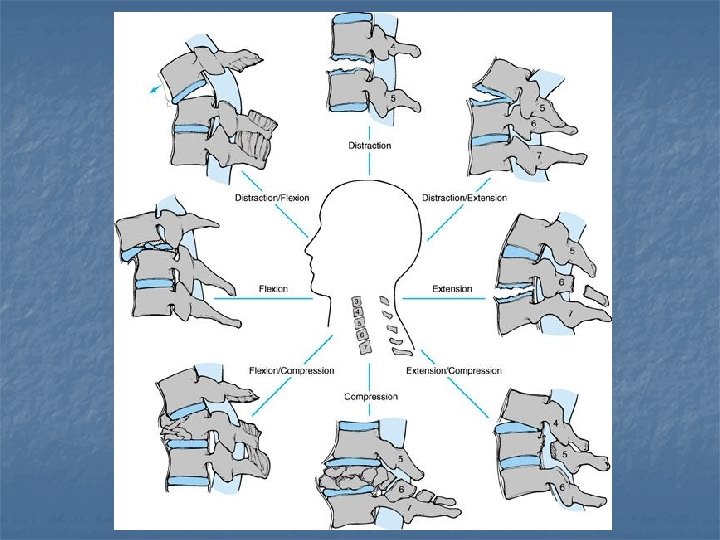
n Spine anatomy Xray Cervical spine n Thoracic









































































 nerve structures ↓ Irreversible Chance for recovery : Partial lesion n")
 Reduce necrosis /")


















 xiphoid process (T 7) umbilicus (T 10) Dermatomes inguinal")
























- Slides: 121
n Spine anatomy * X-ray Cervical spine n Thoracic spine n Lumbar spine n n Spine trauma Cervical spine n Thoracic & lumbar spine n n Trauma patient with spine lesion
Cervical spine
Spine Anatomy
Anatomy
Anatomy
Anatomy
Anatomy
Anatomy
Anatomy 3 2 1 4
Cervical spine X-ray
C spine X-ray Lateral view 5 4 6 1
C spine X-ray Lateral view
C spine X-ray Lateral view
C spine X-ray Lateral view
C spine X-ray Lateral view
C spine X-ray AP view 2 1
C spine X-ray AP view
C spine X-ray AP view
C spine X-ray Oblique view
C spine X-ray Oblique view
C spine X-ray Oblique view
C spine X-ray OMO view 1 2 2 3
C spine X-ray OMO view
Thoracic spine
Spine Anatomy
Anatomy
Normal kyphosis 15° - 50°
Anatomy
Anatomy
T spine X-ray
T spine X-ray AP view 1 2 3
T spine X-ray AP view
T spine X-ray lateral view
T spine X-ray lateral view
Lumbar spine
Spine Anatomy
Anatomy
Normal lordosis < 60° slop of sacral base = 45° from horizon
L spine X-ray
L spine X-ray AP view
L spine X-ray AP view
L spine X-ray AP view
L spine X-ray AP view 1 4 2 3
L spine X-ray Lateral view
L spine X-ray Lateral view
L spine X-ray Oblique view Scotty dog sign 3 1 2 4 5 6
L spine X-ray Oblique view Scotty dog
L spine X-ray Oblique view
L spine X-ray Oblique view
C spine trauma
Denis’ three column model of the spine
The stability n n n Anterior column injury → stable Anterior & middle column injury→more unstable 3 column injury → unstable
C 2 tear drop fracture stable
Hangman fracture Unstable
Wedge fracture Unstable
Tear drop fracture
C 5 -C 6 Bilateral facet dislocation
C 4 -C 5 Bilateral facet dislocation Unstable
Unlateral facet dislocation Unstable
C 5 C 6 bilateral facet subluxation Unstable
Atlantodental interval Atlanto-axial instability Unstable
Occipitoatlantal articulation Power ratio
T+ L spine trauma
90 % of spine fractures
Effects on spine‘s functions 1. 2. 3. 4. Stability Posture Neural protection Neurological function
Denis’ three column model of the spine
1 - Stability More columns damage → more instability
2 - Posture and deformity
2 - Posture and deformity n n n Pain Imbalance at the fracture site Compensatory curves
3 - Neural protection Spinal deformity ↓ spinal canal stenosis ↓ Varying degree of compression
Neural structures occupies 50% spinal canal volume
4 - neural function n n Nerve lesion Cord lesion
Nerve lesion (Overstretched–crushed–severed) nerve structures ↓ Irreversible Chance for recovery : Partial lesion n Release within 8 hours n
Cord lesion Drug may give a chance MPS ( corticosteroid ) Reduce necrosis / oedema n In the first 8 hours n n Regimen : 30 mg/kg/15 minutes After 45 minute 5. 4 mg/kg/hour for 23 hour
Lesion classification
T vertebra Burst fracture
L 2 burst fracture
L 3 burst fracture with rotation
2 T 8 burst fracture + T 9 wedge fracture 8
Trauma patient with spine lesion
Causes of spinal column and spinal cord injury
Trauma patient n n The A – B – C – D RESUSCITATION ( BP ) Conscious level ( Glasgow coma scale ) Assessment of injuries ( Determine the PRIORITY )
Trauma patient - accident scene n n n A : airways B : breathing C : circulation & cervical spine D : disability – drugs E : exposure ( undress the patient ) Spinal column injury must be suspected in in all polytrauma patients, especially < intoxicated – unconscious > individuals.
Trauma patient - Transfer Scoop-style stretcher
Trauma patient Transfer
Trauma patient - Resuscitation Blood pressure BP > 85 mm Hg → better neurogenic outcome
Neurogenic shock n 3 vital signs indicates above T 6 injury : Hypotension n Hypothermia n Bradycardia n Disruption of sympathetic outflow. T 1 -L 2 ↓ unopposed vagal tone
Low blood pressure. . !? ↓ BP + bradycardia =Neurogenic shock ↓ BP + tachycardia = blood loss occult intra-abdominal injuries
Trauma patient - Resuscitation How to deal with Neurogenic shock : n volume replacement n vasopressors And of course<Treat other injuries>
Trauma patient - Assessment Physical examination : n Head n n n n lacerations Contusions Facial fractures ear canal - nasal leakage ( CSF – blood ) Spinous processes palpation Bowel / bladder incontinence Penile erection Occult injury ( abdomen – chest – extremities )
Neurologic evaluation n Level of conscious : n Glasgow coma scale Eyes open n Best verbal response n Best movement response n
Sensory examination
the nipple line (T 4) xiphoid process (T 7) umbilicus (T 10) Dermatomes inguinal region (T 12, L 1) The perineum and perianal region (S 2, S 3, S 4)
Motor examination
Motor examination
Reflexes Stretch reflexes: n Spinal shock = absent n Upper motor neuron lesion = hyperreflexia + spasticity + clonus n Lower motor neuron lesion = absent
Reflexes n Planter reflex : Babinski’s sign n Oppenheim’s sign n n Cremasteric reflex T 12 -L 1
Lesion level The most caudal segment with both sensory and motor function bilaterally
Complete / incomplete cord lesion? n n Complete : no motor/sensory function exist more than 3 segments below the site of injury. Incomplete : some neurologic function below it.
Just to remember !
Classification Central cord syn. Anterior cord syn. Posterior cord syn. Brown-Sequal syn.
Sacral sparing Continued function in the conus medularis = incomplete cord injury Assessment : n Perianal sensation n Toe flexion n Rectal sphincter
Spinal shock n n n After severe spinal cord injury A state of complete spinal Areflexia. Last for varying length of time. 99% within 24 hour. n Evaluation by : Testing the bulbocavernosus reflex ( S 3 – S 4 ) n Anal wink reflex n
Bulbocavernosus reflex Anal wink
Spinal shock n After injury : n No evidence of spinal function below the level of injury ( even bulbocavernosus reflex ) → no determination of completeness of injury n Return of bulbocavernosus reflex with no sacral sparing signs → complete lesion
Roentgenogram n Plain Xray : Routinely n Chest n Pelvis n Cervical spine <AP/Lateral> Poly trauma n <AP/Lateral> thoraco-lumbar spine film n n CT MRI
ER intervention n High dose intravenous methylprednisolone Within 8 hours = more significant improvement 30 mg/kg in 15 minutes → after 45 minutes → 5. 4 mg/kg/hr in the remained 23 hour Complications : Wound infection GI Haemorrhage
ER intervention n Osmotic diuretics Manitol n Low molecular weight dextran n Used in head trauma No clinical effectiveness in spinal cord injury
ER intervention n Cervical stabilization : Bilateral sand bag + taping n Philadelphia collar n Traction : n Gardner wells n Halo vest n
Taping
Philadelphia collar
Gardner-wells tongs
Halo vest orthosis
Thoraco-lumbar braces n n Jewett brace Custom-molded TLSO
Jewett brace
Full contact braces