RDS a case study By Nicole Stevens 1

RDS: a case study By: Nicole Stevens

1. Baby BJ • Antenatal hx: 26 yr old, G 2 P 1, previous LUSCS (breech); bld grp O +ve, serology neg. GDM on insulin; gestational ITP (platelets on day of delivery 82) • Delivery hx (30/7/12): 35 wks, APH, breech until 2/52 ago, decision to perform LUSCS, no labour. Pink liquor. • Baby: cried at 20 secs, then apnoeic, IPPV for 1 min, then good respiratory effort • Apgars 9 & 9. Birth weight: 2670 g

2. Baby BJ • For admission to SCN from theatre, Issues: • Prematurity • Risk of hypoglycaemia • ? RDS • Maternal ITP • Breech until late in pregnancy Plan: • Observe resp. status, aim Sa. O 2 above 88%; BSL at 1 hr, feed if able then (dependent on resp effort); otherwise IV insertion, 10% dextrose and antibiotics

3. Baby BJ • Admitted to SCN at 1840 hrs. Hep B, Vit K given • Initial Gas: p. H: 7. 136, PCO 2: 78. 9, HCO 3: 26. 6, BE: -2, Lactate: 1. 6; TBG: 1. 7. CRP: <3, FBE: NAD (plt: 200) Plan: • IV bung inserted, 10% dextrose commenced and 2 m. L/kg bolus given (recheck TBG in 30 mins) • Hypoglycaemia resolved and not an ongoing issue • IV antibiotics commenced (Benpen 12/24, 60 mg/kg & Gent 36/24, 5 mg/kg) • Commenced CPAP of 6 cm/H 2 O; Fi. O 2: 25% at 2000 hrs • NETS notified of baby on CPAP – keep for now • CPAP increased to 7 at 2245 hrs, grunting

4. Baby BJ • Remained stable in a CPAP of 7 overnight, • • • intermittent grunt and mild work of breathing. Fi. O 2 at 21 -23%. CXR and bloods done 1630 hrs (CRP 4. 7, FBE NAD, plt: 167) Reduced to CPAP of 6, in air Parents and sibling visiting Urine output at 1 m. L/kg/hr Overnight: increased WOB, ? Apnoeic episode, febrile, tachypnoeic, no increase in O 2 requirement
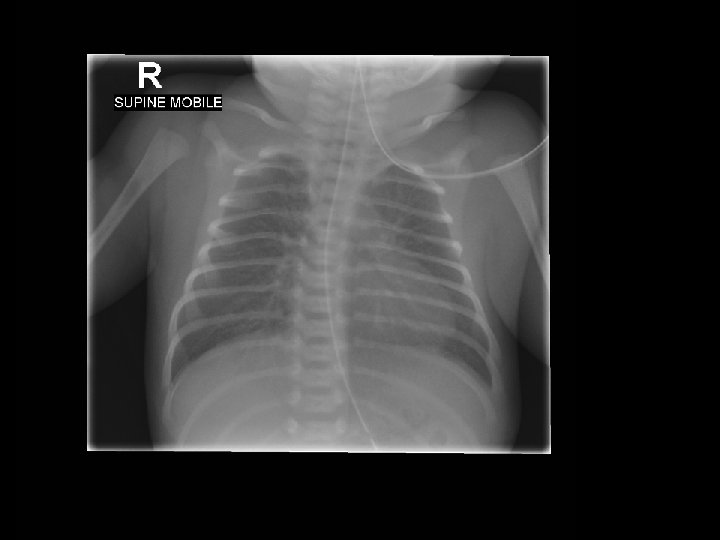
 • Bilateral but diffuse reticular granular densities")
6. XRAY interpretation (31/8/12 @ 1643 hrs) • Bilateral but diffuse reticular granular densities • Lungs do not appear hyperinflated • No pleural effusions • Heart is not enlarged • NG tube is noted, tip below L) hemidiaphragm Impression: findings would favour hilar membrane disease (RDS), with infection also in the differential
 • CPAP increased to 7 in the AM (Cap. G")
7. Baby BJ (1/7/12) • CPAP increased to 7 in the AM (Cap. G p. H: 7. 16, CO 2: 77) • Excessive handling around time gas collected, GNC, • • • bloods etc. CPAP reduced to 5 later in the afternoon, in air mild WOB (p. H 7. 34, p. CO 2 47) Generalised oedema noted; Urine output increasing (3. 5) Phototherapy commenced (SBR 158 at 40 hrs of age) OPos group, coombs neg Hungry, irritable at times, having small amounts of EBM as available for comfort, taking well. Had been febrile overnight (? Environmental), CRP 3. 0
 nd • Genta level taken prior to the 2")
8. Baby BJ (1/7/12 cont…) nd • Genta level taken prior to the 2 dose because of concerns regarding renal function (urine output still low in the morning when dose due, significant oedema still present and Na level 135) • Genta trough level: 1. 4 so dose withheld. Nursing issues: • Weigh nappies of babies on CPAP especially in first couple of days, once diuresis evident and baby stable consider discontinuing • Be mindful of renal function when giving genta as it is metabolised in the kidneys and levels may stay high.
 • Very unsettled 1700 hrs, crying++, not")
9. Baby BJ (1/7/12 cont. . ) • Very unsettled 1700 hrs, crying++, not able to settle. • • Very unsettled 1700 hrs, crying++, not able to settle. Increased WOB noted and slight O 2 requirement (25%) Asked paed to r/v Significant deterioration (colour change, desaturation, O 2 up to 100%) at approx. 1900 hrs, following an unsettled period. Registrar in attendance, transilluminated appeared to be a pnuemothorax, CXR attended to – confirmed pnuemothorax, consultant called. Preparation for insertion of intercostal catheter Morphine bolus given & sucrose given Pigtail catheter inserted by registrar at 1945 hrs
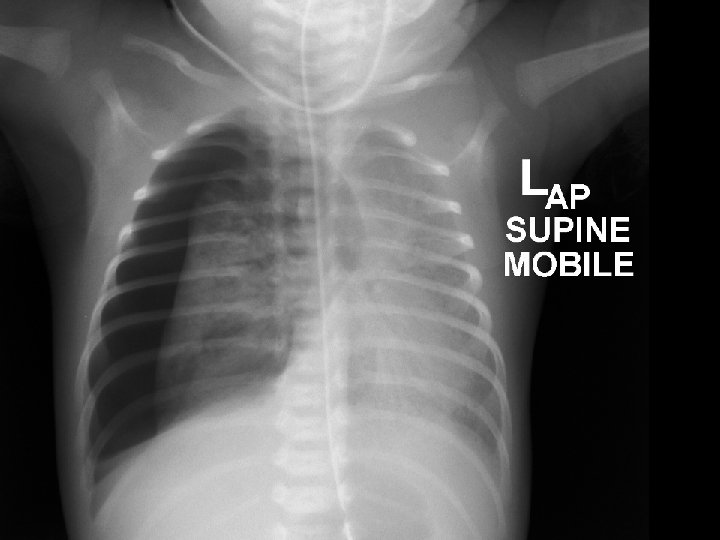
 • Large right sided pneumothorax • Displacement")
11. Xray interpretation (1/8/12 @ 1914 hrs) • Large right sided pneumothorax • Displacement of the mediastinal contents towards the left • Air space opacity in the left lung is increased likely to be due to a degree of compression from the pnuemothorax THIS BABY CLINICALLY VERY UNSTABLE, ALL HANDS ON DECK FOR ICC INSERTION!!
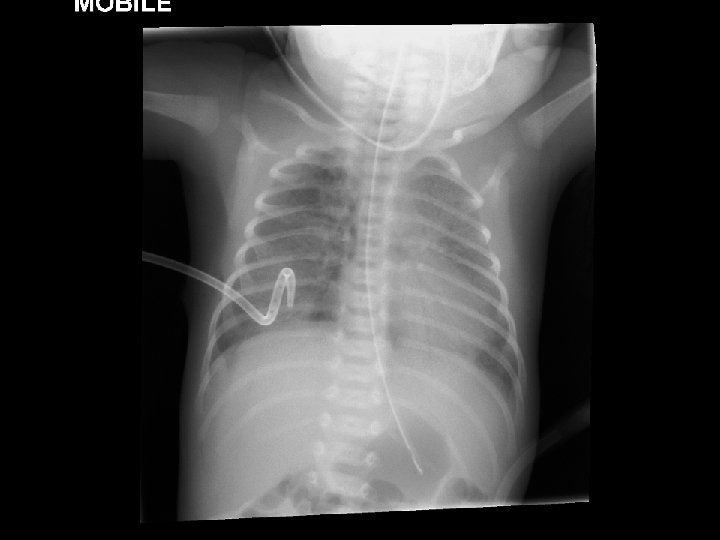
 R) pneumocath noted (pigtail catheter used)")
13. Xray interpretation (1/8/12 @ • 2006 hrs) R) pneumocath noted (pigtail catheter used) • No residual pneumothorax • Heart not enlarged, and cardiothymic contour • • normal NG tube seen with tip below the level of the diaphragm Bilateral air space opacities in both lungs are unchanged from previous SIGNIFICANT IMPROVEMENT INSTANTLY AS CHEST DRAIN INSERTED – AUDIBLE HISS HEARD!

14. Baby BJ • NETS called to retrieve, on their way • Gas (p. H 7. 17, CO 2 78) • 2205 hrs NETS arrived • Morphine infusion commenced • Still on CPAP, apnoeic episode when being examined by NETS doctor • Decision to intubate for safety for transport • Intubated/ventilated
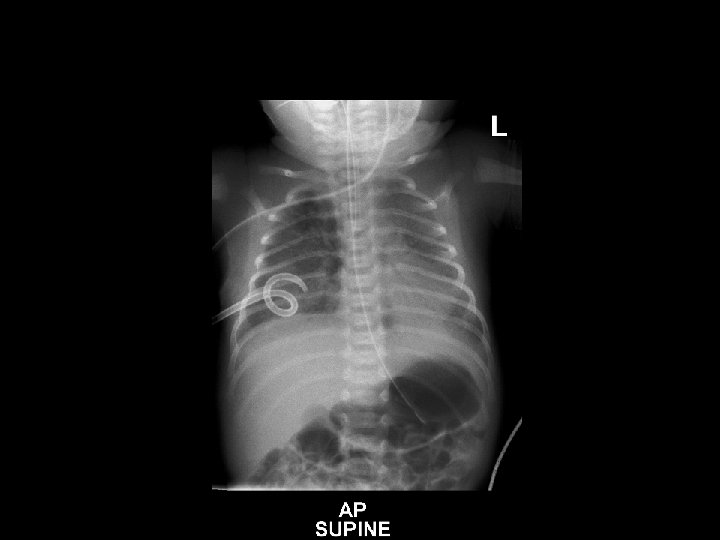
 • R) sided pleural catheter insitu •")
16. Xray interpretation (2/8/12 @ 0028 hrs) • R) sided pleural catheter insitu • Air space opacity in both lungs unchanged • ET tube is seen with tip at the level of the clavicle • NG tube is seen with tip below diaphragm • Heart size normal • No residual pneumothorax
: p. H: 7. 32, p. CO 2:")
17. Baby BJ • Gas (after intubation/ventilated): p. H: 7. 32, p. CO 2: 48, HCO 3: 25, BE: -1. 7, Lact: 2. 5 • Prepared for transport • Left at 0100 hrs Outcome: • Returned to BHS the next day, self ventilating in air, ICC out, NGT for feeds, IVT weaning. • Established feeds over the next 2 weeks and went home doing very well.

18. Pnuemothorax • Signs & symptoms • Diagnosis • Nursing management • Medical management

19. Signs & Symptoms • Irritability • Sudden deterioration with desaturation • Increase in respiratory distress • Diminished chest movements • Drop in blood pressure • Colour change • Blood gases may reflect hypoxia, respiratory and/or metabolic acidosis

20. Signs & Symptoms & diagnosis • Unequal or decreased air entry • Displaced apex beat • Transillumination (not always reliable especially in term/oedematous infants) • CXR will confirm diagnosis (but not always a quick turn around time to have performed)

21. Management Pain relief: • Oral sucrose • Infiltration of insertion site with 1% lignocaine before preparing and draping the field • IV morphine bolus and/or infusion In an emergency can do a needle aspiration: • 21 g butterfly needle, 3 way tap, 10 m. L syringe, alcohol swab, sterile gloves • Infant supine, insert over the top of the rib in the 2 nd or 3 rd intercostal space (mid clavicular). Aspirate air into syringe, expel using 3 way tap, repeat as required until air all removed.

22. Management • Following needle aspiration an ICC will need to be • • inserted for ongoing management See neonatal handbook, or own hospitals clinical practice guidelines for procedure instructions. Under controlled circumstances effort is generally made to perform the insertion in line with the auxilla (for cosmetic reasons). The ICC will need to be connected to a Heimlich valve or an underwater seal drainage set. Familiarise yourself with what equipment your units have because in a high anxiety situation you don’t want to be playing guessing games on what goes where!!

23. Nursing management • Have equipment ready to attach to ICC • Keep end sterile and hand to doctor when they are ready • • • to attacn Set suction as required if using underwater seal drainage (until water bubbling gently in chamber – may not need suction on to achieve this). Appropriate volume of water needs to be added to chamber as indicated in instructions. Continue with observations Ensure pain relief is adequate Counsel parents Handover to NETS nurse Copy appropriate paperwork for transfer
 www. netsvic. org. au/nets/handbook")
24. Reference • NETS handbook (pneumothorax drainage) www. netsvic. org. au/nets/handbook
- Slides: 25