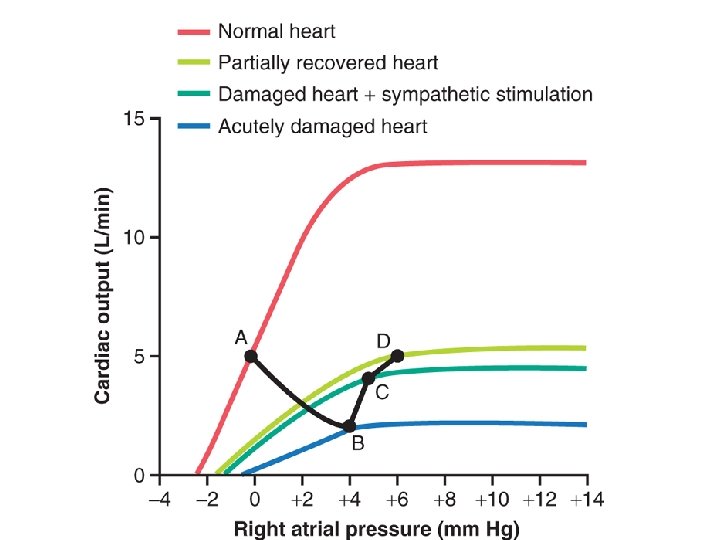
Decompensated cardiac failure
Treatment od decompensated cardiac failure
High-output cardiac failure return