Traumatic conditions of DorsoLumbar spine Anatomy of Thoracic

Traumatic conditions of Dorso-Lumbar spine
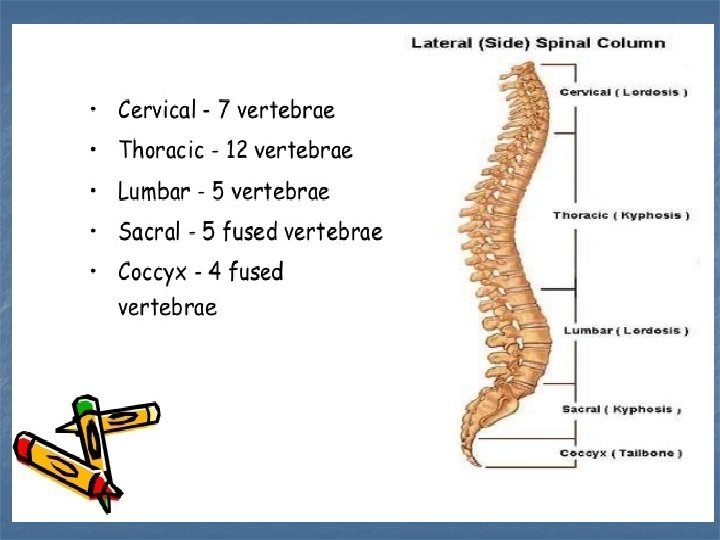


Anatomy of Thoracic Spine n n n Kyphosis is natural alignment Narrow spinal canal Facet orientation Rib factor on stability Conus at T 12 -L 1

Anatomy of Lumbar Spine n n Lordosis is natural alignment Larger vertebral bodies Facet orientation Cauda equina

Thoracolumbar Junction Transition Zone Kyphosis Lordosis Mechanical Difference: Lumbar spine less stiff in flexion

Transition Zone: Predisposed to Failure Little opportunity force dispersion Central loading of T-L junction Not anatomically disposed to transfer force

Patient Evaluation n Pre-hospital care n EMT personnel Initial assessment n Transport and immobilization n

Patient Evaluation n n ABC’s of Trauma History Physical Examination Neurological Classification

Clinical Assessment n n n Inspection Palpation Neurological Evaluation n n ASIA Impairment Scale Sensory Evaluation Motor Evaluation Reflex Evaluation n Bulbocavernosus, Babinski

Clinical Assessment n Associated Injuries Meyer, 1984 – 28% have other major organ system injuries n Noncontiguous spine fractures 3 -56% n Always monitor Hematocrit n GU: Foley recommended, check post-void residuals, if abnormal get cystometrogram n GI: prepare for ileus. n

Radiographic Evaluation n Trauma series includes: lateral cervical, chest, lateral thoracic, A/P and lateral lumbar and A/P pelvis n Obtunded patients require further skeletal survey n CT scan – bony injuries n MRI – images spinal cord, intervertebral discs, ligamentous structures

Thoracolumbar Fractures Controversies CLASSIFICATION!!!!! Indications for surgery Optimal time for surgery Best approach for surgery

CLASSIFICATION SYSTEMS Convey information Produce treatment plan Monitor patient progress Research tool

Böhler 1930 n Importance of injury mechanism n 6 types of spinal fractures included in system • • • Compression Flexion Extension Lateral flexion Shear Torsional

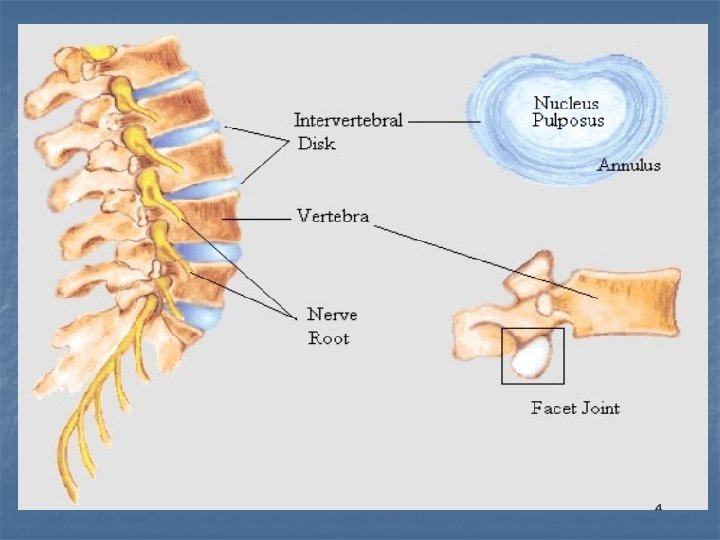
DENIS 3 Column Classification Anterior - Ant 1/3 of disc /VB + ALL Middle - Post 1/3 of disc/VB + PLL Posterior - Post Elements

• Six types Mc. Afee Classification • CT based-100 patients • Middle column most important

AO Mechanistic Classification Complex subdivisions to include most fractures

Spinal Cord Injury Accurately Document Neurological Status Remember SPINAL SHOCK Prognosis of deficit at 48 hours
 Motor(4")
Spinal Cord Injury FRANKEL A B C D E No motor Motor(2 -3) Motor(4 -5) Normal No sensation Min. sensation Sensation Normal

Spinal Cord Injury A. S. I. A. A Complete - no motor or sensation B Incomplete - sensation, no motor C Incomplete - sensation, motor<3 D Incomplete - sensation, motor 3 E Normal

Spinal Cord Injury- Power MRC Grade 0 1 2 3 4 5 none visible contraction contracts, not against gravity contracts against gravity not resistance contracts against resistance normal

Treatment Spine Trauma Severity Score Determined by: n. Injury Morphology n. Neurology n. Ligamentous Integrity

Next Step - Direct TX Assign Points Conservative Surgery

Treatment n. Injuries with 3 points or less = non operative n. Injuries with 4 points=Nonop vs Op n. Injuries with 5 points or more = surgery

Non – Operative Treatment Options No treatment advice / restrict activity Spinal ‘immobilisation’ Bed rest Lumbar pillow / Log rolling Casting / Bracing Combination treatment

THE AIMS OF TREATMENT Prevent neurological deterioration Minimise spinal deformity Fracture healing Minimise complications Acceptable function

Complications Bed rest sequelae Respiratory compromise Worsening of deformity Neurological deterioration

THANK YOU
- Slides: 30