Herpesviridae INTRODUCTION TO THE FAMILY HERPESVIRIDAE GENERAL CHARACTERISTICS




 surrounded by amorphous tegument")

 and inhibiting the")






















")













 which first appear 14")










 Newborn children whose mothers develop chickenpox during the last five days of pregnancy")
- Slides: 66
Herpesviridae
INTRODUCTION TO THE FAMILY HERPESVIRIDAE GENERAL CHARACTERISTICS ØHerpesviruses are amongst the largest human viruses ØHV infections have been recognised since ancient times ØHerpesviruses are highly disseminated in nature ØTo date, there are 8 known human Herpesviruses.
Subfamily Biological properties ØVariable host range Alphaherpesvirinae ØRapid reproductive cycle ØEstablish latent infections in neurons ØHerpes simplex virus type 1 (HSV-1) ØHerpes simplex virus type 2 (HSV-2) ØVaricella-Zoster virus (VZV) HHV-3 ØGenerally restricted host range ØSlow reproductive cycle ØCytomegalic ØEstablish latency in lymphocytes, monocytes, SG, kidney. ØRestricted host range ØLymphotropic, lymphproliferative. ØEstablish latent infections in lymphoid cells ØHuman cytomegalovirus (HCMV) HHV-5 ØHuman herpesvirus 6 (HHV-6) ØHuman herpesvirus 7 (HHV-7) α Betaherpesvirinae β Gammaherpesvirinae γ ØEpstein-Barr virus (EBV-HHV-4) ØHuman herpesvirus 8 (HHV-8)
ss
ØSpherical enveloped virions, 120 -200 nm. ØIcosahedral capsids (162 capsomeres) surrounded by amorphous tegument , then lipid envelope. ØLinear ds. DNA genome, genome associated with protein core. ØReplicates in the nucleus
Herpesviruses Latency • All herpesviruses establish latent infections • Latent infections last the lifetime of the individual • Latency occurs in different cell types for different herpesviruses • Viral lytic cycle genes are not expressed during latency • Latent virus may reactivate, causing recurrent disease or subclinical virus shedding
interfere with apoptosis by downregulating a number of host factors, including(MHC) and inhibiting the apoptotic pathway
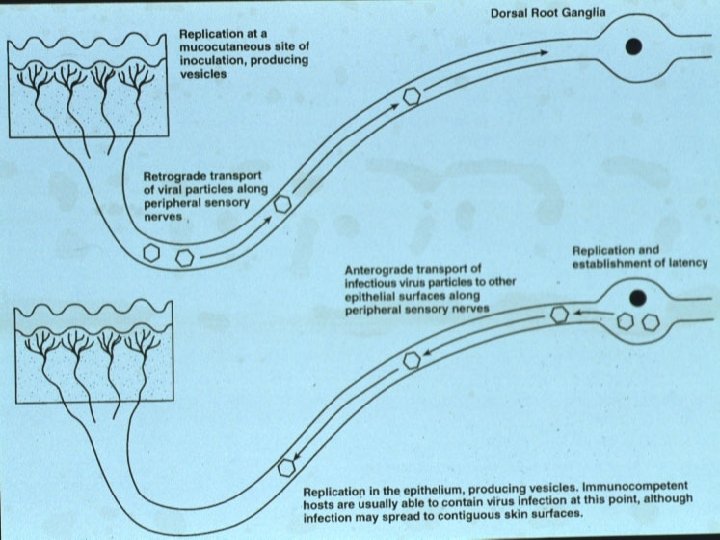
Herpesviruses Reactivation • Reactivation – Spontaneous – Stimuli: sunlight, stress, menstruation, other infections, immunocompromistion. • Reactivated virus travels back down axon causing infection near site of 1° infection
Herpes simplex virus (HSV( Properties • ectodermal tissue tropism • vesicular lesions. • infection multinucleated cell • latency HSV-1 trigerminal nerve ganglia HSV-2 lumbosacral nerve ganglia
HSV-1 vs. HSV-2 • Closely related but clearly distinct viruses • Distinguishable by immunological and molecular methods • HSV-1 has a predilection for causing oral infections • HSV-2 is more likely to cause genital infections • “HSV-1 above the waist, HSV-2 below the waist” is a general rule, not an absolute truth.
Herpes simplex virus transmission • Close body contact • Sexual intercourse • Contaminated materials
Clinical Manifestations HSV is involved in a variety of clinical manifestations which includes-;
Herpes Simplex Virus Infections
Herpes Gingivostomatitis
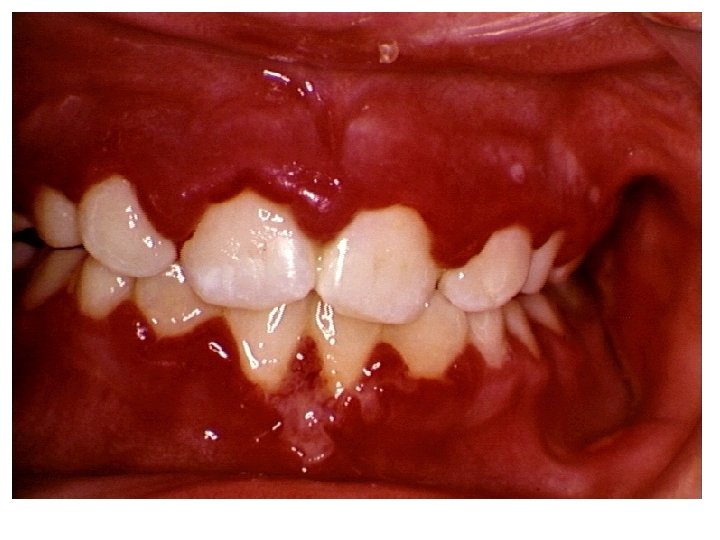
Acute herpetic gingivostomatitis • • • Primary infection. HSV-1 Young children 6 m - 6 years I. P : 2 -12 days (6). Sudden onset of fever, irritability, inability to eat and drink. Cervical lymphadenopathy. Vesiculo-ulcerative lesions. Intra-oral lesions usually are covered with a grayish, white plaque. Lesions involve the lips, palate, tongue and gums Disease is self limited (within a week) but may cause considerable discomfort.
Acute herpes gingivostomatitis
Pharyngotonsillitis • Is the primary infection in adolescent and adults. • Similar to β– haemolytic strept. throat. • Clinical feature: exudative. Fever, lymphadenopathy
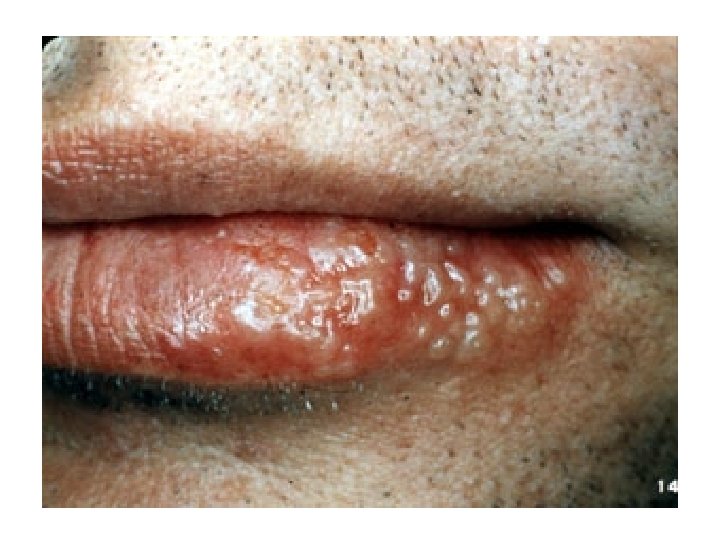
Herpes labialis • Recurrent infection • HSV-1 • Occur along the mucocutaneous junction of the lips. • They may be single or clustered (3 -5 vesicles). • The duration is usually 10 -14 days. • Treatment is usually necessary only in immunecompromised patients.
Herpetic keratoconjunctivitis • Mostly caused by HSV-1 • primary/recurrent infection • lesions eyelid -> vesicle conjuctiva cornea -> dendritic ulcer Geographic ulcer Repeated infection <-stromal formation (rarely blindness).
HSV; eye infection Dendritic ulcer at cornea
Geographic ulcer as a complication of herpes simplex keratoconjunctivitis.
Neonatal herpes • Caused by HSV-2 (The virus can either be obtained in utero or during birth with the latter being more common) • Infectivity higher in primary. • Generalized infection - underdeveloped immune system.
Neonatal HSV infections 50% SEM recover mucocutaneous disease, skin, 20% 80% full premature term eye , mouth, 50% disseminated &/or neurological disease Disseminated &/or neurological disease 30 % survive with neuro &/ or eye damage 70% die
Herpes meningitis & encephalitis • Primary/recurrent infection • HSV-1(most common sporadic viral encephalitis. ) & HSV-2 • Diffuse or localized. • damage to one of the temporal lobes. As a result there is blood in the CSF and the patient experiences neurological symptoms such as seizures. • HSV Meningitis This is the result of an HSV-2 infection. The symptoms
Disseminated HSV • Organ transplantation, Cancer , AIDS , severe burn • Liver, kidney, adrenal, spleen, brain , bone marrow • Clinical : fever, hemorrhagic vesicles, esophagitis , pneumonitis, renal failure, hepatitis
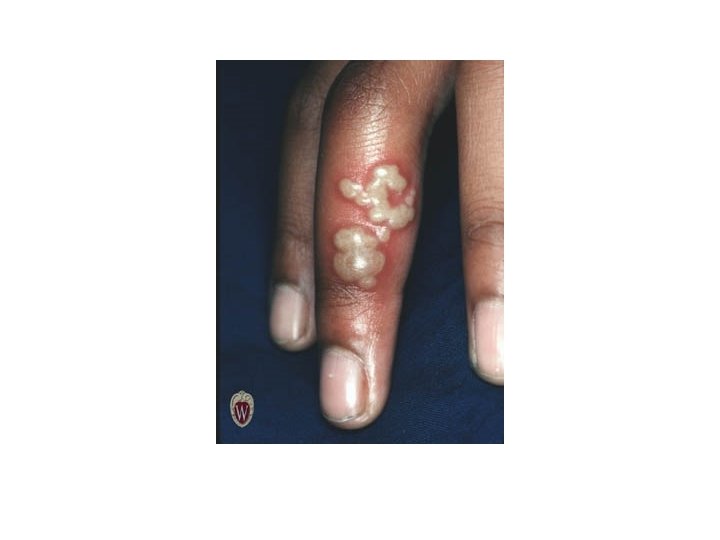
Herpetic whitlow • Manual contact with herpes-infected body secretions • Can be caused by either type of HSV and enters the body via small wounds on the hands or wrists. • It can also be caused autoinoculation
Herpes gladiatorum • This is contracted by wrestlers. • usually appears in the head and neck region • lesions are more often on the right side of the body • It is also seen in other contact sports such as rugby where it is known as scrum pox (Herpes Rugbeiorum).
Eczema herpeticum • in children with active eczema, preexisting atopic dermatitis. • rash is often accompanied by a fever and general malaise • can spread over the skin at the site of eczema lesions. • The virus can spread to other organs such as the liver and adrenals.
Classical primary genital herpes affecting the vulva. This clinical picture is seen in a minority of cases
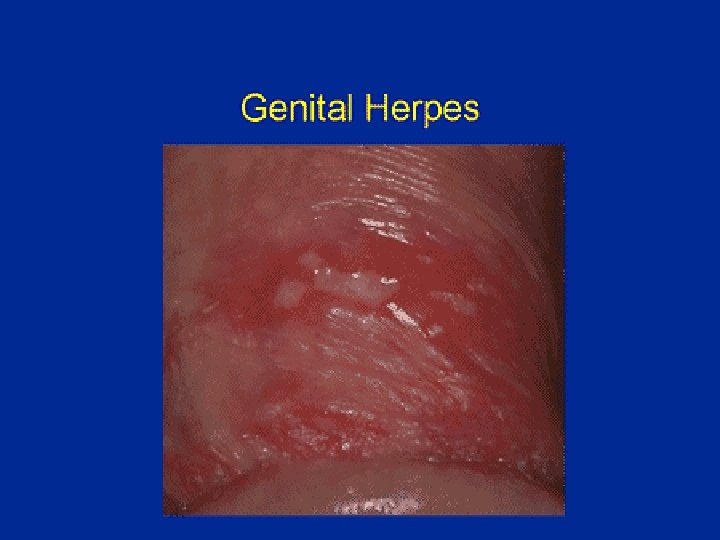
Genital Herpes Vesicles on the penis • facilitate transmission of HIV
HSV proctitis This is an inflammation of the rectum and the anus
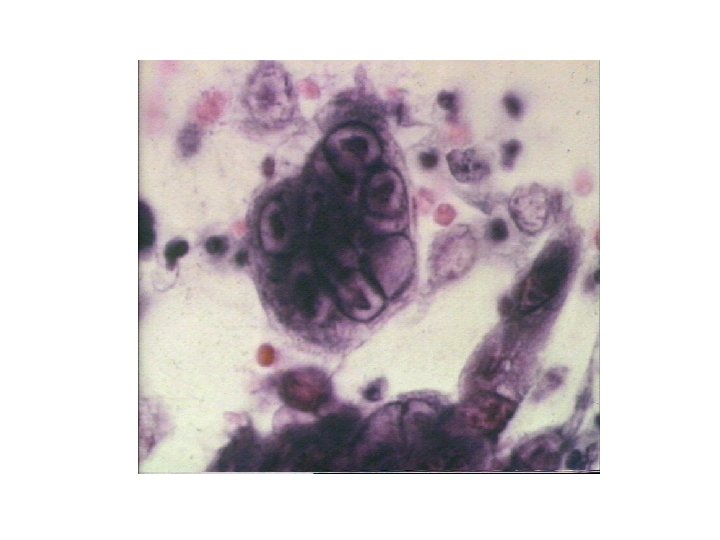
Both clinical and lab criteria are useful A definitive diagnosis : confirmed by isolating the virus in tissue cultures. Vial shell culture. scrapings of skin vesicles and mucosal lesions / transfer them VTM CPE : 24 -48 hours. scraping histologic appearances characteristic • A Tzanck: Wright’s, Giemsa’s , or Papanicolaou’s stain : ( multinucleated giant cells and contain Cowdry type A inclusion bodies), cytologic examination has low sensitivity (approximately 60 -70%). • IF Serologic diagnosis : only to determine past exposure to herpes simplex virus. It may be helpful in demonstrating a primary seroconversion PCR: is the preferred diagnostic.
acycloguanosine
Varicella-Zoster Virus Clinical disease recognised in two forms Primary infection - Varicella (Chicken Pox( Reactivation - Zoster
• Zoster = girdle: from the characteristic rash that forms a belt around the thorax in many patients. • The structure of Varicella virus is very similar to Herpes Simplex virus although the genome is somewhat smaller
• The known envelope glycoproteins (g. B, g. C, g. E, g. H, g. I, g. K, g. L) correspond with those in HSV, however there is no equivalent of HSV g. D. • VZV virons are spherical and 150200 nm in diameter • Its DNA is a single, linear, doublestranded molecule
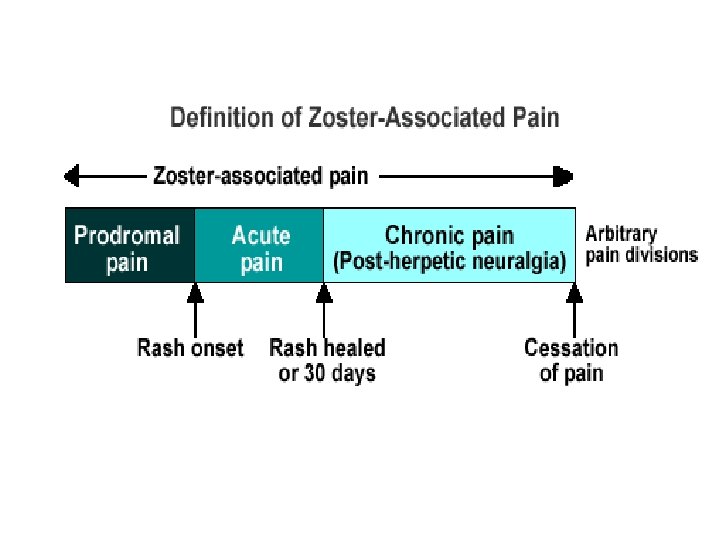
Pathogenesis 2 ry viremia is associated with prodromal symptoms (fever) which first appear 14 -15 days after initial infection 2 ry viremia is usually terminated after 3 days. Fever is followed by a maculopapular rash forming lesions over 2 -4 days. Vesicles contain fluid with infectious virus, and dry over. 1 -3 weeks
Varicella (chickenpox( • Primary infection of VZV • Highest prevalence occurring in children age 4 -10 years • Highly communicable disease, attack rate of 90% in close contacts • Incubation period of 14 -21 days • Infectivity : 2 d before - 5 d after rash appearance • latency: dorsal root ganglia.
Clinical features of Varicella Older children and adults may have prodrome symptoms. Younger children usually have an abrupt onset of rash with mild fever and malaise. Pruritus typically occurs with the rash. Vesicles are classically described as “dew drops on a rose petal”. Most children have 250 – 500 lesions, mostly vesicular. • • • 14 -15 d after exposure (=IP) Occasional prodrome symptoms lasting 2– 3 days: low-grade fever, chills, headache malaise, backache, anorexia, myalgia, nausea, or vomiting 16 -17 d ↓ Rash with crops of small red macules, beginning on the face and scalp, and spreading rapidly to the trunk. Relative sparing of the distal upper and lower extremities. 16 -17 d ↓ Rash progresses over 12– 14 hours to 1– 3 mm papules, vesicles, and then pustules. 17 -19 d ↓ Crust formation 23 - 27 d ↓ Healing Scarring is rare in uncomplicated cases.
Varicella; skin rash Varicella, demonstrating all stages of the rash; macules, papules, vesicles
Congenital Varicella syndrome • Congenital developmental malformations most commonly occur when maternal infection occurs in the first trimester. • These defects may include Ø Ø Ø hypoplastic limbs, cortical atrophy, cicatricial skin lesions, ocular abnormalities, psychomotor retardation, and low birth weight. • Infection in late pregnancy, the baby may develop neonatal varicella.
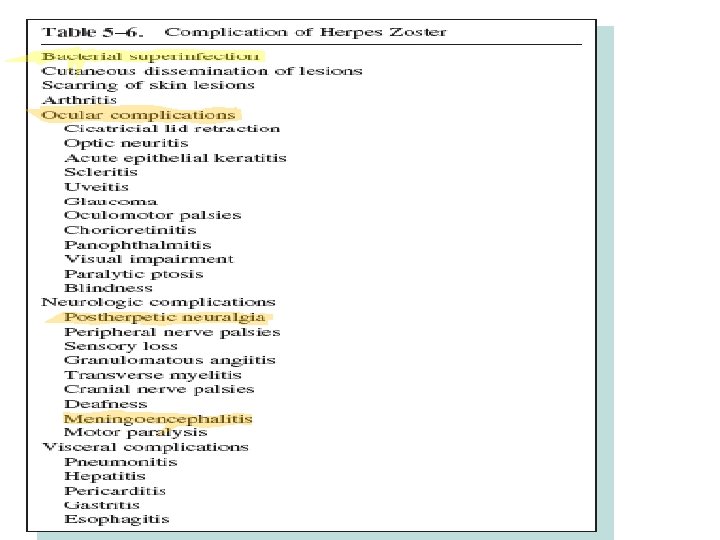
SECONDARY ZOSTER PATHOLOGY Reactivation as herpes zoster involves the ganglia and spinal nerves corresponding to the dermatome involved in the primary infection The areas supplied by the trigeminal nerve (opthalmic( , and thoracic ganglia are most often involved
Herpes Zoster ophthalmicus • Occur after zoster eruption in any branch of trigeminal n. (V 1) • Produce corneal dendrite • Common sequelae: stromal kerratitis, anterior uveitis, ocular motor n. palsy, acute retinal nerosis, post herpetic neuralgia
Scarring from herpes zoster.
Lab diagnosis • Clinical features are VERY DISTINCTIVE • EM • Isolation of VZV in susceptible tissue culture cell line • Tzank smear of vesicular fluid: Multinucleated giant cells and epithelial cells with eosinophilic intranuclear inclusion bodies. – Other histologic findings: Leukocytoclastic vasculitis and hemorrhage are more common in VZV lesions than herpes simplex. • Detection of antibodies: IFA, ELISA, FAMA (fluorescent antibody to membrane antigen) – The latex agglutination test : the most popular serologic assay for determining exposure and immunity to VZV. • PCR
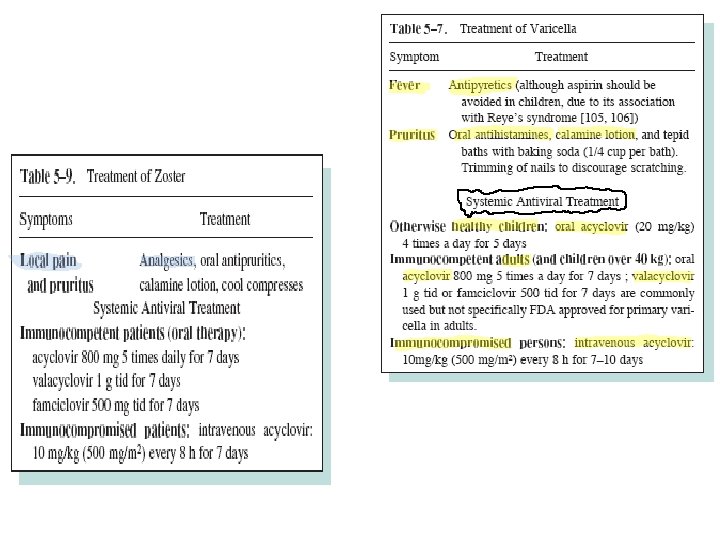
Treatment Normal host • Chickenpox – Children : self-limiting/supportive treatment – prevention of avoidable cpx. , acyclovir therapy is recommend for adolescents and adult with chicken -pox <24 hrs(acyclovir 20 mg/kg 4 times/day x 5) • Herpes zoster – Acyclovir 800 mg five times daily for 7 -10 days Immunocompromised host • Should be treat with intravenous acyclovir(1012. 5 mg/kg v q 8 hrs 7 days
Prevention : FOR ?
1) Newborn children whose mothers develop chickenpox during the last five days of pregnancy or up to two days after delivery. 2) Varicella-exposed premature babies of birthweight 1 kg or less, or babies born before the 28 th week of pregnancy are given VZIG irrespective of the mother’s antibody status. 3) Varicella-exposed seronegative children under certain types of immunosuppressive treatment for malignant disorders. 4)Massively varicella-exposed seronegative pregnant women.